4 minute read
Lymphadenopathy in a Patient with Mucous Membrane Pemphigoid

The following is a synopsis of the article “Multidisciplinary approach to diagnosis and management of lymphadenopathy in a patient with mucous membrane pemphigoid: a case report,” which appears in the September/October issue of General Dentistry.
Read the full article here.
Autoimmune blistering diseases (AIBDs) are a group of disorders marked by autoantibodies that attack structural proteins on the skin and mucous membrane.(1) Mucous membrane pemphigoid (MMP), a type of AIBD, is a chronic and rare disease, more common in females and adults over the age of 60 years.(2,3) Autoantibodies in MMP specifically attack the basement membrane zone of the epithelium and epidermis. MMP primarily affects mucosal surfaces, and the oral mucosa is the most affected site.(4) The clinical presentation can vary from mild erosions and subepithelial blistering to more severe erosions, ulcerations, blindness, and strictures, which can be life-threatening.(1,2)
AIBDs can present concurrently with solid or hematologic malignancies. This concomitant finding is believed to be associated with paraneoplastic syndrome, and management typically requires a multidisciplinary approach. Turkstani et al describe the diagnosis and treatment of a patient previously diagnosed with MMP of the skin who was referred to an oral medicine clinic for evaluation of oral mucosal blisters and gingival bleeding of 8 months’ duration. Incidental findings during routine head and neck examination led to a diagnosis of mantle cell lymphoma (MCL), a frequently aggressive form of non-Hodgkin lymphoma.
Case Report
A 65-year-old woman presented to the oral medicine clinic with a prior diagnosis of MMP and an 8-month history of oral blisters and gingival bleeding. Four months prior, a dermatologist had prescribed a prednisone taper along with topical clobetasol gel for skin blisters and a rash affecting her face, neck, and arms.
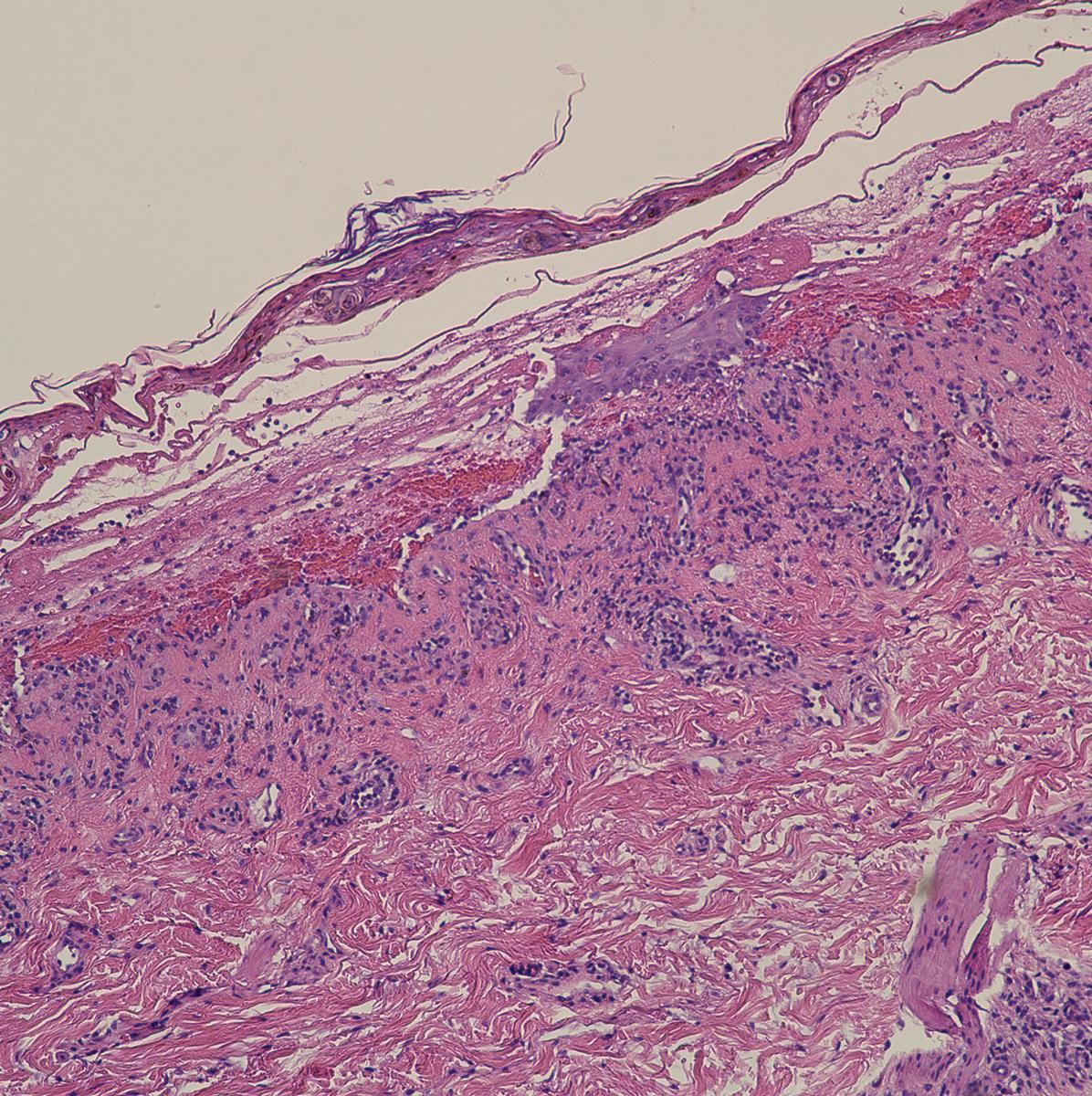
Based on history, clinical examination, and previous diagnosis from a skin biopsy, it was determined that the oral lesions were consistent with MMP. A review of systems revealed dysphagia, odynophagia, and nasal bleeding, and routine head and neck examination revealed a unilaterally large palatine tonsil. The clinical findings and results of computed tomographic imaging dictated a biopsy of the right tonsil, and immunohistochemical analyses of the biopsy specimen revealed markers consistent with MCL, which was later determined to be stage III (Figure).

The patient was prescribed dexamethasone and nystatin oral rinses to manage the MMP and prevent yeast infection from prolonged steroid use. For treatment of MCL, the hematology-oncology specialist prescribed a regimen of acalabrutinib, to be administered indefinitely, and rituximab, which would be administered for up to 24 months.
At the 3-month follow-up with the oral medicine clinic, the patient reported significant improvement. Her skin and oral blisters had cleared, and she was completely asymptomatic after starting the systemic treatment for MCL. It was recommended that she use the dexamethasone and nystatin rinses only as needed for flare-up of oral mucosal lesions.
Discussion
This case report, which to the best of the authors’ knowledge is the first reported case highlighting an instance of MMP associated with MCL, reinforces the importance of thorough, routine head and neck examinations by oral medicine specialists and all healthcare providers managing patients with AIBDs.
The paraneoplastic phenomenon of MMP is characterized by chronic mucosal erosions and fibrosis. It is typically triggered by an immune response to laminin 322 (LM-332) and is frequently associated with underlying malignancies such as B-cell chronic lymphocytic leukemia, non-Hodgkin lymphoma, and acute myeloid leukemia.(5) The risk of neoplastic association is substantially increased in MMP patients due to the presence of LM-332 autoantibodies, necessitating prompt investigation for underlying cancers.(5)
Summary
The incidental finding of hematologic malignancy in this patient underscores the importance of comprehensive, routine head and neck examinations in the assessment of patients with AIBDs. A multidisciplinary approach to management of AIBDs can lead to early detection of concurrent malignancies and improved patient outcomes.
Read the full article here.
References
Cowan TL, Huang C, Murrell DF. Autoimmune blistering skin diseases triggered by COVID-19 vaccinations: an Australian case series. Front Med (Lausanne). 2023;9:1117176. doi:10.3389/fmed.2022.1117176
Rashid H, Lamberts A, Borradori L, et al. European guidelines (S3) on diagnosis and management of mucous membrane pemphigoid, initiated by the European Academy of Dermatology and Venereology. I. J Eur Acad Dermatol Venereol. 2021;35(9):1750-1764. doi:10.1111/jdv.17395
Leisti P, Huilaja L, Jokelainen J, Varpuluoma O, Tasanen K. Epidemiology and comorbidities of mucous membrane pemphigoid: a national cohort study. J Invest Dermatol. 2024;144(9):2078-2080. doi:10.1016/j.jid.2024.02.008
Du G, Patzelt S, van Beek N, Schmidt E. Mucous membrane pemphigoid. Autoimmun Rev. 2022; 21(4):103036. doi:10.1016/j.autrev.2022.103036
Kartan S, Shi VY, Clark AK, Chan LS. Paraneoplastic pemphigus and autoimmune blistering diseases associated with neoplasm: characteristics, diagnosis, associated neoplasms, proposed pathogenesis, treatment. Am J Clin Dermatol. 2017;18(1):105-126. doi:10.1007/s40257-016-0235-z