CLINICAL/CASE STUDY
Multidisciplinary reconstruction of maxillary missing teeth Drs. Chris Wood and Cemal Ucer look at the multidisciplinary demands of complex cases
T
his case study demonstrates how a multidisciplinary and holistic approach is needed to provide a more satisfactory outcome to a complex restorative problem for the mutual benefit of both the patient and the treating dentist. As it is unusual for one clinician to develop expertise in all disciplines of advanced dental care, a multidisciplinary approach must be employed to explore an array of different options when looking to find the most optimum solution to a complex dental problem. Unfortunately, this could be difficult — particularly for the single-handed clinician who may not have in-house access to a multidisciplinary team. This article demonstrates how a more stable esthetic and functional solution was established by addressing all the key restorative requirements with a multidisciplinary dental team.
Initial presentation A middle-aged retired head teacher, who had previously been coping with an upper partial cobalt chrome denture, sought treatment when this denture fractured. He inquired about the availability of fixed or removable prosthodontics. He showed particular interest in dental implant options, as he no longer had the heavy professional pressures that had precluded him from receiving complex implant rehabilitation before his retirement. The patient presented with the situation shown in Figures 1-3. The initial examination revealed the following: 1. The patient was partially dentate in the upper arch (Kennedy Class IV Mod 2), which had been restored with a removable partial denture constructed in a cobalt chrome
framework. This prosthesis was less than ideal with disproportionately small denture teeth and a fracture through the acrylic component of the denture. 2. Class III skeletal and dental malocclusion. 3. Premaxillary disuse bone atrophy (Figure 4) due to absence of permanent teeth for many years — this enhanced the Class III skeletal appearance. 4. Patient had a desire for a fixed restorative solution if at all possible.
Preoperative assessment and treatment planning A full six-point periodontal assessment was carried out, which revealed no evidence of active periodontal disease although there had been some loss of attachment over the years. Investigations included a full assessment of the occlusion using study models mounted on a semi-adjustable articulator
with a facebow and “centric relation” record. Photographs were used to assist the treatment planning procedure and to communicate with and educate the patient. Dental wax was softened and gently applied to the buccal surface of the existing denture. This helped initially to evaluate how the “under contoured” lip support could be improved with treatment (Figure 5). Treatment options were discussed at length with the patient to ensure that proper informed consent was obtained prior to the onset of treatment. These included the following: 1. Treatment undertaken without orthodontic therapy and acceptance of Class III malocclusion: removable cobalt chrome-based partial denture or implant-retained overdenture 2. Treatment undertaken including orthodontic therapy to correct the Class III malocclusion: removable cobalt chrome-based partial denture or implant-retained overdenture.
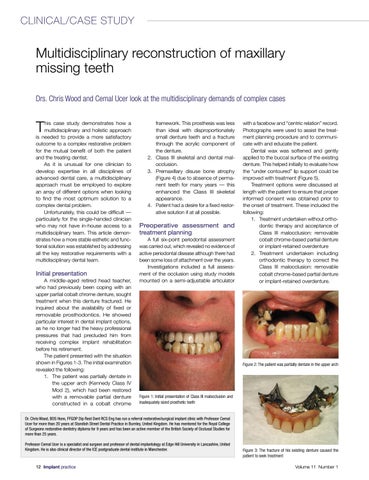
Figure 2: The patient was partially dentate in the upper arch
Figure 1: Initial presentation of Class III malocclusion and inadequately sized prosthetic teeth
Dr. Chris Wood, BDS Hons, FFGDP Dip Rest Dent RCS Eng has run a referral restorative/surgical implant clinic with Professor Cemal Ucer for more than 20 years at Standish Street Dental Practice in Burnley, United Kingdom. He has mentored for the Royal College of Surgeons restorative dentistry diploma for 9 years and has been an active member of the British Society of Occlusal Studies for more than 25 years. Professor Cemal Ucer is a specialist oral surgeon and professor of dental implantology at Edge Hill University in Lancashire, United Kingdom. He is also clinical director of the ICE postgraduate dental institute in Manchester.
12 Implant practice
Figure 3: The fracture of his existing denture caused the patient to seek treatment Volume 11 Number 1