TEXAS DENTAL

October 2022
2022 Legislative Landscape The Council on Legislative, Regulatory, and Governmental Affairs Help DENPAC Help You Meet the TDA Legislative Team Political Process 101 How A Bill Becomes A Law in Texas The Texas State Board of Dental Examiners — Regulating the Profession Texas Dental Association: The Premier Advocate for Medicaid & CHIP Special Investigative Units Your Insurance Advocate TDA Legislative Resource Guide

578 Texas Dental Journal | Vol 139 | No. 10 We’ll Take Care of Your Health Insurance. What’s the real difference between purchasing insurance through TDA Financial Services Insurance Program and somewhere else? You’ll always have attentive customer service from a team dedicated to TDA members and staff with TDA Financial Services Insurance Program. We work to make insurance easier for you and your staff. Go to our portal to review, compare, and buy your health insurance Sign up for coverage effective Jan. 1 through the portal. 2023 rates will be available on Nov. 1 Portal at TDAmemberinsure.com For more information, call 800-677-8644 Enroll or learn more at tdamemberinsure.com Open Enrollment Begins Nov. 1
Anesthesia Education & Safety Foundation
New TSBDE requirement of Pain Management
Two programs
(counts
(satisfies
be
Principles of Pain Management
Fulfills rule 104.1 for all practitioners
and
or Online (at your convenience)
(ask Dr. Canfield) for a bundle of 2 programs:

Use and Abuse of Prescription Medications and Provider Prescription Program
Fulfills rules 104.1 and 111.1
SEDATION & EMERGENCY PROGRAMS:
Nitrous Oxide/Oxygen Conscious Sedation Course for Dentists:
Credit: 18 hours lecture/participation (you must complete the online portion prior to the clinical part) Level 1 Initial Minimal Sedation Permit Courses:
*Hybrid program consisting of Live Lecture and online combination Credit: 20 hours lecture with 20 clinical experiences
SEDATION REPERMIT PROGRAMS: LEVELS 1 and 2
LIVE WEBCAST AND IN CLASS) ONLINE LEVEL 3 AND 4 SEDATION RE PERMIT AVAILABLE!
Anesthesia Programs
Class,
and
American Heart Association Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) Initial and Renewal Programs NOTE: ACLS or PALS Renewal can be completed by itself at any combined program

Combined ACLS-PALS-BLS

WEBCASTING and ONLINE RENEWALS AVAILABLE! Live and archived webcasting to your computer in the comfort of your home. Here are the distinct advantages of the webcast (contact us at 214 384 0796 to see which courses are available for webcast):
1. You can receive continuing education credit for simultaneous live lecture CE hours. 2. There is no need to travel to the program location. You can stay at home or in your office to view and listen to the cou rse. 3. There may be a post-test after the
www.tda.org | October 2022 579
Two ways to register: Call us at 214 384 0796 or e mail us at sedationce@aol.com Visit us on the web: www.sedationce.com NOW Available: In Office ACLS & PALS renewals; In Office Emergency Program Live Programs Available Throughout Texas Approved PACE Program Provider FAGD/MAGD Credit. Approval does not imply acceptance by a state of provincial board of dentistry or AGD endorsement. 8/1/2018 to 7/31/2022 Provider ID# 217924 Two ways to Register for our Continuing Education Programs: e-mail us at sedationce@aol.com or call us at 214-384-0796 OUR GOAL: To teach safe and effective anesthesia techniques and management of medical emergencies in an understandable manner. WHO WE ARE: We are licensed and practicing dentists in Texas who understand your needs, having provided anesthesia continuing education courses for 34 years. The new anesthesia guidelines were recently approved by the Texas State Board of Dental Examiners. As practicing dental anesthesiologists and educators, we have established continuing education programs to meet these needs. Dr. Canfield
available
rules 104.1
111.1) Live Webcast
as in-class CE)
All programs can
taken individually or with a special discount pricing
(ONLINE,
(Parenteral Review) Level 3 or Level 4
(In
Webcast
Online available):
and Level 2, 3 and 4 Program
online course concludes, so you will receive immediate CE credit for attendance 4. With the webcast, you can enjoy real-time interaction with the course instructor, utilizing a question and answer format OUR MISSION STATEMENT: To provide affordable, quality anesthesia education with knowledgeable and experienced instructors, both in a clinical and academic manner while being a valuable resource to the practitioner after the programs. Courses are designed to meet the needs of the dental profession at all levels. Our continuing education programs fulfill the TSBDE Rule 110 practitioner requirement in the process to obtain selected Sedat ion permits. AGD Codes for all programs: 341 Anesthesia & Pain Control; 342 Conscious Sedation; 343 Oral Sedation This is only a partial listing of sedation courses. Please consult our www.sedationce.com for updates and new programs. Two ways to Register: e-mail us at sedationce@aol.com or call us at 214-384-0796
contents
LEGISLATIVE OVERVIEW
Matt Roberts
THE COUNCIL ON LEGISLATIVE, REGULATORY, AND GOVERNMENTAL AFFAIRS
HELP DENPAC HELP YOU
MEET THE TDA LEGISLATIVE TEAM
POLITICAL PROCESS 101
HOW A BILL BECOMES A LAW IN TEXAS
THE TEXAS STATE BOARD OF DENTAL EXAMINERS — REGULATING THE PROFESSION
TEXAS DENTAL ASSOCIATION: THE PREMIER ADVOCATE FOR MEDICAID & CHIP
SPECIAL INVESTIGATIVE UNITS
YOUR INSURANCE ADVOCATE
TDA LEGISLATIVE RESOURCE GUIDE
Editorial Staff
Jacqueline M. Plemons, DDS, MS, Editor
Paras B. Patel, DDS, Associate Editor
Nicole Scott, Managing Editor
Barbara Donovan, Art Director
Lee Ann Johnson, CAE, Director of Member Services
Editorial Advisory Board
Ronald C. Auvenshine, DDS, PhD
Barry K. Bartee, DDS, MD
Patricia L. Blanton, DDS, PhD
William C. Bone, DDS
Phillip M. Campbell, DDS, MSD
Michaell A. Huber, DDS
Arthur H. Jeske, DMD, PhD
Larry D. Jones, DDS
Paul A. Kennedy Jr, DDS, MS
Scott R. Makins, DDS, MS
Daniel Perez, DDS
William F. Wathen, DMD
Robert C. White, DDS
Leighton A. Wier, DDS
Douglas B. Willingham, DDS
The Texas Dental Journal is a peer-reviewed publication.
Established February 1883 • Vol 139 | No. 8
Texas Dental Association
1946 S IH-35 Ste 400, Austin, TX 78704-3698
Phone: 512-443-3675 • FAX: 512-443-3031
Email: tda@tda.org • Website: www.tda.org
Texas Dental Journal (ISSN 0040-4284) is published monthly (one issue will be a directory issue), by the Texas Dental Association, 1946 S IH-35, Austin, TX, 78704-3698, 512-443-3675. Periodicals Postage Paid at Austin, Texas and at additional mailing offices. POSTMASTER: Send address changes to TEXAS DENTAL JOURNAL, 1946 S IH 35, Austin, TX 78704. Copyright 2022 Texas Dental Association. All rights reserved.
Board of Directors
Texas Dental Association
PRESIDENT Duc “Duke” M. Ho, DDS 281-395-2112, ducmho@sbcglobal.net
PRESIDENT-ELECT Cody C. Graves, DDS 325-648-2251, drc@centex.net
PAST PRESIDENT Debrah J. Worsham, DDS 936-598-2626, worshamdds@sbcglobal.net
VICE PRESIDENT, SOUTHEAST Glenda G. Owen, DDS 713-622-2248, Dr.owen@owendds.com
VICE PRESIDENT, SOUTHWEST Carlos Cruz, DDS 956-627-3556, ccruzdds@hotmail.com
VICE PRESIDENT, NORTHWEST Teri B. Lovelace, DDS 325-695-1131, lovelace27@icloud.com
VICE PRESIDENT, NORTHEAST Elizabeth S. Goldman, DDS 214-585-0268, texasredbuddental@gmail.com
SENIOR DIRECTOR, SOUTHEAST Shailee J. Gupta, DDS 512-879-6225, sgupta@stdavidsfoundation.org
SENIOR DIRECTOR, SOUTHWEST Richard M. Potter, DDS 210-673-9051, rnpotter@att.net
SENIOR DIRECTOR, NORTHWEST Summer Ketron Roark, DDS 806-793-3556, summerketron@gmail.com
SENIOR DIRECTOR, NORTHEAST Jodi D. Danna, DDS 972-377-7800, jodidds1@gmail.com
DIRECTOR, SOUTHEAST Laji J. James, DDS 281-870-9270, lajijames@yahoo.com
DIRECTOR, SOUTHWEST Krystelle Anaya, DDS 915-855-1000, krystelle.barrera@gmail.com
Case
of
Annual subscriptions: Texas Dental Association members $17. Instate ADA Affiliated $49.50 + tax, Out-of-state ADA Affiliated $49.50. In-state Non-ADA Affiliated $82.50 + tax, Out-of-state Non-ADA Affiliated $82.50. Single issue price: $6 ADA Affiliated, $17 Non-ADA Affiliated, September issue $17 ADA Affiliated, $65 Non-ADA Affili ated. For in-state orders, add 8.25% sales tax. Contributions: Manuscripts and news items of interest to the membership of the society are solicited. Electronic submissions are required. Manuscripts should be typewritten, double spaced, and the original copy should be submitted. For more information, please refer to the Instructions for Contributors statement printed in the September Annual Membership Directory or on the TDA website: tda. org. All statements of opinion and of supposed facts are published on authority of the writer under whose name they appear and are not to be regarded as the views of the Texas Dental Association, unless such statements have been adopted by the Association. Articles are accepted with the understanding that they have not been published previously. Authors must disclose any financial or other interests they may have in products or services described in their articles.
Advertisements: Publication of advertisements in this journal does not constitute a guarantee or endorsement by the Association of the quality of value of such product or of the claims made of it by its manufacturer.
DIRECTOR, NORTHWEST Stephen A. Sperry, DDS 806-794-8124, stephenasperry@gmail.com
DIRECTOR, NORTHEAST Mark A. Camp, DDS 903-757-8890, macamp1970@yahoo.com
SECRETARY-TREASURER*
Carmen P. Smith, DDS 214-503-6776, drprincele@gmail.com
SPEAKER OF THE HOUSE*
John W. Baucum III, DDS 361-855-3900, jbaucum3@gmail.com
PARLIAMENTARIAN**
Glen D. Hall, DDS 325-698-7560, abdent78@gmail.com
EDITOR** Jacqueline M. Plemons, DDS, MS 214-369-8585, drplemons@yahoo.com
LEGAL COUNSEL
Carl R. Galant
*Non-voting member
**Non-voting
580 Texas Dental Journal | Vol 139 | No. 10
FEATURES 586 2022 Legislative Landscape 586
Dr
596
598
600
602
604
610
618
625
627
630
editorials 581 Editor’s Letter 584 President’s Message HIGHLIGHTS 634 Oral and Maxillofacial Pathology Case
the Month 637 Calendar of Events 638 Value for Your Profession: 2023 Open Enrollment and ACA Update 643 Pathology
Diagnosis and Management 644 Advertising Briefs 650 Index to Advertisers
Editor’s Letter
Fall is finally here! I can’t remember a time when the unrelenting heat of a summer in Texas has made me really yearn for cooler weather. Change is in the air—students are back in school, and life takes on a more comfortable routine. For me, it’s often a time when I not only prepare for teaching but look at what’s working and not working in my practice with a goal of improving quality of care and optimal efficiency.
From conferences to workshops and mentoring to sharing case studies, there is no way to overestimate the importance of learning from the people around us. When we’re open to learning from others, we benefit from their experiences incorporating those into our own allowing us to improve and grow. Collaboration and sharing details of techniques and procedures among colleagues makes learning twice as rich. While the practice of dentistry can feel a little isolating at times, it’s comforting to realize we don’t have to acquire all knowledge on our own.
I’d be willing to bet that most of us have “perfected” certain techniques and procedures we perform in a way not necessarily described in the “instructions for use” or “suggested protocols.”
Following these “discoveries”, I find myself most excited and proud of my work. And I want to share!
Tips of the trade are often “clever or ingenious skills, techniques or methods used by professionals to do something more easily or efficiently” and can be shared through one-on-one training, group sessions, an internal web site, or even a department newsletter. The Texas Dental Journal is a great place to share your discoveries.
Consider submitting your cases that highlight specific techniques that are unique or have worked well for you in the past! What appear to be little modifications in a procedure can make a world of difference to other dentists. The publications team will be glad to provide you with assistance! Let us know your ideas—We are Listening!

www.tda.org | October 2022 581
Jacqueline Plemons, DDS MS
SmileCon Registration is Open

Scan to see the full session list on the Agenda Builder!Houston, TX Oct. 13–15, 2022
Our Smile Pass gives you access to 120+ courses, the Opening Session with Dr. Brené Brown, SmileCon Street Fest, Dental Central (the exhibit hall), the Closing Session, and more. Register today for this mighty meeting at SmileCon.org.
SMILECON is a trademark of
American
Association.
582 Texas Dental Journal | Vol 139 | No. 10
the
Dental







www.tda.org | October 2022 583 346-221-0316 713.486.4411 go.uth.edu/Pathology • Complimentary biopsy kits • Delivery via FedEx, local courier or USPS • Diagnosis within two business days of receiving most biopsy specimens. • UT M.D. Anderson Cancer Center and UTHealth Medical School available for consultations as needed. • Affiliated with UT School of Dentistry at Houston. Our Pathologists: Specializing in: • Conventional biopsy testing • Cytopathology • Histochemistry • Immunohistochemistry • Direct immunofluorescence testing Jerry E. Bouquot, DDS, MSD Ngozi N. Nwizu, BDS, MMSc, PhD Kalu U.E. Ogbureke, BDS, DMSc, JD, MSc Nadarajah Vigneswaran, DMD, DrMedDent
Dentist to Dentist
RELATIONSHIP. MENTORSHIP. COMMUNICATION.
It’s early on in my presidential year, and I’ve had an amazing time meeting with members, non-members, and students —listening to their stories, thoughts and concerns about a myriad of issues. This journey started in Amarillo, extended to El Paso and their new school, which is amazing, and will soon ramp up to include visits to San Antonio, Houston, Dallas, Austin, and McAllen before the end of the year.
This upcoming year is an important one, as it is the lead for the 88th Session of the Texas Legislature. Within this month’s Texas Dental Journal, you will find a comprehensive update on our upcoming legislative session, including the current climate of the legislature, what our team is working on and what is needed from each of us to ensure a successful year. As importantly, updates throughout the session can be found in “The Root,” which will include how our agenda is progressing along with all issues that might affect each of us practicing.
Legislative Agenda
Although not comprehensive, highlights of our legislative agenda this year will include:
• An insurance bill that will seek to address network leasing, disallowables (the practice of not being able to bill patients even when the procedure performed
is a non-covered service) and retroactive denials.
• Seeking increases in Medicaid reimbursements (the last increase was in 2007).
• Funding for the Dental Education Repayment Program which incentivizes young dentists with high debt to practice in underserved areas.

Regulatory and Compliance Questions with Diane
Have you or anyone you’ve known posted dental compliance and regulatory practice questions on social media resulting in 20 different (and often wrong) answers? Questions like:
• Why can’t I bill the patient’s insurance for some non-covered procedures?
• How many dentists are allowed to oversee hygienists in a single practice?
• Do I have to take a controlled substances CE course if I don’t prescribe narcotics?
Perhaps one of the best-known but quietly hidden gems of the Texas Dental Association is our own Senior Policy Manager Ms Diane Rhodes, who has started an online resource titled, “Ask Diane”, to help answer many questions that deal with compliance and regulatory landmines. Diane has been
Duc “Duke” M. Ho, DDS, FAGD TDA President
with the Association for over 20 years and has an almost incomprehensible wealth of knowledge regarding legislative statutes and Board rules.
So, if you have questions, or see questions online that you suspect need the right answer, just call out, “Ask, Diane”.
Member Money Matters
Lastly, I suspect that you’re probably tired of me mentioning the Employee Retention Credit but there has not been a more direct means of getting money to our members than through our TDA Perks endorsed vendor: ERC Specialist. To date, over 400 practices have received monies totaling over $9 million—and it is likely many of your friends have received money. The application is free and the window is slowly closing, so don’t wait much longer.
584 Texas Dental Journal | Vol 139 | No. 10


www.tda.org | October 2022 585 586 596 598 600 602 604 610 618 625 627 630 2022 Legislative Landscape Dr Matt Roberts The Council on Legislative, Regulatory, and Governmental Affairs Help DENPAC Help You Meet the TDA Legislative Team Political Process 101 How A Bill Becomes A Law in Texas The Texas State Board of Dental Examiners — Regulating the Profession Texas Dental Association: The Premier Advocate for Medicaid & CHIP Special Investigative Units Your Insurance Advocate TDA Legislative Resource Guide 2022 LEGISLATIVE Landscape Contents www.tda.org | October 2022 585
2022
Legislative Landscape

586 Texas Dental Journal | Vol 139 | No. 10
Dr Matt Roberts, Chair TDA Council on Legislative, Regulatory, and Governmental Affairs
INTRODUCTION
Each October, the Texas Dental Journal focuses its attention on organized dentistry’s efforts in the legislative and regulatory arenas. Much of what dentists do every day in their practices is controlled by the Texas legislature, made up of 150 members of the Texas House of Representatives and 31 members of the Texas Senate. The Texas State Board of Dental Examiners (TSBDE), made up of 11 members, including 6 dentists, 3 dental hygienists, and 2 members of the public, also plays a significant role in regulating dentistry in Texas. Texas statewide officials—including the governor, lieutenant governor, attorney general, and comptroller—also have roles in the oversight and regulation of dentistry.
The practice and regulation of dentistry and dental hygiene are governed in state statute by the Dental Practice Act (DPA) contained in the Texas Occupations Code. The DPA commits almost 20 chapters with over 200 sections to the practice and oversight of dentistry. The TSBDE is charged with interpreting and enforcing the DPA and the other statutes affecting dentistry, as well as implementing rules to protect public health and safety.
Given the depth and complexity of the laws, regulations, and oversight of dentistry, it is imperative that the TDA commit adequate resources and personnel toward ensuring our voice is not only present but heard in all legislative and regulatory forums where dentistry is considered.
The TDA’s Council on Legislative, Regulatory, and Governmental Affairs (or CLRA) is made up of TDA member dentists from around the state who have experience and expertise in the legislative and regulatory fields. CLRA is charged with working with the legislature and the regulatory entities to represent the Association and implement its policies as set by the House of Delegates and Board of Directors. The TDA legislative “team” (the TDA Department of Legislative and Regulatory Affairs staff and legislative consultants) works closely alongside CLRA members and the TDA leadership to assist with achieving organized dentistry’s goals.
The 88th Session of the Texas Legislature convenes in January 2023. It should be “back to normal” in terms of doing most of the business faceto-face; the previous session was often virtual due to the pandemic. It is safe to say that the 87th session was one of the more atypical in history because of the many health and safety protocols put in place.
With the 2022 primary election behind us, the membership makeup of the Texas Senate and Texas House for next session is becoming more defined. At the time of this writing, there will be at least 6 new members in the Texas Senate and at least 27 new members in the Texas House. Turnover at the Capitol is normal but numbers that large are not.
www.tda.org | October 2022 587
The general election is in November, and it is possible that a few more seats could change as well. As a reminder, the redistricting process in Texas generally results in districts being drawn to favor one party over the other, so close races in the general election are the exception not the rule. In any case, there will be a significant number of new lawmakers at the Texas Capitol next session. The TDA team is working to create relationships and educate the incoming lawmakers and staff.
Regarding over-arching issues the legislature will face next session, the budget will be top priority. Per the Texas Constitution, lawmakers must pass a balanced budget every 2 years. Unlike sessions of the recent past, there will be a budget surplus for the next biennial budget. The legislature will have roughly $26 to $28 billion in additional funds to work with. The legislature is not required to spend all the money available; some could be deposited into the “rainy day fund” which is a savings account for the state. The TDA will pursue additional state dollars to vital oral health programs. These will be discussed later in this article.
There are other priority issues the legislature will face next session including school safety, mental health, firearms, women’s health, border security, education, transportation, water, public health, and access to health care to name just a few. Collectively, these issues, and more, will dominate a majority of the legislature’s limited time.
The TDA will have its own agenda at the Capitol and will compete against these issues for lawmakers’ time. There will be hundreds of other stakeholders at the Capitol doing the same thing.
As it is every session, it will be a mad dash from the moment lawmakers gavel in to the moment they gavel out. With only 140 days to work with, time during session is both your enemy and your friend; enemy when working to pass legislation, friend when working to kill legislation.
Your TDA team will work around the clock to represent the membership and accomplish the many goals of the Association.
The remainder of this article will provide an overview of the Texas Legislature and summarize the TDA’s legislative agenda for the 88th session.

On behalf of CLRA and the legislative team, thank you for being a member of the Texas Dental Association and enjoy this issue of the Journal
If your TDA legislative team can be of any assistance to you, please do not hesitate to contact me, Jess Calvert, Diane Rhodes, or Staci Rives in the legislative department.
588 Texas Dental Journal | Vol 139 | No. 10
TEXAS LEGISLATURE—OVERVIEW
The Texas Legislature is the chief policymaking branch of state government that the Texas Constitution vests with all legislative power in the state. It is a bicameral body composed of an upper chamber, the Texas Senate, and a lower chamber, the Texas House. The 181 members of the legislature are elected from districts throughout the state (31 senators, 150 representatives). The legislature enacts thousands of laws each session that govern the conduct of persons and businesses, allocate resources, and define the duties of government institutions. The only bill lawmakers are constitutionally required to pass, however, is the biennial state budget.
In addition to legislative powers, the legislature exercises other types of authority. Constituent powers include the ability to alter the state Constitution, and members have authority to exercise powers of attorney on behalf of their constituents. The legislature is also allowed by statute to create and regulate the state’s administrative system, which comprises boards, commissions and departments that oversee state agencies. The legislature establishes and funds the departments and agencies—such as the TSBDE—and defines their powers and functions.

TEXAS LEGISLATIVE SESSIONS
The Texas Constitution limits the regular legislative session to a maximum of 140 days every 2 years, but the governor has authority to call a special session when necessary. Regular sessions begin on the second Tuesday of January in odd-numbered years. Special sessions are limited to 30 days each and are limited to a specific “call,” or subject matter, determined by the governor.
TERMS OF OFFICE —TEXAS HOUSE AND SENATE
House members serve 2-year terms. To qualify to run for the office, representatives must be at least 21 years old, have been Texas residents for at least 2 years and residents of the district they wish to represent for at least 1 year. There is no limit on the number of terms a member can be re-elected.
Senate members are elected to 4-year terms. To run for Texas Senate, candidates must be at least 26 years old, have been residents of Texas for 5 years preceding their election and residents of the district they are seeking for at least 1 year.
TEXAS SENATE, TEXAS HOUSE—MEMBERSHIP
Each election cycle brings forth change. Members of the Senate and House change each cycle—voluntarily or involuntarily. As previously mentioned, in the Texas House, there will be at least 27 new members and, in the Texas Senate, at least 7 new members.
Consistency at the Capitol is advantageous. The TDA team knows every lawmaker and their staff, they know where they are in terms of leadership and seniority, what committees they chair, what committees they are appointed to, their positions on oral health issues, etc. When members leave, there are unknowns.
There will be significant change and unknowns in the 88th. The TDA, along with all other stakeholders, will contend with this shake-up.
www.tda.org | October 2022 589
88th Legislative Session —
590 Texas Dental Journal | Vol 139 | No. 10
— TDA Agenda
ACCESS TO ORAL HEALTH CARE
Increasing access to oral health care is always a top priority of the TDA. The state must adequately fund programs and public health initiatives that provide dental care and oral health awareness and education to Texans.
Medicaid Dental—Funding
Medicaid dental has not received an increase in funding since 2007. Rates have remained the same for almost 16 years despite the ever-increasing costs of providing care.
Adequate Medicaid dental reimbursement rates are a crucial component of sustaining a viable Medicaid dental program and providing access to care to millions of Texans who cannot otherwise afford it. Rates must be fair for dentists to participate in the program and treat patients.
The TDA will advocate for additional funding to the Medicaid dental program in the 88th session.
Texas Dental Schools—Funding
It is the policy of the TDA to support the mission of state-funded, universitybased dental schools which is to educate students to serve their patients and communities.
Texas dental schools train a diverse group of future clinicians for important roles in Texas’ oral health care workforce, improving the oral health of individuals and communities throughout the state.
The state provides much of the funding to the dental schools. State funding to the schools must be adequate to ensure they can continue to operate their dental clinics and educate and train the state’s dental workforce.
State funding must also be at a level that that does not unfairly place much of the cost burden on students leaving them with unmanageable debt upon graduation. The balance between state funding and student cost must be fair.
The TDA will continue to partner with the dental schools next session to increase state funding to them.
www.tda.org | October 2022 591
Oral Health Improvement Program—Funding

Failure to treat dental disease has serious economic and medical consequences. The Oral Health Improvement Program, or OHIP, at the Texas Department of State Health Services conducts oral health surveillance and administers schoolbased preventive dental clinics and the Smiles for Moms and Babies program.
The OHIP was virtually dismantled in 2003 due to budget constraints. Funding dropped from approximately $3.1 million in fiscal year 2002 to $1.2 million in fiscal year 2005. Additional funding is needed to ensure that the OHIP has the resources necessary to collect, analyze, and disseminate essential oral health data and implement a comprehensive education and promotion campaign focused on at-risk populations.
The TDA will work with the legislature in the 88th session to support additional funding to the OHIP and mandate that the dental director of the program be a Texas licensed dentist.
Dental Education Loan Repayment Program—Funding
The TDA successfully worked with lawmakers in 1999 to create the Dental Education Loan Repayment Program (DELRP). The goal of the program is to recruit and retain qualified dentists to provide care in areas of the state that are underserved.
Dentists participating in the DELRP agree to practice general or pediatric dentistry for a specific length of time in return for loan repayment assistance. Dentists in the program practice in Dental Health Professional Shortage Areas, approved practice sites including Community Health Centers and Federally Qualified Health Centers, or other practice locations serving populations that Texas determines to be critically underserved.
The participating dentists also agree to accept Medicaid and/or CHIP and not deny services based on a patient’s inability to pay. In return, the state provides financial compensation to assist with payment of student loans. Despite the success of the DELRP program, funding to it has been inadequate and inconsistent. In 2015, TDA successfully advocated for lawmakers to reinstate some funding. However, state budget challenges eliminated subsequent DELRP funding.
TDA strongly supports the DELRP and its goal which is to place dentists in areas of need/shortage to provide access to oral health care and address workforce distribution issues.
The TDA will work with lawmakers in the 88th session to restore the program’s funding and expand the program overall.
592 Texas Dental Journal | Vol 139 | No. 10
DENTAL INSURANCE REFORM
Dental insurance can often be confusing for both patients and dentists. Dentists report that one of the most challenging aspects of running a dental practice is dealing with third-party payors or insurance. These challenges often complicate and strain the dentist-patient relationship.

The TDA will work with lawmakers in the 88th session to address 3 key insurance issues affecting dentists and patients—retroactive denials, silent network leasing, and disallowable clauses in contracts.
Retroactive Denials
Dental insurers audit their claims payments for accuracy and efficiency, which is standard business practice. However, dentists and patients expect insurers to process dental claims, and address any inaccuracies, within a reasonable timeframe. When a carrier demands recovery of a paid claim 6 months or more after the care was provided, the dentist and patient are unduly burdened. In some cases, patients are left to pay for dental care they and their dentist thought was covered and already paid for by insurance. This places unexpected financial strain on the patient and can harm the relationship between the dentist and the patient.
The first component of TDA’s dental insurance legislation creates a reasonable time limit of 180-days for state-regulated insurers to seek recovery of a claim. It also gives dentists sufficient time to challenge or appeal the carrier’s recovery effort. This is consistent with similar statutes applicable to medical care claims.
Silent Network Leasing
State regulated dental insurers can currently sell or lease an existing provider network to another entity or carrier. These arrangements are often silent, occurring without the dentist’s knowledge or consent. The lack of transparency can lead to incorrect assumptions about treatment plans or insurance coverage, and unforeseen costs for patients. This can negatively impact the trust between patient and dentist.
The second component of TDA’s insurance legislation protects patients by requiring state-regulated insurance companies to conspicuously notify dentists when the insurance network can be sold or leased. This provides dentists an opportunity to review the contract and proactively decide whether to participate. In turn, patients can be more fully informed about the costs of care early in the health care transaction.
The bill also requires any third party who gains access to the network to comply with the original contract’s terms. These provisions will foster fairness between contracting dentists and insurance carriers and reduce the occurrence of surprise billing to patients following treatment.
www.tda.org | October 2022 593
Dental treatment is between a dentist and his or her patients. Dental benefits exist to help patients with the cost of dental care, not to determine the clinical decisions made by dentists and their patients.
It is also imperative that dentists can decline to participate in a network sale or lease without repercussions. In some Texas communities, a single dental practice may be the only practice accepting the insurance for a large employer. If a dentist’s refusal to participate in a leasing arrangement results in termination of other contracts, the dental practice could lose its in-network status with a major carrier. This could affect coverage for many existing patients.
TDA’s insurance legislation gives dentists the right to opt-out without negative repercussions to other contracts, which ensures continuation of care for patients.

Disallowables
Dental treatment is between a dentist and his or her patients. Dental benefits exist to help patients with the cost of dental care, not to determine the clinical decisions made by dentists and their patients.
Some dental carriers have steadily attempted to change that matrix and have become not only the payer, but also the arbiter of some clinical decisions. An example is the use of disallow clauses which can be found in some provider network agreements in place today.
This clause allows a carrier to both deny payment for a covered dental procedure and prohibit the doctor from collecting any fees associated with the services provided. Disallow clauses interfere with the doctor-patient relationship by selecting what types of procedures can be paid for. This places dentists in the unfair position of diagnosing and providing care that is necessary without being compensated for it.
The TDA will work with lawmakers in the 88th session to prevent disallowable clauses in state regulated dental insurance contracts.
SCOPE OF PRACTICE
Attempts are made each legislative session to expand the scope of practice of nondentists. TDA will oppose and work to defeat all legislative proposals exposing Texas dental patients to a lower standard of care by non-dentists.
TDA is positioned well to represent the interests of the membership and ensure dentistry’s voice is heard. Thank you for your membership and for being an advocate for your patients and your profession.
594 Texas Dental Journal | Vol 139 | No. 10

THE COUNCIL ON LEGISLATIVE, REGULATORY, AND GOVERNMENTAL AFFAIRS
The Council on Legislative, Regulatory, and Governmental Affairs (CLRA) makes certain that the Texas Dental Association (TDA) has an effective voice in the legislative process and state government. CLRA works with the legislative and regulatory affairs staff and TDA contract legislative consultants to implement TDA’s legislative agenda and maintain positive working relationships with legislators, state officials, and allied professional groups. In conjunction with component societies, the council informs members about governmental actions and mobilizes the TDA’s grassroots organization. The council also works with regulatory agencies to help ensure a competitive marketplace for dentists and quality dental care for all Texans.
Dr Matthew B. Roberts, Chair General dentist from Crockett, former TDA president, current member of the American Dental Association (ADA) Council on Government Affairs, former member of the ADA Council on Access, Prevention and Interprofessional Relations, and former member of the Commission on Dental Accreditation. Dr Roberts is serving his 19th year on CLRA.
Dr Jay C. Adkins, Member General dentist from Lubbock, former TDA Board of Directors member, former member of the Texas State Board of Dental Examiners Dental Hygiene Advisory Committee, current TDA Smiles Foundation Board member (18th year), and current regent for Texas in the International College of Dentists. Dr Adkins is serving his 11th year on CLRA.
Dr Paul A. Kennedy III, Member Pediatric dentist from Corpus Christi, former assistant professor of the Department of Pediatric Dentistry at the University of Texas Health Science Center at San Antonio School of Dentistry, and past president of the Nueces Valley District Dental Society. Dr Kennedy is serving his 5th year on CLRA.
Dr Lee P. Oneacre, Member Oral surgeon from Carrollton, former TDA Board of Directors member, former Dallas County Dental Society president, and former member of the ADA Council on Access, Prevention and Interprofessional Relations. Dr Oneacre is serving his 16th year on CLRA.
Dr Cody C. Graves, PresidentElect General dentist from Goldthwaite, third generation dentist, former TDA Board of Directors member (7 years), ADA and TDA delegate, former chair of the TDA Budget and Finance Committee, former president of the 21-B District. Dr Graves is serving his 1st year on CLRA.
Dr Debrah Worsham, Past President
General dentist from Center, current TDA past-president, former DENPAC chair, former ADPAC vice-chair, former TDA Board of Directors member. Dr Worsham is serving her 20th year on CLRA.
Dr Melissa Uriegas, New Dentist
General dentist from McAllen, current DENPAC representative, former Trustee for the National Hispanic Dental Association, former participant of the ADA’s Institute for Diversity in Leadership, TDA delegate. Dr Uriegas is serving her 1st year on CLRA.
Dr David A. Duncan, Consultant
General dentist from Amarillo, former TDA president, former TDA Board of Directors member, former Panhandle Dental Society president, former member of the ADA Council on Dental Practice, former member ADA’s political action committee (ADPAC). Dr Duncan is serving his 13th year on CLRA.
Dr Michael Najera, Consultant Periodontist from El Paso, former president of the 16th District, current chair Legislative Action Committee of the 16th District, current DENPAC board member and chair of 16th District for past 16 years, past TDA and ADA delegate. Dr Najera is serving his 3rd year on CLRA.
Dr Mark Peppard, Consultant General dentist from Austin, served on the ADA’s political action committee (ADPAC), former TDA Board of Directors member, former TDA delegate, former ADA delegate, current DENPAC board member. Dr Peppard is serving his 17th year on CLRA.
Dr R. Lee Clitheroe, DENPAC General dentist from Sugar Land, current DENPAC chair, former TDA vice president, current member of the Greater Houston Dental Society (GHDS) Foundation Board, current chair of the GHDS Legislative Action Committee, ICD and ACD fellow, and adjunct faculty at the University of Texas School of Dentistry at Houston. Dr Clitheroe is serving his 2nd year on CLRA.
Ms Julia Martin, Alliance of the TDA
From Arlington, she has held numerous offices in the Alliance of the Texas Dental Association (ATDA) and Alliance of the Fort Worth District Dental Society. She has been an Alliance member since 1985. Ms Martin is serving her 4th year on CLRA.
596 Texas Dental Journal | Vol 139 | No. 10
Row 1 (L-R)
Dr Matthew B. Roberts, Chair (Crockett)
Dr Jay C. Adkins (Lubbock)





Dr Paul A. Kennedy III (Corpus Christi)


Row 2 (L-R)
Dr Lee P. Oneacre (Carrollton)
Dr Cody C. Graves (Goldthwaite)
Dr Debrah Worsham (Center)
Row 3 (L-R)
Dr Melissa Uriegas (McAllen)

Dr David A. Duncan (Amarillo)
Dr Michael Najera (El Paso)
Row 4 (L-R)
Dr Mark Peppard (Austin)
Dr R. Lee Clitheroe (Sugar Land)


Ms Julia Martin (Arlington)

www.tda.org | October 2022 597
Help DENPAC

598 Texas Dental Journal | Vol 139 | No. 10
Help You
Dr R. Lee Clitheroe, Chair DENPAC
Dental insurance reform • Scope of practice

Dental school funding • Licensing
Teledentistry • Medicaid funding
Student loan relief • Taxation • Access to care
Each of these issues affects you, and they are all on the line every time the Texas Legislature meets. How are you going to effectively advocate for yourself? For your practice and your patients?
Thousands of bills are filed each session, with as many as a hundred bills coming before legislators on any given day for a vote. How are you going to keep track of everything going on? How are you going to determine whether a bill would help or hurt you? How are you going to communicate your concerns to the 181 members of the Texas Legislature?
You can’t do it alone, and the good news is you don’t have to. The Texas Dental Association provides a powerful, united voice for organized dentistry. Through TDA’s political arm, DENPAC, we can effectively advocate for you. But DENPAC can’t work without you! DENPAC uses voluntary donations from TDA members to contribute to election campaigns of state candidates who have demonstrated their concern for the preservation of dentistry as an independent profession, and for the dental health of the people of Texas.
Every dollar donated to DENPAC goes directly to state candidates who are friends of dentistry, regardless of their political party. And we have a proven record of success. In election years, DENPAC contributes over $300,000 to candidates running for state office, historically winning over 90% of our targeted races. By contributing to these candidates, DENPAC facilitates relationships between the TDA legislative team, TDA member dentists, and key decisionmakers at the Capitol. These relationships are invaluable to TDA’s lobby efforts. The financial support that DENPAC has been able to provide lawmakers over the years has given TDA invaluable access to these crucial players.
The 88th Legislature will convene in January 2023, and your TDA legislative team is already tirelessly at work preparing to advocate for you. The success TDA has seen in the past is a direct result of DENPAC—we were successful because we had a seat at the table. DENPAC exists to ensure that TDA has a constant presence at our state capitol, so that when lawmakers address issues affecting the practice of dentistry, we will be there to make your voice is heard.
DONATING IS EASY
Scan the QR code with your phone’s camera to donate now! You can also visit denpac.org, mail a check, or call 512-443-3675, ext. 123 to make a payment over the phone. If you practice dentistry in Texas, you can’t afford to not be politically engaged.

Help DENPAC help you!
TDA can’t afford to take our past successes for granted. The high turnover in this election year means TDA will have to start from scratch with at least 30 new members of the legislature to establish and grow new relationships with these legislators. That’s why we need your help now more than ever! Every TDA member benefits from the work DENPAC does, but only a small percentage of members are invested in the PAC. It’s time to do your part.
Thank you to all our current DENPAC members and anyone who has participated in previous advocacy efforts. We encourage everyone to become involved, regardless of your level of participation. Even if you can only contribute a few dollars today, your investment will make a difference, and your ongoing support is crucial to keeping our profession strong.
For more information, please visit denpac.org or contact our DENPAC Coordinator Staci Rives by email at srives@tda.org or by phone at 512-443-3675, ext. 123.
www.tda.org | October 2022 599
TDA LEGISLATIVE
JESS CALVERT is TDA’s director of public affairs. He serves as TDA’s in-house legislative consultant and oversees the day-to-day operations of the TDA Department of Legislative, Regulatory, and Governmental Affairs, including policy, DENPAC, and the contract legislative consultants. He began his career as an analyst at the Legislative Budget Board (LBB), where he was assigned to general government and natural resource agencies. After leaving the LBB, he served on the staff of the Texas House of Representatives Committee on Appropriations as an analyst assigned to education, criminal justice, and the judiciary. Prior to coming to work at the TDA, Jess was employed at General Motors Acceptance Corporation, where he managed several residential finance programs. A native of Austin, Jess earned a BA degree from Texas Tech University and a master of public administration from Texas State University.

NORA DEL BOSQUE is a contract legislative consultant to TDA. Nora formerly worked as an associate to past TDA legislative consultant Dick Brown. Prior to that, she worked in public affairs and public relations for the Miller Brewing Company, serving as an industry lobbyist in Arizona, Colorado, New Mexico, and Texas. Before joining Miller Brewing Company, she worked in the Texas Legislature as chief clerk for the House Committee on Appropriations and as a legislative aide to the House Ways and Means Committee and for the late Representative James Hury (D-Galveston). A native of Abilene, Nora earned a BA degree from the University of Texas at Austin.

600 Texas Dental Journal | Vol 139 | No. 10
TEAM
SUSAN ROSS is a contract legislative consultant to TDA and a former director of public affairs for the Association. Prior to representing TDA, she represented the nursing home industry for the Texas Health Care Association and worked as an aide to two influential legislative consultants, Bill Pewitt and Jack Gullahorn. Susan first came to the Capitol in 1993 as an aide to Senator Dan Shelley (R-Crosby). A native of Crosby, she earned a BS degree from Texas A&M University.


DIANE RHODES is TDA’s senior policy manager. She works on legislative and regulatory issues and serves as staff liaison to the Texas State Board of Dental Examiners, the Council on Legislative, Regulatory, and Governmental Affairs (CLRA), the Council on Dental Licensing, Standards, and Education (CDLSE), and the Council on Public Health and Access to Care (CPHAC). Prior to coming to TDA, Diane worked in the Division of State Grants in the governor’s office and as a legislative aide to Representative Tom Ramsay (D-Mount Pleasant). A native of Waco, Diane earned a BA degree from Baylor University.
STACI RIVES is TDA’s PAC coordinator and policy analyst. She serves as staff liaison to DENPAC, the TDA Oral Health PAC (TOHPAC), the Council on Professions and Trends (CPT), and the Community Fluoride Committee (CFC). She worked 6 legislative sessions for various members of the Texas House of Representatives, most recently serving as chief of staff for Representative Ed Thompson (R-Pearland). She also spent time working as an insurance specialist for the Texas Department of Insurance. A native of Houston, Staci earned a BA degree from Southwestern University.

www.tda.org | October 2022 601
POLITICAL PROCESS 101

602 Texas Dental Journal | Vol 139 | No. 10
The Texas Dental
Association takes pride in its legislative team and the participation in the political process by member dentists. Although mapping the legislative infrastructure may appear to be a daunting task, the processes can be navigated with the help of experts.
The Texas Senate and House of Representatives meets every 2 years on an odd-numbered year for no more than 140 days. At times, the business of the legislature may exceed the 140 days, and the governor may call a special session for up to 30 days. Although the legislative session is constrained by the time limitations, the truth is the legislators work in their districts all year long to meet with constituents, raise funds for campaigns, and learn which issues affect their areas.

During the 140 days that the legislature meets, the elected officials (31 members of the Senate and 150 members of the House of Representatives) review thousands of bills, listen to committee testimony, meet with visiting constituents and legislative staff, and become policy experts in many areas of law. While this may appear to be a lofty agenda for the elected official, the procedure for enacting a law is particularly cumbersome involving numerous steps in both the House and Senate. At every point in the process, the bill’s survival is at risk. Also, at every point in the process, the public has the opportunity to make their opinions heard by meeting with their elected officials and attending committee hearings.
The lieutenant governor presides over the Texas Senate and is elected by a statewide popular vote to serve a 4-year term of office. However, the lieutenant governor is not a member of the Senate and only votes to break a tie. The lieutenant governor also appoints all chairs and members to all Senate committees and refers all of the bills to the committees as well. Lieutenant Governor Dan Patrick currently presides over the Texas Senate and the next election for the position is scheduled for 2022.
In the other chamber, the speaker of the house presides over the Texas House of Representatives. The presiding officer is elected by a majority of the House members and appoints all chairs and members to House committees. The speaker of the house also refers all of the bills to the House committees.
Unlike the lieutenant governor, the speaker of the house is a member of his/her chamber and has full voting rights as other House members.
Speaker Dade Phelan currently presides over the House of Representatives.
While the legislative process is tedious and calculated, the democratic process relies heavily on civic participation and engagement. The process encourages constituents to meet with their legislators, understand the issues, and express their opinions to the offices of the officials. With today’s technology and the expertise of the TDA, member dentists have many valuable tools to help effectively voice their opinions.
From fundraisers for candidates and Legislative Day to letter writing campaigns and preparing for testimony before the House or Senate committees, the Texas Dental Association is ready and able to assist its members with political participation that supports the goals of organized dentistry and protect the future of the profession. With the influx of new senators and representatives into the Texas Legislature, the TDA hopes to encourage more member dentists to participate in the political process and be advocates for the profession.
www.tda.org | October 2022 603

604 Texas Dental Journal | Vol 139 | No. 10
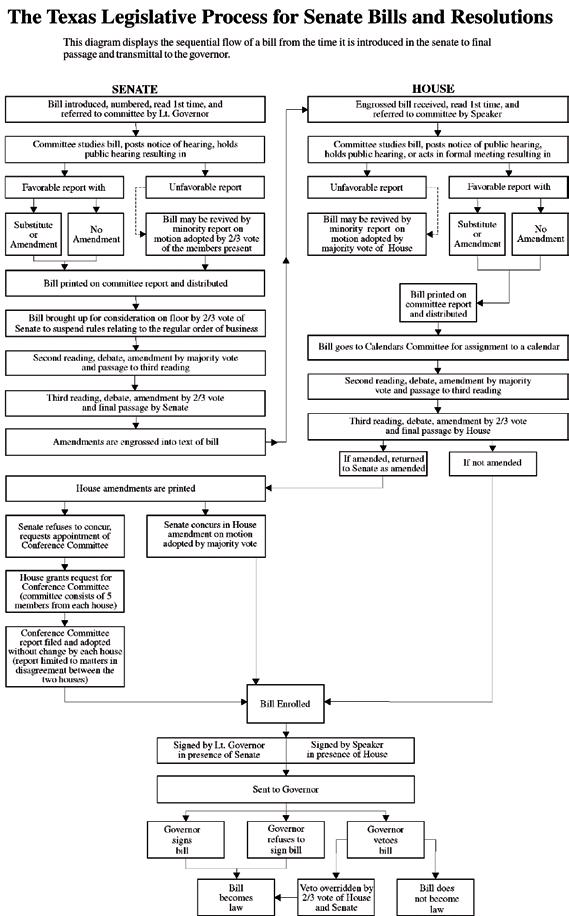
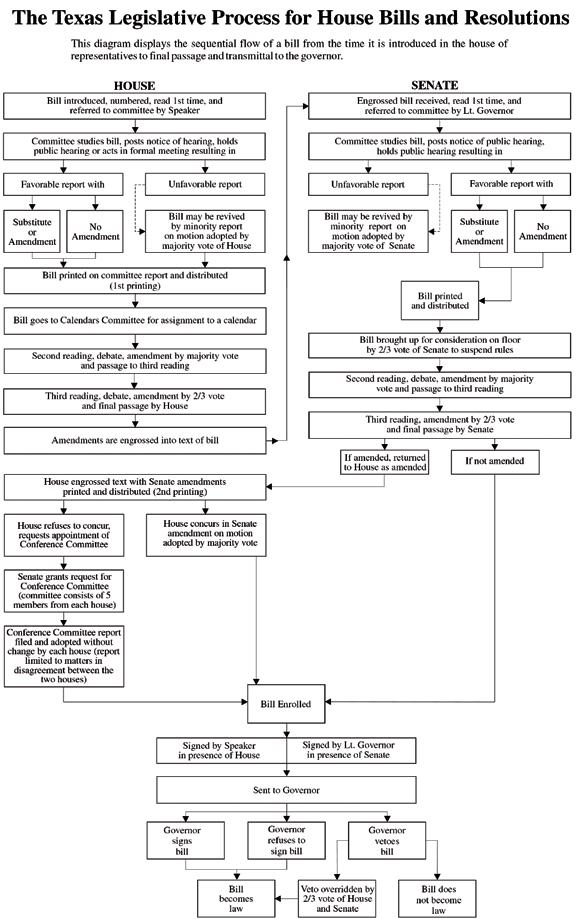
HOW A BILL BECOMES A LAW IN TEXAS
LEGISLATIVE BRANCH OF GOVERNMENT
The Texas Constitution divides state government into 3 separate but equal branches: the executive branch, headed by the governor; the judicial branch, which consists of the Texas Supreme Court and all state courts; and the legislative branch, headed by the Texas Legislature, which includes the 150 members of the House of Representatives and the 31 members of the state Senate.
Members of the House of Representatives are elected to 2-year terms and represent districts of about 168,000 people each. Senators serve 4-year terms and serve about 850,000 people each.
The legislature meets every odd-numbered year to write new laws and to find solutions to the problems facing the state. This meeting time, which begins on the second Tuesday in January and lasts 140 days, is called the regular session. The governor can direct the legislature to meet at other times also. These meetings, called special sessions, can last no more than 30 days and deal only with issues chosen by the governor.
On the first day of each regular session, the 150 members of the House of Representatives choose one of their members to be the speaker of the House. The speaker is the presiding officer of the House. He or she maintains order, recognizes members to speak during debate, and rules on procedural matters.
The speaker also appoints the chairs and vice chairs of the committees that study legislation and decides which other representatives will serve on those committees, subject to seniority rules. There are 31 committees, each of which deals with a different subject area, and 5 committees that deal with procedural or administrative matters for the House. Most members serve on 2 or 3 different committees.
www.tda.org | October 2022 605
THE
In the Senate, the presiding officer is the lieutenant governor, who is not actually a member of the Senate. The lieutenant governor is the secondhighest ranking officer of the executive branch of government and, like the governor, is chosen for a 4-year term by popular vote in a statewide election.
The first thing that the speaker of the house and the lieutenant governor ask their respective houses of the legislature to do is to decide on the rules that the legislators will follow during the session. Some legislative procedures are provided for in the state constitution, but additional rules can be adopted by a house of the legislature if approved by a majority vote of its members.
Once rules have been adopted, the legislature begins to consider bills.
INTRODUCING A BILL
A representative or senator gets an idea for a bill by listening to the people he or she represents and then working to solve their problem. A bill may also grow out of the recommendations of an interim committee study conducted when the legislature is not in session. The idea is researched to determine what state law needs to be changed or created to best solve that problem. A bill is then written by the legislator, often with legal assistance from the Texas Legislative Council, a legislative agency which provides bill drafting services, research assistance, computer support, and other services for legislators.
Once a bill has been written, it is introduced by a member of the House or Senate in the member’s own chamber. Sometimes, similar bills about a particular issue are introduced
in both houses at the same time by a representative and senator working together. However, any bill increasing taxes or raising money for use by the state must start in the House of Representatives.
House members and senators can introduce bills on any subject during the first 60 calendar days of a regular session. After 60 days, the introduction of any bill other than a local bill or a bill related to an emergency declared by the governor requires the consent of at least four-fifths of the members present and voting in the House or four-fifths of the membership in the Senate.
After a bill has been introduced, a short description of the bill, called a caption, is read aloud while the chamber is in session so that all of the members are aware of the bill and its subject. This is called the first reading, and it is the point in the process where the presiding officer assigns the bill to a committee. This assignment is announced on the chamber floor during the first reading of the bill.
THE COMMITTEE PROCESS
The chair of each committee decides when the committee will meet and which bills will be considered. The House rules permit a House committee or subcommittee to meet: (1) in a public hearing where testimony is heard and where official action may be taken on bills, resolutions, or other matters; (2) in a formal meeting where the members may discuss and take official action without hearing public testimony; or (3) in a work session for discussion of matters before the committee without taking formal action. In the Senate, testimony may be heard and official action may be taken at any meeting of
a Senate committee or subcommittee.
Public testimony is almost always solicited on bills, allowing citizens the opportunity to present arguments on different sides of an issue.
A House committee or subcommittee holding a public hearing during a legislative session must post notice of the hearing at least 5 calendar days before the hearing during a regular session and at least 24 hours in advance during a special session. For a formal meeting or a work session, written notice must be posted and sent to each member of the committee 2 hours in advance of the meeting or an announcement must be filed with the journal clerk and read while the House is in session. A Senate committee or subcommittee must post notice of a meeting at least 24 hours before the meeting.
After considering a bill, a committee may choose to take no action or may issue a report on the bill. The committee report, expressing the committee’s recommendations regarding action on a bill, includes a record of the committee’s vote on the report, the text of the bill as reported by the committee, a detailed bill analysis, and a fiscal note or other impact statement, as necessary. The report is then printed, and a copy is distributed to every member of the House or Senate.
In the House, a copy of the committee report is sent to either the Committee on Calendars or the Committee on Local and Consent Calendars for placement on a calendar for consideration by the full House. In the Senate, local and noncontroversial bills are scheduled for Senate consideration by the Senate Administration Committee. All other bills in the Senate are placed on the regular order of business for consideration by the full Senate in the
606 Texas Dental Journal | Vol 139 | No. 10
www.tda.org | October 2022 607
order in which the bills were reported from Senate committee. A bill on the regular order of business may not be brought up for floor consideration unless the Senate sponsor of the bill has filed a written notice of intent to suspend the regular order of business for consideration of the bill.
FLOOR ACTION
When a bill comes up for consideration by the full House or Senate, it receives its second reading. The bill is read, again by caption only, and then debated by the full membership of the chamber. Any member may offer an amendment, but it must be approved by a majority of the members present and voting to be adopted. The members then vote on whether to pass the bill. The bill is then considered by the full body again on third reading and final passage. A bill may be amended again on third reading, but amendments at this stage require a two-thirds majority for adoption. Although the Texas Constitution requires a bill to be read on 3 separate days in each house before it can have the force of law, this constitutional rule may be suspended by a four-fifths vote of the House in which the bill is pending. The Senate routinely suspends this constitutional provision in order to give a bill an immediate third reading after its second reading consideration. The House, however, rarely suspends this provision, and third reading of a bill in the House normally occurs on the day following its second reading consideration.
In either house, a bill may be passed on a voice vote or a record vote. In the House, record votes are tallied by an electronic vote board controlled by buttons on each member’s desk. In the Senate, record votes are taken by calling the roll of the members.
If a bill receives a majority vote on third reading, it is considered passed. When a bill is passed in the house where it originated, the bill is engrossed, and a new copy of the bill which incorporates all corrections and amendments is prepared and sent to the opposite chamber for consideration. In the second house, the bill follows basically the same steps it followed in the first house. When the bill is passed in the opposite house, it is returned to the originating chamber with any amendments that have been adopted simply attached to the bill.
ACTION ON THE OTHER HOUSE’S AMENDMENTS AND CONFERENCE COMMITTEES
If a bill is returned to the originating chamber with amendments, the originating chamber can either agree to the amendments or request a conference committee to work out differences between the House version and the Senate version. If the amendments are agreed to, the bill is put in final form, signed by the presiding officers, and sent to the governor.
Conference committees are composed of 5 members from each house appointed by the presiding officers. Once the conference committee reaches agreement, a conference committee report is prepared and must be approved by at least 3 of the 5 conferees from each house. Conference committee reports are voted on in each house and must be approved or rejected without amendment. If approved by both houses, the bill is signed by the presiding officers and sent to the governor.
GOVERNOR’S ACTION
Upon receiving a bill, the governor has 10 days in which to sign the bill, veto it, or allow it to become law without a signature. If the governor vetoes the bill and the legislature is still in session, the bill is returned to the House in which it originated with an explanation of the governor’s objections. A two-thirds majority in each house is required to override the veto. If the governor neither vetoes nor signs the bill within 10 days, the bill becomes a law. If a bill is sent to the governor within 10 days of final adjournment, the governor has until 20 days after final adjournment to sign the bill, veto it, or allow it to become law without a signature.
CONSTITUTIONAL AMENDMENTS
Proposed amendments to the Texas Constitution are in the form of joint resolutions instead of bills and require a vote of two-thirds of the entire membership in each house for adoption. Joint resolutions are not sent to the governor for approval, but are filed directly with the secretary of state. A joint resolution proposing an amendment to the Texas Constitution does not become effective until it is approved by Texas voters in a general election.
Upon receiving a bill, the governor has 10
days in which to sign the bill, veto it, or allow it to become law without a signature.
608 Texas Dental Journal | Vol 139 | No. 10
www.tda.org | October 2022 609
Compared to the Texas Legislature that meets biennially to make laws, the TSBDE’s rulemaking process is fluid. Not including the dental board’s updated COVID-19 emergency rule, the dental board adopted 8 rule changes from December 2021 to August 2022.
THE TEXAS STATE BOARD OF DENTAL EXAMINERS— REGULATING THE PROFESSION

610 Texas Dental Journal | Vol 139 | No. 10
The Texas legislature meets every 2 years for 140 days. During that time thousands of bills are considered, and only a small number making it through the process to become a law. The bills that complete the legislative process are codified in law in the Texas Statutes. The Texas Dental Practice Act is found in the Texas Occupations Code Chapters 251 through 267.
Under the Texas Constitution, only the state legislature can enact laws such as the Dental Practice Act (DPA). The DPA authorizes the Texas State Board of Dental Examiners (TSBDE) to enforce state law and TSBDE rules, investigate and punish violators, and make binding rules.
Compared to the Texas Legislature that meets biennially to make laws, the TSBDE’s rulemaking process is fluid. Not including the dental board’s updated COVID-19 emergency rule, the dental board adopted 8 rule changes from December 2021 to August 2022.
It is important for Texas dentists to remain informed about changing rules and how the rules impact their dental practice. That can be tough, but one important benefit of TDA membership is TDA advocacy at both the state Capitol and the dental board. In addition to helping ensure the most balanced regulatory environment for dentists, TDA also keeps members educated about rule changes in its written publications, emails, and podcasts. Individual help is also only a phone call away for TDA members.
INDIVIDUALIZED TSBDE ASSISTANCE
TDA provides individualized help for member dentists with TSBDE issues. Call or email Senior Policy Manager Diane Rhodes at drhodes@tda.org or 512-443-3675 ext 122.
TSBDE RULE CHANGES
Dental Board Amends and Adopts New Rules: December 31, 2021, Effective Date
The TSBDE adopted 2 rule amendments and 1 new rule that became effective on December 31, 2021.
Exemption from Licensure for Certain Military Spouses
The amended rules addresses what a military spouse must submit to the dental board to establish residency in Texas to qualify for exception for dental and dental hygiene licensure as required by House Bill 139 of the Regular Session of the 87th Texas Legislature.1,2
Individualized TSBDE Assistance
TDA provides individualized help for member dentists with TSBDE
issues. Call or email Senior Policy Manager Diane Rhodes at drhodes@tda.org or 512-443-3675 ext 122.
www.tda.org | October 2022 611
Call Coverage Agreements
The new rule establishes minimum requirements for call coverage agreements pursuant to House Bill 2056 of the Regular Session of the 87th Texas Legislature. The new rule is consistent with the call coverage language in the teledentistry bill (ie, House Bill 2056) and with the Medical Board’s call coverage language pursuant to the telehealth statute.3
The agreements may be oral or written and apply to dentists providing call coverage, regardless of the technology used. The covering dentist must give the patient’s dentist of record a report detailing the dental intervention or advice provided to the patient. The dentist’s party to the agreement can decide the agreement’s timing, how the report will be provided, and who receives the report.
Dental Board Adopts Rule Amendment: March 10, 2022, Effective Date
The TSBDE adopted 1 rule amendment that became effective on March 10, 2022.
Remedial Plans
The amendment addresses remedial plans. The amendment establishes when multiple remedial plans may be issued and when a remedial plan can be removed from the TSBDE’s public website. The amended rule is consistent with Senate Bill 1534 of the 87th Texas Legislature, Regular Session (2021).
The dental board may not issue a remedial plan to resolve a complaint against a licensee if the license holder entered into a remedial plan in the preceding 5 years.
For all remedial plans issued on or after September 1, 2021, the TSBDE may remove any public information about the remedial plan from the dental board’s website on or after the 5th anniversary of the date the TSBDE issued the remedial plan. However, public information about the remedial plan cannot be removed from the TSBDE’s website if the plan was related to the delivery of health care or more than one remedial plan was issued by the TSBDE to resolve complaints alleging the same violation including a complaint not related to the delivery of health care.
To request removal of a remedial plan, the dentist or dental hygienist must submit a written request to the TSBDE’s general council. The request must include (1) the specific case number of which removal is requested; and (2) proof that the dentist or dental hygienist complied with and successfully completed the terms of the remedial plan of which removal is requested.4
612 Texas Dental Journal | Vol 139 | No. 10
According to the TSBDE’s rule synopsis published in the Texas Register, “A dentist must ask the patient to come to the dental practice for a physical examination if the diagnosis or treatment utilizing teledentistry is not adequate or consistent with the standard of care.”7
Dental Board Amends and Adopts New Rules: June 2, 2022, Effective Date
The TSBDE adopted 1 rule amendment and 1 new rule that became effective on June 2, 2022.
Teledentistry
The new teledentistry rule creates the standards for delivering teledentistry dental services as authorized by the Texas Legislature in 2021.5

During that legislative session, TDA worked with lawmakers and stakeholders to pass HB 2056 permitting teledentistry in Texas, while upholding the current standard of care and mandating proper dentist oversight, supervision, and delegation.
After the legislature passed the teledentistry bill in 2021, TDA advocacy staff immediately began discussions with the TSBDE and Governor Abbott’s office to make sure the teledentistry rule maintained a single standard of dental care and held teledentistry services to the same standards and guidelines as exist for in-person dental services.
Dentists utilizing teledentistry must adopt protocols to prevent fraud and abuse in teledentistry. Dentists utilizing teledentistry must provide patients with notice how to file a complaint with the TSBDE. The notice must include: (1) the TSBDE’s name, (2) the TSBDE’s mailing address, and the (3) TSBDE’s telephone number. Dentists can accomplish such notice by prominently placing a sign where rendering teledentistry services, or including the information on written registration forms, brochures, contracts for dental services, or bills for dental services. Dentists can download signs from the TSBDE’s website, or the dentist can create their own matching requirements in the board rule governing consumer information—22 TAC §108.3, Consumer Information.
Practicing Teledentistry
A dentist, dental hygienist, or dental assistant delivering teledentistry services to Texas’ patients must hold an active Texas license or registration issued by the TSBDE. This means only registered dental assistants may provide teledentistry services.
Dental health professionals performing teledentistry services or procedures are subject to the same standard of care that applies in an in-person setting. Dentists must (1) establish a practitionerpatient relationship and (2) maintain complete and accurate patient dental records as required by the recordkeeping rule (22 TAC §108.8).
Dentists may only delegate and simultaneously supervise through teledentistry no more than a total of 5 dental hygienists and registered dental assistants.
Measures must be in place to protect all patient communications consistent with federal and state privacy laws.
Individuals, including prospective patients and patients of record, and family members of prospective
www.tda.org | October 2022 613
The TSBDE’s June 2022 newsletter, available on the TSBDE’s website, tsbde.texas.gov, defined “reasonable and prudent dentist” in the standard of care and teledentistry rules. According to the article, the TSBDE’s Dental Review Panel (DRP) determines what a reasonable and prudent dentist would do in a specific situation. This, in turn, helps to create a peer established standard of care. The DRP basis its standard of care interpretation on statements from major dental organizations, generally accepted dental practices, and evidenced-based research papers for evidence of what constitutes appropriate care under similar circumstances.
patients and patients of record, may submit photographs or digital images to a Texaslicensed dentist or Texas-licensed dental hygienist for the sole and limited purpose of screening, assessment, or examination. In Texas, only dentists may perform comprehensive examination, diagnosis, and treatment planning.
Teledentistry Informed Consent
Informed consent for teledentistry dental services must include not only the existing informed consent requirements from the minimum standard of care rule and the recordkeeping rule, but also the (1) delegating dentist’s name, (2) Texas license number, (3) credentials, (4) qualifications, (5) contact information, (6) practice location involved in a patient’s care, and (7) disclosure to the patient that the dentist delegated the service(s).
Additionally, the teledentistry informed consent must include the (1) name and (2) Texas license number or registration number for all dental hygienists and registered dental assistants providing patient care along with their (3) credentials and qualifications. This information must be both publicly displayed and given to the patient in writing.
Issuing Prescriptions Using Teledentistry
The same standards apply to prescriptions issued by dentists via teledentistry as issued in an in-person setting. Prescribing dentists have to meet the standard of care, professional practice standards, and all applicable federal and state regulations when issuing, dispensing, delivering, or administering a prescription medication through teledentistry.
As with in-person prescriptions, teledentistry prescriptions must be issued for legitimate dental purposes as part of a practitioner-patient relationship. Dentists need to meet all applicable federal and state regulations before prescribing, dispensing, delivering, or administering a dangerous drug or controlled substance.
Any prescription drug orders resulting from a teledentistry dental service are subject to all regulations, limitations, and prohibitions set out in the federal and Texas Controlled Substances Act, Texas Dangerous Drug Act, and any other applicable federal and state law.
Limitation on Certain Teledentistry Prescriptions
A dentist prescribing a patient a controlled substance as a teledentistry dental service cannot prescribe more than a 2-day supply of opiates or a 5-day supply of controlled substances other than opiates. For Saturdays, Sundays, or national holidays, the time period extends to include the next day that is not a Saturday, Sunday, or national holiday.
Remember that before prescribing or dispensing opioids, benzodiazepines, barbiturates, or carisoprodol, a dentist must access the patient’s prescription drug history through the Texas Pharmacy Board’s Prescription Monitoring Program.
Minimum Standard of Care, General When it adopted the new teledentistry rule, the dental board also adopted
614 Texas Dental Journal | Vol 139 | No. 10
amendments to the minimum standard of care rule.6 The rule amendments were necessary to allow for the provision of teledentistry dental services without first requiring the patient to have an in-person examination as long as the dentist adheres to the standard of care. However, a dentist must ask the patient to come into the office for a physical examination if the diagnosis or treatment utilizing teledentistry is not adequate or consistent with the standard of care.
The standard of care does not require a dentist to perform an in-person examination before every type of dental service, but depending on the circumstances, the standard of care may require a dentist to perform an in-person examination or have other in-person contact with a patient before providing teledentistry dental services.
According to the TSBDE’s rule synopsis published in the Texas Register, “A dentist must ask the patient to come to the dental practice for a physical examination if the diagnosis or treatment utilizing teledentistry is not adequate or consistent with the standard of care.”7
TDA’s advocacy efforts preserved that the dentist must perform a limited physical examination when a reasonable and prudent dentist would do so and perform and review that examination, at a minimum, annually.
The TSBDE’s June 2022 newsletter, available on the TSBDE’s website, tsbde. texas.gov, defined “reasonable and prudent dentist” in the standard of care and teledentistry rules. According to the article, the TSBDE’s Dental Review Panel (DRP) determines what a reasonable and prudent dentist would do in a specific situation. This, in turn, helps to create a peer established standard
of care. The DRP basis its standard of care interpretation on statements from major dental organizations, generally accepted dental practices, and evidenced-based research papers for evidence of what constitutes appropriate care under similar circumstances.
Dental Board Adopts Rule Repeal and Rule Amendment: September 1, 2022, Effective Date
The TSBDE adopted 1 rule repeal and 1 rule amendment that became effective on September 1, 2022.
Dental Health Care Workers
The repeal deletes unnecessary repetitive statutory language found in Chapter 85 of the Texas Health and Safety Code.
Continuing Education Providers
The amended rule adds Dental Risk Solutions, LLC as a TSBDE-approved continuing education course provider.8
Check Your Team Members’ Licenses and Registrations
The dentist is responsible for all delegated acts performed by dental hygienists and dental assistants under their direction. This includes ensuring that the dental hygienists and registered dental assistants have current licenses and registrations.9
In order for a dentist to delegate the taking of patient x-rays to a dental assistant, the dental assistant must hold a registration issued by the TSBDE (ie, Registered Dental Assistant).10 In order for a registered dental assistant or dental hygienist to monitor nitrous oxide, he or she must have a specific N20 monitoring designation issued by the TSBDE.11, 12
Additionally, a dentist can’t delegate coronal polishing or pit & fissure sealants to a dental assistant unless the dental assistant completed the required education and training prior to the delegation. Dentists are responsible for verifying that the dental assistant has at least 2 years’ experience, current basic life support, and completed the required 8 hours didactic and clinical education in coronal polishing and/ or pit and fissure sealants prior to delegating those procedures.
As a reminder to Texas dentists, training programs may only be offered by dental, dental hygiene, or dental assistant programs accredited by the Commission on Dental Accreditation (CODA) and approved by the TSBDE. Neither dental professional associations nor individual dentists may offer initial training courses unless they are offering a course taught by a CODA-accredited dental education program approved by the TSBDE.
Dentists must perform ongoing due diligence to ensure that all team members working in the dentist’s practice remain in compliance with the TSBDE’s license and registration requirements.
Continuing Education Requirements
TDA understands that tracking your CE requirements can become tedious. To
www.tda.org | October 2022 615
Dentists must perform ongoing due diligence to ensure that all team members working in the dentist’s practice remain in compliance with the TSBDE’s license and registration requirements.
help members with this process, TDA has a CE infographic and new CE mobile app called “Dental Concierge.”
TDA CE Infographic
As a Texas dentist, you are required to take a certain amount of CE to renew your dental license. And depending on what you do, the specifics of what CE you need can change. How do you keep track of the hours you need, in what areas, and what’s acceptable by the Dental Board?
TDA made it easier for you by creating an infographic to help you understand the CE you need.
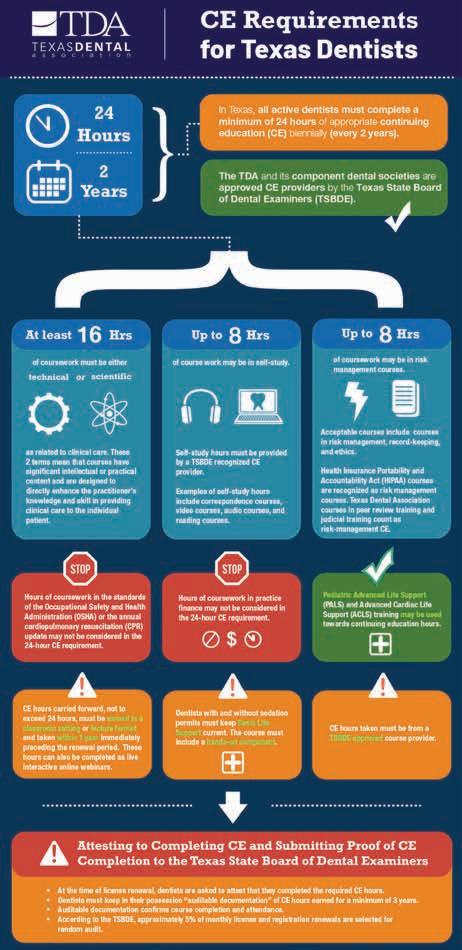
Go to tda.org > Member Center > click on “CE Requirements for Texas Dentists and Staff.”
Not only can dentists confirm their CE requirements, staff can find what CE they need to renew a dental hygiene license or dental assistant registration.
TDA CE Infographic
As a Texas dentist, you are required to take a certain amount of CE to renew your dental license. And depending on what you do, the specifics of what CE you need can change. How do you keep track of the hours you need, in what areas, and what’s acceptable by the Dental Board?
PLEASE NOTE: This is only an excerpt of the infographic, and does not show the full requirements. To view the full infographic, go to tda.org > Member Center > click on “CE Requirements for Texas Dentists and Staff.”
616 Texas Dental Journal | Vol 139 | No. 10
DENTAL CONCIERGE

Dental Concierge is an app and learning management system commissioned by TDA and TDA Perks Program that allows its users to keep track of CE courses taken, which requirements are outstanding, and easily access CE documentation in the event of a TSBDE audit.

CLOSING
that TDA is here to serve you, the member, by helping advance dental positive legislation and regulations as well as keeping you up to date about state legislative and regulatory matters. TDA is vocal about the regulatory and legislative proposals affecting dentistry in Texas. TDA cannot and will not sit silently while decisions are made that impact your dental practice.
Administrative Code §101.14,
Licensure for Certain

Spouses
Administrative Code
for
from Licensure for Certain
Spouses
Texas Administrative Code §108.74, Call Coverage Agreements
Texas Administrative Code §107.204,
Plans
Texas Administrative Code §108.16,
Texas Administrative Code §108.7,
Standard of Care, General
Register. March 11, 2022. Volume 47
10. Page 1174
Texas Administrative Code §104.2(e)(22),
Occupations Code §258.003,

of Delegating Dentist
Texas Administrative Code §114.2,
of Dental Assistants
Administrative Code §114.4,
the Administration of Nitrous
Texas Administrative Code §115.2,
Duties
www.tda.org | October 2022 617 Simplify CE
the whole team. Scan here: Dentists, hygienists, and RDAs can track and submit CE hours with the TDA Dental Concierge app. And you can start right now. tdadentalconcierge.com
The
Remember
References 1. 22 Texas
Exemption from
Military
2. 22 Texas
§103.10, Exemption
Military
3. 22
4. 22
Remedial
5. 22
Teledentistry 6. 22
Minimum
7. Texas
Number
8. 22
Providers 9. Texas
Responsibility
10. 22
Registration
11. 22 Texas
Monitoring
Oxide 12. 22
Permitted
TDA supports member dentists providing dental care in Texas’ dental public health safety net by continuously
advocating for appropriately funded and administratively simple dental programs.

THE PREMIER ADVOCATE FOR MEDICAID & CHIP
618 Texas Dental Journal | Vol 139 | No. 10 TEXAS DENTAL ASSOCIATION:
The Texas Dental Association (TDA) represents dentists participating in Medicaid, the Children’s Health Insurance Program (CHIP), and other public health dental programs helping to make dental care accessible to all Texans. TDA prioritizes maintaining and strengthening Texas’ dental public health safety net by encouraging its member dentists to actively participate in Medicaid, CHIP, and other programs providing needed dental care to children, adults, and individuals with special health care needs.1
Low-income Texans must have access to oral health care though a dental public health safety net that emphasizes health equity, comprehensive dental services, and oral health literacy. This is crucial for Texans to keep a healthy mouth and healthy body. Dental disease often adversely effects an individual’s general health and quality of life.2 Oral health remains an important but often neglected part of overall health and well-being.3
A dental safety net structured to protect the sanctity of the dentist-patient relationship and the dentist’s ability to make clinical decisions based on each patient’s needs will help vulnerable Texans from developing urgent and immediate oral health concerns. Treating dental disease that could easily be prevented or treated in its early stages but progressed to the point of chronic infection, lost gum and bone tissue, and inevitable removal of teeth is a significant reason why Texas’ clinical health care system can become overwhelmed.
A strong dental public health safety net also discourages elected officials from expanding the state’s dental safety net to include mid-level dental providers, such as dental therapists and dental hygiene practitioners, that remove the dentist from the patient and create a 2-tiered system of care.
TDA supports member dentists providing dental care in Texas’ dental public health safety net by continuously advocating for appropriately funded and administratively simple dental programs. TDA’s advocacy occurs at the legislature and at state agencies to help ensure the best possible dental programs for patients and dentists in Texas.
TDA SEEKS MEDICAID DENTAL FUNDING INCREASE
For Texas’ Medicaid dental program to remain effective and cost efficient, steps must be taken to ensure continued dentist participation. The most important step being a reimbursement rate adjustment so that dentists can continue program participation.
That’s why TDA’s advocacy team already started laying the groundwork for TDA’s Medicaid dental fee increase request for the upcoming 88th Legislative Session. Maintaining adequate general state revenue for Medicaid is an essential part of setting reimbursement rates that help maintain a stable network of dentists.
TDA’s Role in APM Models
Throughout discussions over the past 8 years, TDA negotiated to achieve the best APM/ VBP model for Texas’ dentists. TDA has met, and will continue meeting, with both HHSC and the DMOs to help determine the best design for dentists. TDA identifies and advocates for APM/VBP alternatives that allow the DMOs to meet the state’s APM/ VBP requirement, without jeopardizing reimbursement to participating dentists.
www.tda.org | October 2022 619
At the end of the 2019 legislative session, TDA began discussions with HHSC to ensure that dentistry was included in improvements to Medicaid managed care required by Senate Bill 1207. TDA’s been very involved with HHSC’s State Medicaid Managed Care Advisory Committee and directed dental Medicaid administration improvement projects through the committee for recommended adoption by HHSC.
TDA PARTICIPATES IN RIDER 26 WORKGROUP
The Texas Health and Human Services Commission (HHSC) created the workgroup according to a budget rider from the 87th Regular Legislative Session. The workgroup is developing and submitting Medicaid dental policy recommendations to HHSC’s Executive Commissioner by the December 31, 2022. The recommendations will be specific to preventing waste, fraud, and abuse in the Medicaid dental program as required in the budget rider. Dr Paul Kennedy III represents TDA on the workgroup.
TDA’s Council on Public Health and Access to Care completed a comprehensive review and analysis of the entire Medicaid dental program and identified program policies and dental procedures codes for the workgroup’s consideration. Within TDA’s comments, TDA included overall concerns with the workgroup’s methodology. Namely, (1) lack of access to Medicaid dental claims data; and (2) lack of access to dental specialty feedback.
HHSC staff and workgroup members will meet one last time to review and finalize the draft Rider 26 report before sending it to HHSC’s Executive Commissioner. Depending on the information included in the draft report, TDA may meet with HHSC Executive Commissioner Cecile Young to discuss the report.
TDA MONITORS VALUE-BASED PAYMENT QUALITY IMPROVEMENT
TDA staff met during the summer with HHSC’s Health Quality Institute Director, and HHSC’s lead staffer to discuss the ongoing application of HHSC’s alternative payment models (APMs) to the dental maintenance organizations (DMOs).
For years, HHSC’s been slowly transitioning its numerous Medicaid health programs away from fee-for-service payment models and into APMs within the value-based care (VBC) system. Since 2012, HHSC required that each DMO submit an annual report on its VBC activities with its dentists for HHSC information and planning purposes.
Beginning in 2021, HHSC required 50% of the DMO’s dentist provider payments to be through an APM and not fee-for-service. Additionally, 10% of the DMOs APMs had to include financial risk for dentist providers.
HHSC has no current plans to change the DMOs APM requirements, or the data collection tools used by the DMOs. However, TDA staff will meet with the Health Quality Institute Director, and HHSC’s lead staffer, sometime in late 2023 to deliberate possible HHSC changes to the DMO APM requirements.
620 Texas Dental Journal | Vol 139 | No. 10
TDA’S ROLE IN APM MODELS
Throughout discussions over the past 8 years, TDA negotiated to achieve the best APM/VBP model for Texas’ dentists. TDA has met, and will continue meeting, with both HHSC and the DMOs to help determine the best design for dentists. TDA identifies and advocates for APM/VBP alternatives that allow the DMOs to meet the state’s APM/VBP requirement, without jeopardizing reimbursement to participating dentists.
TDA will keep promoting APM/ VBP efforts that positively reward participating dentists and not financially penalize participating dentists.
TDA COLLABORATES WITH HHSC ON MEDICAID TELEDENTISTRY RULE DEVELOPMENT
TDA staff maintains ongoing communications with the HHSC associate commissioners responsible for rule development about the timeline for writing the teledentistry Medicaid rules. Currently, there is no date set, but HHSC will contact TDA when the process begins so that TDA can assist in writing the rules.
TDA WORKS TO IMPROVE MEDICAID OPERATING ROOM ACCESS
We have heard from members participating in the Medicaid dental program that there has been a significant decrease in operating room access for dental procedures. Patients are often waiting up to 6 months or more to access needed dental treatment under general anesthesia.
This is largely due to low Medicaid reimbursement rates for general anesthesia, and the facility fee that goes to the hospital or ambulatory surgical center (ASC).
TDA remains committed to improving access to dental care for the segment of the Medicaid dental population that rely on receiving dental services under general anesthesia in operating room settings.

While TDA advocates at the state level, the American Dental Association, the American Academy of Pediatric Dentistry, and the American Association of Oral and Maxillofacial Surgeons asked federal lawmakers to improve hospital operating room access for children and special needs patients. The groups called on the Centers for Medicare and Medicaid Services (CMS) to create a sustainable operating room billing mechanism for dental surgical services in both Medicare and Medicaid. Namely, designating a specific Medicare billing code inclusive of fair reimbursement for dental services provided in a hospital operating room or ASC.
The groups secured an initial victory when CMS announced it will publish the “2023 Proposed Hospital Outpatient Payment Rule” on July 26, 2022. The proposed rule revises the Medicare hospital outpatient prospective payment system and the Medicare ASC payment system for calendar year 2023. Specifically, the draft rule moves the unlisted CPT 41899 code to the Ambulatory Payment Classification (APC) for dental procedures (APC 5871) with a mean rate of $1,958. This should result in the individual state Medicaid facility rates for dental cases becoming/being much more competitive.
However, CMS did not go so far as to establish a dental code for use within an ASC, so there is more work to be done at the federal level.
While federal efforts continue, so will TDA’s efforts at HHSC and with the Medicaid medical and dental managed care organizations to develop solutions to the operating room crisis. TDA is also exploring legislative action during the upcoming 88th Legislative Session.
TDA KEEPS DENTIST CONCERNS AT THE FOREFRONT: STATE MEDICAID MANAGED CARE ADVISORY COMMITTEE
At the end of the 2019 legislative session, TDA began discussions with HHSC to ensure that dentistry was included in improvements to Medicaid managed care required by Senate Bill 1207. TDA’s been very involved with HHSC’s State Medicaid Managed Care Advisory Committee and directed dental Medicaid administration improvement projects through the committee for recommended adoption by HHSC.
www.tda.org | October 2022 621
TDA FIGHTS AGAINST ILLEGAL MEDICAID DENTAL SOLICITATION
TDA, the Office of Inspector General (OIG), HHSC, and the DMOs continue efforts to end illegal Medicaid dental solicitation. Medicaid program rules prohibit providers from offering clients inducements to influence their health care decisions.4
Solicitation can include:
• Unsolicited personal contact, such as direct mail, telephone, and door-to-door solicitation.
• Canvassing neighborhoods, offering free transportation to clients.
• Offering gifts or other inducements designed to influence a client’s choice of provider.
• Cash, cash equivalents and gift cards in any amount are not permitted. These items include gift cards and dental services or credits to parents who bring in Medicaid-eligible patients for treatment.5
The regulations apply to Medicaid participating dentists regardless if the dentist offers the solicitation directly or through a third party such as individuals or marketing firms soliciting to Medicaid clients.
OIG created a brochure to educate dentists about the signs and consequences of illegal dental solicitation in Medicaid. Download it from https://oig.hhs.texas.gov/sites/default/ files/documents/resources/OIG-DentalSolicitation-Brochure-Accessible-10-2019.pdf.
This brochure represents years of teamwork between TDA, OIG, and HHSC, to create an easy-to-understand explanation of illegal Medicaid dental solicitation.
Illegal
OIG investigates illegal solicitation as part of its mission to detect, prevent, and deter fraud, waste and abuse in Medicaid and CHIP. Dentists cannot illegally solicit patients.
Dental Solicitation What dental providers need to know to avoid illegally soliciting clients who have Medicaid. The office’s mission is to strengthen Texas Health and Human Services’ capacity to combat fraud, waste and abuse in publicly funded, state-run health and human services programs. Our values are: • Accountability: We serve Texans and take responsibility for our decisions and actions. • Integrity: We demonstrate honesty and credibility. • Collaboration: We work collectively to multiply our contributions and create shared goals, leading to greater success. • Excellence: We strive to be and do our best. Main number: 512-491-2000 Fraud hotline: 800-436-6184 211 Texas: Dial 2-1-1, select your language, then choose Option 3. Website: oig.hhsc.texas.gov Facebook: facebook.com/TxOIG Twitter: twitter.com/TexasOIG About the Office of Inspector General Contact Us HHS COMM 20D0031 October 2019
According to OIG’s website, “Sanctions against providers who solicit patients can include exclusion from the Medicaid and CHIP programs, disciplinary action from the Texas State Board of Dental Examiners, and monetary penalties. Depending on the conduct, e.g., whether there is resulting patient harm, solicitation penalties may be up to $15,000 per violation, in addition to potential penalties based on the paid claims amount.”6
OIG investigates illegal solicitation as part of its mission to detect, prevent, and deter fraud, waste and abuse in Medicaid and CHIP. Dentists cannot illegally solicit patients.
OIG created a brochure to educate dentists about the signs and consequences of illegal dental solicitation in Medicaid. Download it from https://oig.hhs.texas.gov/sites/ default/files/documents/resources/ OIG-Dental-Solicitation-BrochureAccessible-10-2019.pdf. This brochure represents years of teamwork between TDA, OIG, and HHSC, to create an easyto-understand explanation of illegal Medicaid dental solicitation.
TDA encourages dentists to download the brochure on illegal dental solicitation from OIG’s website and share it with Medicaid clients, provider dentists in their communities, and local businesses. The brochure is
especially helpful in educating Medicaid clients and local businesses to avoid participation in illegal Medicaid solicitation activities.
In February 2022, OIG extended its illegal Medicaid dental solicitation efforts to the Texas Department of State Health Services (DSHS).7 OIG and DSHS are partnering to share information about illegal dental solicitation with participating Texas Health Steps dentists. Outreach occurred through the DSHS Regional, and Local Health Operations and OIG staff is training DSHS staff about illegal dental solicitation and the OIG’s role in preventing it.
Fighting Fraud, Waste and Abuse
The OIG enforces Texas Administrative Code (TAC) §371.1669, which prohibits a person from offering any payment that may influence a potential client’s selection of a Medicaid service provider.
If a provider solicits Medicaid clients, the provider may be found guilty of a Class A misdemeanor and a third degree felony if the dentist was previously convicted of illegal dental solicitation or was employed by the federal, state or local government at the time. The provider may be subject to disciplinary action by the Texas State Board of Dental Examiners, an injunction, civil penalties of up to $10,000 and possible exclusion as a provider.*
Illegal Dental Solicitation
Dental providers are prohibited from offering cash, gifts or other items to people who have Medicaid in order to influence their health care decisions. Providers may not offer and clients may not accept:
• Cash, cash equivalents or gift cards in any amount.
• Transportation unless it’s properly arranged through the Medicaid Transportation Program.
• Free or discounted services for a family member to influence their health care decisions.

Providing goods or services of any value could be considered a violation, but that would typically not be the case for noncash, low-cost items such as a toothbrush valued less than $10.
Office of Inspector General Investigations
The OIG may investigate improper gifts to potential clients, including providers who hire people to canvass neighborhoods looking for Medicaideligible children and pay drivers to transport children for Medicaid services. The OIG may also investigate providers who advertise free transportation on their website.
This material is provided for general informational purposes only and is not intended to present an official position of the OIG or legal advice. The facts and circumstances of any particular question should be evaluated independently.
*Texas Occupations Code, Sec. 102.001, 102.009, 102.010
TEXAS OFFICE OF INSPECTOR GENERAL QUARTERLY REPORTS
OIG Quarterly Reports 2022
• https://oig.hhs.texas.gov/sites/default/
https://oig.hhs.texas.gov/sites/default/
important
TDA MEETS WITH STATE AGENCY OFFICIALS AND DENTAL MANAGED CARE ORGANIZATIONS
TDA regularly meets with HHSC leaders and representatives from the DMOs to discuss program concerns and ways in which to improve the delivery of dental services for patients and participating dentists. These meetings are very productive and give TDA an opportunity to speak with all participating entities at the same time.
CLOSING
The state’s top legislative and agency decision makers regularly seek TDA’s input about Medicaid, CHIP, and other public health programs. Every day, TDA represents its members helping protect patients and Medicaid- and CHIPparticipating dentists.
TDA provides individualized help for member dentists with Medicaid and CHIP. For individual help, email Senior Policy Manager Diane Rhodes at drhodes@tda.org or call 512-443-3675 ext 122.
All TDA’s advocacy efforts, both legislatively and within state agencies, result in program changes that improve Texas dentists’ experience with public health dental programs and lead to significant improvements in the delivery of dental care to Texans.
TDA provides individualized help for member dentists with Medicaid and CHIP. For individual help, email Senior Policy Manager Diane Rhodes at drhodes@tda.org or call 512-443-3675 ext 122.
References
1. Texas Dental Association. Policy 66-2010-H.
2. US Department of Health and Human Services, Oral Health in America: A Report of the Surgeon General (Rockville, MD: US Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health, 2000), http://www.nidcr.nih. gov/DataStatistics/SurgeonGeneral/ Documents/hck1ocv.@www.surgeon. fullrpt.pdf.
3. Ibid.
4. 1 Texas Administrative Code §371.27, Prohibition Against Solicitation of Medicaid or CHIP Recipients
5. 1 Texas Administrative Code §354.152, Provider Marketing
6. Texas Office Of Inspector General. Accessed September 22, 2021, https://oig. hhs.texas.gov/about-us/news/medicaidproviders-penalized-illegal-dentalsolicitation.
7. Texas Office of Inspector General. Access June 2022, https://oig.hhs.texas.gov/ about-us/news/oig-expands-illegal-dentalsolicitation-education-effort.
624 Texas Dental Journal | Vol 139 | No. 10
files/documents/reports/quarterly_ report_qtr1_fy2022.pdf •
files/documents/reports/quarterly_ report_quarter_2_fy2022.pdf • https://oig.hhs.texas.gov/sites/default/ files/documents/reports/quarterly_ report_quarter_3_fy2022.pdf
The OIG’s quarterly reports include information about Medicaid dental cases and recoveries. Cases covered upcoding, billing for services not rendered, missing or inadequate documentation, medically unnecessary services, and failure to meet the professional standard of care. It is very
that dentists only bill for services provided, always bill the correct procedure codes, and maintain proper documentation in the patient’s dental record.
A 2019 contract amendment requires DMOs to maintain a full-time SIU manager and credentialed investigator dedicated to examining improper claims by Texas Medicaid members and service providers.
SPECIAL INVESTIGATIVE
UNITS
HELP PREVENT FRAUD, WASTE AND ABUSE
Texas Health and Human Services (HHS) spends approximately $43 billion in public funds annually to deliver benefits that include Medicaid and the Children’s Health Insurance Program (CHIP). The HHS Office of Inspector General (OIG) helps ensure those tax dollars are used for their intended purpose. The OIG’s mission is to prevent, detect and investigate fraud, waste and abuse (FWA) in HHS programs, including dental services delivered through Medicaid and CHIP.
While the OIG recovers tax dollars lost to wrongdoing, the agency endeavors to prevent fraud from happening in the first place. Educating stakeholders across the health care system helps do that. Knowing that the majority of dental providers take pride in their work and deliver excellent care to their patients, the OIG works with dentists to minimize waste and costly billing errors.
HELPING DMOS ENGAGE PROVIDERS
Collaboration between the OIG and dental maintenance organizations (DMOs) plays an important role preventing and identifying FWA in Medicaid and CHIP delivery. One tool used by DMOs for accomplishing this is their special investigative units (SIUs), which investigate possible provider acts of FWA for all services provided under each DMO’s contract with Texas Medicaid. The OIG works with DMOs to ensure their SIU annual plans contain the required elements, and the OIG has a dedicated SIU coordinator who assists with referrals, investigations and FWA training.
A 2019 contract amendment requires DMOs to maintain a full-time SIU manager and credentialed investigator dedicated to examining improper claims by Texas Medicaid members and service providers. Since that time, the OIG also increased outreach to DMOs and managed care organizations (MCOs) through the Texas Fraud Prevention Partnership to assist in identifying, investigating and referring more cases. These changes likely contributed to the 33 percent increase in SIU referrals to the OIG for provider investigation from fiscal year 2020 to 2021.

www.tda.org | October 2022 625
PROVIDER INVESTIGATIONS
SIUs engage with dental providers when fraud allegations arise, whether through a referral or data-generated initiatives from a DMO. Preliminary investigations can lead to a record review to determine if suspicious billing patterns are due to fraud or some other issue. A DMO may then choose to take action against the provider, such as requiring prepayment claims reviews to conducting postpayment claims audits, and/or terminating a provider’s contract with the DMO network.
CONTAINING COSTS THROUGH SIUS
Effective SIUs are essential to support overall DMO cost containment efforts. The OIG routinely audits SIU activities to check compliance with state and contractual requirements. DMOs are contractually required to provide the OIG with the following:
• Fraudulent practices referrals
• Fraud, waste and abuse compliance plans
• Open case list reports
• Annual lock-in actions reports
• Annual reports on certain fraud and abuse recoveries
• Pre-payment review monthly reports
OIG audits examine DMO compliance related to preventing, detecting and investigating FWA and reporting information on SIU activities, results and recoveries to HHS. Audits examine whether DMOs have the required staff, conduct training and monitor provider and member service patterns. Through the audit process, the OIG verifies that the SIUs ensure investigations include all required elements, maintain a log of suspected incidences of FWA, and meet deadlines for submitting required reports and referrals to the OIG.
The OIG makes recommendations to DMOs based on audit findings. Working with DMOs on process improvements related to SIU activities helps maintain efficient and effective fraud prevention and detection and helps DMOs effectively work with providers. You can explore the audits of various SIUs on the OIG website.
TEXAS FRAUD PREVENTION PARTNERSHIP
The OIG regularly engages with SIUs through the Texas Fraud Prevention Partnership (TFPP). Meetings are held 3 times each year with all SIUs and the Office of the Attorney General Medicaid Fraud Control Unit to share insights and information. The gatherings provide an opportunity for the OIG to discuss referrals, provider and client investigations, and best practices for compliance. DMO representatives report on the improper billing patterns they observe. The OIG also holds one-on-one meetings with SIU staff of each DMO to discuss their investigations and current trends in FWA. Additionally, the Inspector General and executive staff meet with the executive leadership of the DMOs periodically.
Dental providers who discover their own discrepancies are encouraged to self-report the matter to their DMO or to the OIG’s Fraud Hotline at 800-436-6184 or website, ReportTexasFraud.com.
626 Texas Dental Journal | Vol 139 | No. 10
To learn more about the Office of Inspector General: Facebook: www.facebook.com/TxOIG Twitter: www.twitter.com/TexasOIG LinkedIn: hhsc-office-ofinspector-general
TDA has a proven track record of achieving insurance victories for its members.
YOUR INSURANCE ADVOCATE
Texas Dental Association (TDA) members identify dental benefits and third-party payer issues as their top concerns. TDA is committed to helping its members navigate the complicated laws and regulations associated with dental insurance and third-party payers. In collaboration with the American Dental Association (ADA) and TDA’s Council on Professions and Trends, TDA is your trusted resource for information about how best to address your insurance issues.
In addition to the resources TDA makes available on its website, TDA has a proven track record of achieving insurance victories for its members. Working closely with the various insurance plans (including Medicaid managed-care plans), the Texas Department of Insurance (TDI), and the Texas Health and Human Services Commission (HHSC), TDA successfully addresses issues members are facing every day.
PERSONALIZED ASSISTANCE
TDA’s PERSONALIZED THIRD PARTY PAYER ASSISTANCE
Coding? Denied claims? Overpayments? Coordination of benefits? TDA offers personalized help with third party payer and insurance issues. Call Debbie Rogers at 512-443-3675, ext. 152 or email her at drogers@ tda.org.
TDA’s PERSONALIZED INSURANCE & REGULATORY ASSISTANCE
Need help understanding insurance statutes or state insurance regulations? Call Diane Rhodes at 512-4433675, ext. 122 or email her at drhodes@tda.org.
ADA’s THIRD PARTY PAYER CONCIERGE
ADA offers free assistance for member dentists with insurance questions and concerns with third party payers. Call 1-800-621-8099 or email dentalbenefits@ada.org.

UNDERSTANDING COVERAGE & CONTRACTS
Patients’ insurance benefits vary considerably in coverage, treatment limitations, and fee schedules. For dentists deciding to be in a network’s plan, it is important to read the contract carefully before signing it. When you sign an insurance contract and become a participating provider, you are making a legally binding promise.
www.tda.org | October 2022 627
The most important thing for a dentist to know when facing an insurance dispute is whether the patient’s plan is regulated by the State of Texas or the federal government.
Most Texans are covered by self-funded insurance plans, in which the plan sponsor (most often the patient’s employer) is responsible for claims payments and hires a carrier to administer the plan and process claims. Self-funded dental plans are governed by a federal law called ERISA (Employee Retirement Income Security Act). ERISA plans are exempt from most state insurance laws.
You should also always submit your full fee to the insurance carrier. Many large carriers monitor the fees submitted on dental claims. They then analyze those fees to establish the “usual and customary rates” for the participating dentists in each market. If contracted dentists only bill the contracted rates, this will inadvertently bring down the “average” fees in each market area. This is not only misleading, but potentially harmful down the road as it may encourage carriers to lower their fees. Additionally, billing your full fee ensures that you receive the highest fee available on that service date.
For dentists choosing not to participate in-network with a patient’s insurance plan, it is still important to know what dental services are covered by a patient’s plan, specifically the plan’s limitations and exclusions.
ADA CONTRACT ANALYSIS
ADA offers a free contract analysis service for its members. If you would like to submit a contract for analysis, or if you have any questions regarding the contract analysis service, please contact Debrah Rogers with the TDA Department of Member Services by phone at 512-443-3675 ext. 152 or by email at drogers@tda.org.
ADDRESSING INSURANCE DISPUTES—
STATE V. FEDERAL PLANS
The most important thing for a dentist to know when facing an insurance dispute is whether the patient’s plan is regulated by the State of Texas or the federal government.
Most Texans are covered by self-funded insurance plans, in which the plan sponsor (most often the patient’s employer) is responsible for claims payments and hires a carrier to administer the plan and process claims. Self-funded dental plans are governed by a federal law called ERISA (Employee Retirement Income Security Act). ERISA plans are exempt from most state insurance laws.
Fully insured plans are qualified health insurance plans, in which contributions are made to an insurer and the insurance company provides the plan’s benefits and administers the plan on behalf of the plan’s participants. Fully insured plans are regulated by TDI and state insurance law.
To determine whether the patient’s insurance is ERISA or state regulated, check their insurance card. State regulated plans will have the initials “TDI” or “DOI.” You can also look for language such as “ERISA plan, Managed by…” or “Administered by…” to identify ERISA plans.
You will often find these notations on the lower left-hand corner of the insurance card. If you do not have a copy of the patient’s insurance card, you will need to ask the patient or contact their insurance carrier to ask them.
Additionally, self-funded ERISA plans are required to file a Form 5500 with the US Department of Labor. Search the Form 5500 database online at freeerisa.benefitspro. com to determine if a plan is self-insured.
628 Texas Dental Journal | Vol 139 | No. 10
INSURANCE COMPLAINTS— WHERE TO GO
Self-Funded Insurance Plans
(ERISA):
File complaints against self-funded plans with the US Department of Labor online at www.askebsa.dol. gov/webintake/home.aspx
State-Regulated Insurance Plans:
File complaints with TDA through their online complaint system at www.tdi.texas.gov/hprovider/ providercompl.html
COMMON TYPES OF INSURANCE PRODUCTS
It is important for you to know the type of commercial insurance product your patient is using. This list is not exhaustive, but includes information on the most common patient plan options.
Dental Preferred Provider Organization (DPPO or PPO)
In this model, the insurer creates a network of providers for patients to choose from that are contracted to the insurance company to perform dental services for set fees according to the provisions of the contract. Contracted dentists usually must accept the maximum allowable fee as dictated by the plan, but non-contracted dentists may have fees either higher or lower than the plan allowance. Patients are free to see dentists outside the network, but usually at higher out-ofpocket costs. DPPOs typically cover all in-network preventative care, but have co-payments for restorative work and orthodontia up to the patient’s annual allowable maximum.
Dental Health Maintenance Organization (DHMO or HMO)
These plans utilize a network of providers, and patients are typically required to pick a primary provider and stay in network in order to get the full benefit of their plan. Dentists are paid based on the number of patients on the DHMO. This is often referred to as a capitated payment model.
Dental Indemnity Insurance
An indemnity plan is traditional dental insurance. There are no provider networks, and the dentist gets paid their usual fees. These plans have deductibles and co-payments like DPPOs.
LEGISLATIVE ACHIEVEMENTS AND AGENDA
TDA has achieved numerous victories for Texas dentists in almost every legislative session, and there is still more to be accomplished. In the 88th Legislative Session convening in January 2023, TDA will work with lawmakers to address three key insurance issues affecting dentists and patients –retroactive denials, silent network leasing, and disallowable clauses in contracts. Here are some of the dental insurance reform measures TDA has successfully taken on in previous sessions.
In 2019, TDA secured passage of historic comprehensive reform for state-regulated insurance that brought much needed relief to dentists through HB 2486. The bill required stateregulated insurance plans to have a free website available for patients and dentists that includes information about the patient’s plan or policy. It also prohibited these plans from mandating
payment methods to dentists. HB 2486 required state-regulated insurance plans to pay for dental treatment that has been prior authorized. It also prevented the insurers from collecting an “overpayment” from a dentist who did not treat the patient where the overpayment occurred.
TDA achieved coordination of benefits (COB) protection for dentists in 2015 with the passage of HB 3024. That bill required state-regulated insurance plans to coordinate a patient’s primary and secondary insurance so that they secondary insurer also pays on a dental claim up to, but not exceeding, 100 percent of the total amount of the claim. When both plans have COB provisions, the plan in which the patient is enrolled as an employee or the main policyholder is primary. The plan in which the patient is enrolled as a dependent would be secondary.
In 2011, TDA attained non-covered services protection for dentists through the passage of SB 554. State-regulated dental plans are prohibited from setting fees for dental services not covered by the plan. The only fees a dental plan may cap are fees for services the plan covers.
TDA accomplished assignment of benefits protection for dentists in 2003, preventing state-regulated insurance plans from prohibiting or restricting a patient from making a written assignment of benefits to a dentist.
TDA will continue working with legislators and regulators to eliminate insurance issues plaguing dentists. TDA’s success at the Capitol begins with your involvement and grassroots efforts, and with your help TDA will continue to make significant insurance improvements for Texas dentists.
www.tda.org | October 2022 629
TDA Legislative Resource Guide Resources
The staff at the Texas Dental Association stands ready to assist you. Please use this guide to identify staff members who are knowledgeable in areas of legislative and regulatory affairs. If you have questions or need assistance with any of these entities, or others not listed, please give us a call.
General Legislative & Regulatory Questions
1946 S IH35, Ste 400, Austin, TX 78704 512-443-3675, ext. 270
Director of Public Affairs Jess Calvert 512-443-3675, ext. 132 jcalvert@tda.org
Senior Policy Manager Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Policy Analyst/PAC Coordinator
Staci Rives 512-443-3675, ext. 123 srives@tda.org
DENPAC
1946 S IH35, Ste 400, Austin, TX 78704 512-443-3675, ext. 123
Texas State Board of Dental Examiners
333 Guadalupe, Tower III, Ste 800 PO Box 13165, Austin, TX 78701
P 512-463-6400
F 512-463-7452 www.tsbde.texas.gov
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Office of Inspector General
Chief Dental Officer
Dr Janice E. Reardon
PO Box 85200, MC-1300, Austin, TX 78708 512-491-2060 janice.reardon@hhsc.state.tx.us
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Health and Human Services Commission
Texas Medicaid and CHIP Division
Dr Marguerite Laccabue MPH, Dental Director
11501 Burnet Rd, Bldg 902 #309 Austin, TX 78758 512-491-5674 marguerite.laccabue@hhsc.state.tx.us
Texas Department of State Health Services
Oral Health Improvement Program Dr Rhonda Stokley
Public Health Dental Director
MC 1938 PO Box 149347, Austin, TX 78714 1100 W 49th St, Austin, TX 78756 512-776-2008 rhonda.stokley@dshs.texas.gov
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Insurance
Texas Department of Insurance 333 Guadalupe, Austin, TX 78701 800-578-4677 www.tdi.texas.gov
Provider Resources 800-252-3439 www.tdi.texas.gov/hprovider/index.html
Department of Insurance Consumer Protection 800-252-3439 www.tdi.texas.gov/consumer/complfrm.html
TDA Staff: Lee Ann Johnson 512-443-3675, ext. 134 ljohnson@tda.org
Medicaid and CHIP
Texas Medicaid & Healthcare Partnership
General Inquiries Line: 800-925-9126
Provider Enrollment: 800-925-9126, option 3 www.tmhp.com
Texas Health Steps Dental
877-847-8377 www.hhs.texas.gov/doing-businesshhs/provider-portals/health-servicesproviders/texas-health-steps/dentalproviders
DentaQuest 800-896-2374 dentaquest.com/state-plans/regions/ Texas/dentists
MCNA Dental 1-855-PRO-MCNA (776-6262) www.mcnatx.net/dentists/#resources
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Children’s Health Insurance Plan
(CHIP)
Providers
Customer Service Department PO Box 537014 Sacramento, CA 95853-7014 866-561-5891 deltadentalins.com/dentists.html
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
630 Texas Dental Journal | Vol 139 | No. 10
Professional Recovery Network
Statewide Toll-Free Help Line 800-727-5152 txprn.com
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
X-Ray Unit Certification
Texas Department of State Health Services Radiation Control Program
Attn: Registration 1100 W 49th St, Austin, TX 78756 888-899-6688 dshs.texas.gov/radiation
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Prescriptions
DEA Diversion Control Program deadiversion.usdoj.gov 800-882-9539 dea.registration.help@usdoj.gov
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Texas Prescription Monitoring Program
333 Guadalupe, Ste 3-500
Austin, TX 78701 512-305-8050 texaspmp@pharmacy.texas.gov www.pharmacy.texas.gov/pmp
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Infection Control and OSHA
Occupational Safety and Health Administration (OSHA)
US Department of Labor Occupational Safety and Health Administration 200 Constitution Ave, NW Room Number N3626 Washington, DC 20210 800-321-OSHA (6742) osha.gov/dentistry
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
Area OSHA Offices:
Austin: 512-374-0271
Corpus Christi: 361-888-3420
Dallas: 972-952-1330
El Paso: 915-534-6251
Fort Worth: 817-428-2470
Houston (North): 936-760-3800 Houston (South): 281-286-0583
Lubbock: 806-472-7681 San Antonio: 210-472-5040
Environmental Regulations
Texas Commission on Environmental Quality (TCEQ)

PO Box 13087, Austin, TX 78711 512-239-1000 tceq.texas.gov
TDA Staff: Diane Rhodes
512-443-3675, ext. 122 drhodes@tda.org
Tax Issues
Texas Comptroller of Public Accounts
PO Box 13528, Capitol Station
Austin, TX 78711
888-334-4112 comptroller.texas.gov
TDA Staff: Diane Rhodes 512-443-3675, ext. 122 drhodes@tda.org
631

632 Texas Dental Journal | Vol 139 | No. 10 • Representation Before the Texas State Board of Dental Examiners • Medicaid Audits and Administrative Hearings • Employment Issues—Texas Workforce Commission Hearings • Administrative (SOAH) Hearings and Counsel • Professional Recovery Network (PRN) Compliance • Employment/Associateship Contract Reviews • Practice Acquisition and Sales • Business Organizations, PAs, PCs, and PLLCs • Civil Litigation 2414 Exposition Blvd., Suite A1 • Austin, Texas 78703 • Phone: 512-477-6200 • Fax: 512-477-1188 • Email: mhanna@markjhanna.com Not Board Certified by the Texas Board of Legal Specialization Mark J. Hanna JD Former General Counsel, Texas Dental Association LAW OFFICES OF MARK J. HANNA EXPERIENCED LEGAL REPRESENTATION FOR TEXAS DENTISTS
Dental Practice Valuation
Free
Take the 1st step in selling your dental practice. Contact us to receive a free practice valuation. Terry Watson, D.D.S. Jeremy Brown, J.D. Frank Brown, J.D., LL.M. 469-222-3200
ORALand maxillofacial pathology case of the month
Case History
This case concerns a 68-year-old male patient who presents with an asymptomatic radiolucency within the crown of tooth #6. The lucency extends to the dentino-enamel junction, is poorly circumscribed, and has a moth-eaten appearance (Figure 1 A&B). Within the more coronal aspects of the dental crown, an ill-defined radiopacity is noted.
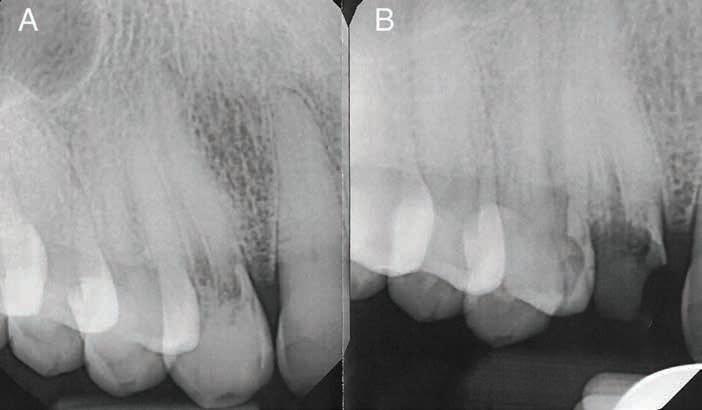
There was no history of trauma, and no visible discoloration of the tooth. No caries was evident on clinical or radiographic exam.
During preparation of the tooth for a crown, blood was observed weeping through the dentin surfaces. The tooth was judged to be non-restorable, and the extracted root tip was submitted for histopathologic evaluation.
Microscopic examination reveals tubular dentin containing
AUTHOR
John E. Kacher, DDS Director, JKJ Pathology

Oral Medicine—Oral Pathology
The Woodlands, Texas
pulp comprised of loose connective tissue containing an infiltrate of lymphocytes. Toward the coronal aspect of the root tip, replacement of the dentin with osseous-type tissue exhibiting marrow spaces, woven bone, and osteocytes in lacunae is noted. The junction between the dentin and osseous material is continuous (Figure 2 A&B).
What is your differential diagnosis?
What is your final diagnosis?
See page 643 for the answer and discussion.
Figure 1A and B.
Figure 1A: Ill-defined radiolucency within the canal space of tooth #6. The crown exhibits obliteration of the pulp chamber that is filled with material that has intermediate radiodensity between dentin and bone.
Figure 1B: After crown preparation most of the radiodense material has been removed, and the remaining lucency appears moth-eaten.
634 Texas Dental Journal | Vol 139 | No. 10
Figure 2B. Tubular dentin and osseous replacement tissue. The interface between the two tissues is irregular, which belies the resorption of dentin prior to replacement with osseous tissue.
www.tda.org | October 2022 635
Figure 2A. Tubular dentin of the root with central pulp tissue. The internal walls of the dentin exhibit replacement with osseous-type tissue.
LESS CHAIRSIDE,
EXPERT witness training DAY ONE - learnDAY TWO - experience -
Are you a Dentist who is becoming tired of working chairside, near the end of your career, or merely looking for supplemental income? Dental Expert Witness work could be the answer for you!
Until now there have been no lectures and no instruction available on what it is, what it takes, and how to market yourself as an Expert Witness. Our exclusive workshop is the first ever of its kind!
Using their 30 years of experience, Dr. Boeke DDS & Dr. Krueger DDS/JD have created a 2 day workshop on the beautiful Texas A&M-Commerce campus, that will teach you the ins and outs of becoming an Expert Witness in a way that is informative, effective, and fun.
- what it is to BE a Dental Expert Witness



how it helps serve your peers and community
how it generates additional income
of the chair
to market yourself as an Expert Witness.
an exclusive experience,
Dr. Krueger’s firsthand records and depositions of trials past

mock testimonies based on those trials, complete with testimony from a witness stand
end your day with a Texas BBQ experience on Dr. Boeke's Ranch
to 10 seats per month!
SEPTEMBER & OCTOBER
636 Texas Dental Journal | Vol 139 | No. 10 $7,500 $5,000 FOR
2022 For more information, and to reserve your seat, please visit www.dentalexpertwitnesstraining.com
MORE INCOME DENTAL
-
-
outside
-how
-
-
-
For
our program is limited


www.tda.org | October 2022 637 JKJ Pathology Oral Pathology Laboratory John E Kacher, DDS ¥ Available for consultation by phone or email ¥ Color histology images on all reports ¥ Expedited specimen shipping with tracking numbers ¥ Reports available online through secure web interface Professional, reliable service with hightechnology solutions so that you can better serve your patients. Call or email for free kits or consultation. jkjpathology.com 281-292-7954 (T) 281-292-7372 (F) johnkacher@jkjpathology.com Protecting your patients, limiting your liability Calendar of events Due to COVID-19, please check each meeting’s website for up-to-date information related to cancellations or rescheduling. THE TEXAS DENTAL JOURNAL’S CALENDAR will include only meetings, symposia, etc., of statewide, national, and international interest to Texas dentists. Because of space limitations, individual continuing education courses will not be listed. Readers are directed to the monthly advertisements of courses that appear elsewhere in the Journal TMOM 2022 SCHEDULE Dallas—November 4-5, 2022 TMOM 2023 SCHEDULE TMOM Bonham: April 14-15, 2023 TMOM Abilene: July 14-15, 2023 SMILECON Houston—October 13-15, 2022 House of Delegates, October 15-18
VALUE for your profession
Provided by:

2023 Open Enrollment and ACA Update
By Eric Tiedtke, CFP TDA Financial Services Insurance Program
What follows is TDA Financial Services Insurance Program’s annual update on health insurance. For 2023, there’s been quite a bit of legislation passed and more changes ahead for individual and small group markets. For instance, the subsidies for the Affordable Care Act (ACA) individual plans were extended under the recently passed Inflation Reduction Act; and there are new companies offering plans in Texas and options to consider.
Slight Rate Increases or Decreases for Individual HMOs, Slight Rate Increases for Small Groups
If you have individual or small group coverage, there are changes coming. Filed rates are being reviewed to determine if proposed increases are based on reasonable cost assumptions and solid evidence. Final rates won’t be available until November 1 when open enrollment starts, so you can’t really start comparing until then.

And after 5 years of most major insurance companies (other than Blue Cross) leaving the individual market in Texas, some new options will be available—not only in individual but also small-group markets.
Individual Plans
Blue Cross will again be the only company offering individual plans statewide in Texas, and they will again be HMO only. Blue Cross filed for a 3.52% increase on their most popular HMO. The other individual plans offered in Texas—United Healthcare, Humana, Aetna, Community Health, Molina, and Friday Health Plan—filed for higher rate increases in the range of 10% to 30%, so keep an eye out for your renewal.
638 Texas Dental Journal | Vol 139 | No. 10
There are no ACA-compliant individual PPO plans in Texas (at the time of this writing in mid-August). There are regional or local plans available in Texas—mostly HMOs—and in limited areas of the state where a hospital system has several facilities and offers a plan.
United Healthcare & Cigna are supposed to have new individual plans available. We anticipate these to be Exclusive Provider Organization (EPO) plans, which are like PPOs with no or limited out-of-network coverage. Plan details were not available at the time this article was written.
There are other companies offering individual plans in a few select major metropolitan areas; such as Friday Health Plan, Molina, Oscar, and Scott & White; and a few hospital-specific plans. Keep in mind the network being offered, as it could have limited or no coverage in parts of the state. Most of the plans incorporate tele-med, direct primary care, or concierge medicine as part of the coverage.
• Tele-med allows virtual visits with your physician that may or may not have a copay.
• Direct primary care and concierge arrangements typically provide certain services—such as an annual physical exam and specified treatment for a specific condition—and often don’t qualify as insurance, as you’re essentially pre-paying for a service.
• Virtual primary care sessions can include some prescriptions, durable medical equipment, lab tests, and diagnostic imaging.
Again, it’s very important to understand the scope of the networks, the coverage, and limitations—especially if you’re seeing specialists for an ongoing medical condition.
Don’t forget about subsidies or premium credits.
The ACA’s health insurance premium subsidies—also known as premium tax credits—normally adjust each year to keep pace with premiums. But for 2021 and 2022, subsidies are much more robust than they usually are. There is no “subsidy cliff” for this 2-year period. Instead, no one purchasing coverage through the marketplace must pay more than 8.5% of their household income. And people with lower incomes are expected to pay a smaller-thannormal percentage of their income for the benchmark plan—as low as $0 for people with income that doesn’t exceed 150% of the poverty level.
The eligibility range was capped at household incomes of 400% of the federal poverty level (FPL). But that changed for 2021 and 2022. Pending legislation would eliminate the income cap for subsidy eligibility through 2025.
Small Group Plans
Small group plans continue to be the only option for getting true PPO plan options under the ACA.
Rate changes filed for small group plans range from less than 5% to as high as 26% depending on the company. For 2023, it appears small group:
• PPO rates will again be slightly lower than individual HMO rates.
• HMO group rates will be 5% to 15%
lower than individual plans (nonsubsidized).
Of the major companies, we anticipate Blue Cross will have the lowest rates (their filed rate increase for the PPO and HMO is around 4.5%) followed closely by United Healthcare, Humana, and Aetna. Friday Health Plan is expanding in Texas, but only in select metropolitan areas of the state, including DFW, Houston, Austin, and San Antonio.
Coverage Options
Small-Group Plans: Less Expensive than Individual Plans, More Options
If you have a practice with at least one other full or part-time employee, you should consider a small group plan. Depending on how your practice is structured, the other employee could be your spouse. Contact TDA Financial Services Insurance Program at (800) 677-8644 for details.
Why go through the additional paperwork and effort for a small group?
• Small group plans will be less expensive than the individual plans, and you can still get a PPO.
• If you sign up during the special enrollment for new small groups (starting Nov. 1), the mandatory employer contribution towards employee premiums (as well as other requirements) are waived. This is a good way to attract and retain high-quality employees while offering a lot of flexibility on plan designs.
• If you payroll deduct the employee premiums, it saves the practice and employees on taxes.
• You can offer more than one plan
www.tda.org | October 2022 639
VALUE continued
within your group—a base plan that’s less expensive for employees (perhaps an HMO with an Rx and office copay) and a PPO plan for you and your family.
We can start comparing rates for small group plans beginning October.
Here are the maximum out-of-pocket amounts for coverage in 2023:
In-network
• $9,100 for an individual
• $18,200 for a family
High-deductible plans intended to be HSA-compatible are subject to these out-of-pocket maximums:
• $7,500 for individual coverage
• $15,000 for family coverage
Out-of-network
If you have out-of-network expenses, the maximum can be double what’s listed above or more; or out-of-network expenses might not even be covered. The plans with the lowest premiums will have the highest out-of-pocket expenses.
This is Important.
It’s critical you check the network of the insurance company you select for 2023 and make sure your providers and hospitals are in-network. You need to know the company name and the network name. Some providers, for instance, might take a Blue Cross PPO, but not Blue Cross HMO.
What other options do I have for health insurance in 2023?
Level-Funded plans
If your practice and its employees are generally healthy and not big users of health care, you might want to consider a level-funded plan. These are underwritten based on the health of the group and can be as much as 10% to 25% lower than regular ACA small group plans.
Keep in mind only 40% of groups will qualify based on underwriting, so this will not be a fit for all practices. Also, they typically don’t qualify for the special enrollment, so the practice must pay 50% of the employee premium and meet a participation requirement regarding the number of eligible employees that participate. Additionally, there are other considerations, such as the different PPO networks, stop loss coverage, and just understanding how the plans work and what’s covered.
Faith-Based, MediShare and HealthShare Groups
These types of plans are not insurance and should not be considered a substitute. With these types of arrangements, you join a group and pay or contribute a monthly amount to the plan. After your deductible is met, you submit your medical bills and are
reimbursed from the funds available or through others making additional contributions to cover your bill. Many have incorporated a PPO network, so you can get the discounted amount when you have treatment. However, remember you’re still responsible for the bill even if the health-share plan might reimburse you.
These arrangements also have stricter guidelines than traditional insurance companies on which procedures are eligible for reimbursement or cost sharing. As well, there’s normally a lifestyle guideline where a member agrees to live a certain way (abstain from illegal drug consumption, sex outside of marriage, tobacco use, and abuse of alcohol or prescription drugs). The payments of medical bills through these arrangements are not guaranteed in any way. Each member is always solely responsible for the payment of his or her own medical bills.
If you understand how the plans work and their limitations, these can be a less expensive option than ACA plans.
Short Term Medical
We don’t recommend you go without insurance; however short-term health insurance is an option if you’re without coverage because of a waiting period, you’re transitioning from one plan or coverage to another (e.g., in-between jobs), it’s outside the open enrollment period, or you’re close to being eligible for Medicare.
640 Texas Dental Journal | Vol 139 | No. 10
These plans are exempt from the definition of individual health insurance coverage under ACA provisions and usually don’t pay for pre-existing conditions. They’re designed to cover a new sickness or accident, with no treatment in the previous five years. They also have limitations on coverage (e.g., no maternity coverage) and don’t have all the same mandates, such as unlimited-benefits maximums. The good news is these plans are available for up to 12 months of coverage and may be renewed for up to 36 months.
Limited Benefit
Sickness-and-Accident Plans
These plans are sometimes called “minimed plans” and are marketed as an ACA alternative with a PPO.
They may offer copays and Rx benefits, however, they don’t include the “essential minimum health benefits” required by the ACA.
These types of plans may include a PPO and provide a schedule of benefits that pay a certain amount per day or treatment and are limited to a maximum amount. A company selling these plans will often address this limitation by selling additional coverage for critical or specified illness.
These are underwritten based on good health and have some form of pre-existing condition limitation, which means anything you’ve previously been treated for is not covered for a period—normally 12 months. If the plan is guaranteed issue with no pre-existing condition, make sure you’re not just buying a discount plan.
These plans can be an option, however you need to really understand the limitations and coverage, as you could be responsible for tens of thousands of dollars—even if you’re covered—if you have a major accident or illness.
Additional Options and Considerations
If you’re concerned about having a high deductible, limited, or no out-ofnetwork coverage, you might consider a supplemental product for accidents or hospital confinements. These types of plans pay you directly and in addition to your other coverage. They tend to be relatively less expensive and are a good option if you don’t want to self-insure high-deductible and out-of-pocket expenses.

HSA Plans
When picking a plan, keep the above numbers in mind, but also consider the following. Prescription-drug and office-visit copays are convenient plan features, but you need to know the combined cost of your total out-ofpocket exposure and your plan (the premium).
If you haven’t looked at HSA plans or didn’t think they made sense previously, you should look at them.
• HSA plans offer the lowest premium and can be a great way to build up a self-funding account for current and future medical expenses. This can be especially important if you have to go out-ofnetwork.
• Contributions are tax deductible (as much as $4,850 for an individual and $8,750 for a family).
• Earnings and interest accumulate tax-free.
• You own and control the funds.
• HSA plans are not a use-it or-lose-it vehicle.
www.tda.org | October 2022 641
VALUE continued
ICHRA
Individual Coverage Health Reimbursement Arrangement (ICHRA) presents an opportunity for employers to take more control over their benefits spend. An ICHRA allows them to set aside tax-advantaged dollars to reimburse their employees for individual health insurance plans; and is inflation-resistant compared with group plan premiums. ICHRA brings more cost control and less risk for the employer and more purchasing power and choice for employees.
Keep in mind, however, that the individual health insurance plans offered are probably going to be HMO only; so no PPO. Additionally, the individual HMO plans are 10% to 15% higher than the group HMO plan, if unsubsidized. There’s also the ICHRA set up and additional administration for the practice, which isn’t particularly burdensome but should be taken into account.
HRA
Use of Health Reimbursement Accounts (HRAs) expanded because new regulations issued by the Departments of Labor, Treasury, and Health and Human Services, allow reimbursements for individual-market insurance premiums.
Before employers offer a benefit that includes individual HRAs, they should consider the implications related to the (ACA) employer shared-responsibility mandate and the ability of their employees to obtain a premium tax credit (PTC) or subsidy on the ACA marketplace. Because of this indexing methodology, the maximum newcontribution amount for an excepted benefit HRA remained $1,950 for 2023 plan year.
2023 Landscape Review
If you want or need full coverage, the small group market is still the best way to get coverage with more options available at lower cost than in the individual market. However, with proposed legislation, this could definitely change in 2023—so keep your ears open!
The alternative options discussed all have a place at the table, but you need to make sure you understand plan limitations and risks before making a change to something less expensive. Stay informed and get ready to review and compare your options and decide as soon as possible. You’ll be able to review individual plans and rates beginning November 1 and small group plans and rates in early October.
Important Dates
The open enrollment period for health plans offered under ACA begins November 1, 2022, with the effective date of January 1, 2023. For individual plans, you’ll have until December 15 to pick or change to a new plan with a Jan. 1 effective date; or until December 31, if your plan terminates December 31.
Please note: This article was submitted the mid-August, so some information may have changed by the time this article is published.
If you would like to receive more information or discuss available insurance options, please feel free to contact TDA Financial Services Insurance Program at (800) 677-8644 or visit www. tdamemberinsure.com.
642 Texas Dental Journal | Vol 139 | No. 10
ORALand maxillofacial pathology
Internal Resorption, Replacement Type
Discussion
Internal root resorption is a class of pulpal disease characterized by loss of dentin secondary to clastic activity derived from inflammation. The source of the cells involved in the resorptive process are from the dental pulp in internal resorption, and from the periodontal ligament in external resorption.1
For internal resorption, prior trauma is commonly cited as a predisposing factor. This could be either physical trauma or caries-related pulpitis. Internal resorption is much less common than external resorption. Orthodontic tooth movement is a risk factor for external root resorption.
Two patterns are associated with internal resorption: inflammatory resorption, and replacement resorption. For inflammatory resorption dentin is replaced by inflamed granulation tissue. The cervical portion of the tooth is most frequently affected with this pattern.
This case is an example of replacement resorption, whereby the dentinal wall is resorbed and replaced with bone or cementum-like bone. The radiographic presentation shows an enlargement of the canal, which is filled by a material that is less radiodense than the surrounding dentin. Obliteration of the canal may be observed.
Inflammatory resorption typically presents as a balloon-like radiolucent dilation of the canal space. When this process becomes progressive enough, the external visible appearance of the tooth can become pink due to showthrough of the vascular tissues just below the tooth surface. This effect is termed “Pink tooth of Mummery”.
It has been suggested in the literature that the receptor-ligand system RANKL/RANK/OPG plays an essential role in bone remodeling and also in external dental resorption cases.2 The biomolecular pathway for internal resorption is not well understood.
Sometimes it can be difficult to distinguish external from internal root resorption due to the radiographic presentation of a lucency superimposed on the tooth root. Either multiple radiographs can be used to expose the lesion from various angles, or cone beam imaging accomplished to elucidate the precise location of the lesion.4
Treatment of internal resorption can include endodontic therapy if the lesion has not yet perforated into the PDL. More recent literature suggests that with modern Endodontic techniques, the prognosis is good even in cases where the walls of the root canal system are perforated.3 However, since the lesion is asymptomatic, frequently lesions enlarge beyond this point before
they are discovered. If this happens the tooth can be extracted and an implant subsequently placed.
Thanks to Dr Edward Estrada for contributing this case.
References
1. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology, 2nd edition.
Philadelphia: WB Saunders Company 2002; location 2785.
2. Pathophysiological mechanisms of root resorption after dental trauma: a systematic scoping review, Kerstin MG et al, BMC Oral Health:163 (2021).
3. Management of Internal Root Resorption on Permanent Teeth, Nilsson E et al, International Journal of Dentistry, 2013, PMID 929486.
4. Radiological and Histopathological Features of Internal Tooth
Resorption, Koehne T et al, in vivo, July 2020 34(4) 1875-1882.
www.tda.org | October 2022 643
diagnosis and management—from page 635
ADVERTISING BRIEFS
PRACTICE OPPORTUNITIES
ALL TEXAS LISTINGS FOR MCLERRAN & ASSOCIATES. TO REQUEST MORE INFORMATION ON OUR LISTINGS: Please register at www.dentaltransitions.com or contact us at 512-900-7989 or info@ dentaltransitions.com. AUSTIN (ID #556):
Opportunities Online at TDA.org and Printed in the Texas Dental Journal
ADVERTISING BRIEF INFORMATION
DEADLINE
Copy text is due the 20th of the month, 2 months prior to publication (ie, January issue has a due date of November 20.)
MONTHLY RATES
PRINT: First 30 words—$60 for ADA/TDA members & $100 for non-members. $0.10 each additional word.
ONLINE: $40 per month (no word limit). Online ads are circulated on the 1st business day of each month, however an ad can be placed within 24 business hours for an additional fee of $60.
SUBMISSION
Ads must be submitted, and are only accepted, via www.tda.org/Member-Resources/TDAClassified-Ads-Terms. By official TDA resolution, ads may not quote specific incomes or revenues and must be stated in generic terms (ie “$315,000” should be “low-to-mid-6 figures”). Journal editors reserve the right to edit and/or deny copy.
100% fee-for-service GD practice in north Austin. The approximatelyh 2,300 sq ft, fully equipped, 6 operatory office features computers in operatories, digital radiography, X-ray sensors, intra oral cameras, and paperless charts. The practice serves a large patient base with a robust hygiene recall program. AUSTIN-WEST (ID #539): 100% feefor-service practice in the Texas hill country with strong hygiene recall (approximately 30% of total production) and an increasing revenue trend over the past 3 years. The practice is located in a free-standing building that features 3 fully equipped operatories, newly installed computers in each room, digital sensors, handheld X-ray units, practice management software (Dentrix Ascend), and paperless charts. The real estate is also for sale. DALLAS/FORT
WORTH (ID #551): Premier cosmetic dentistry practice located in the heart of the Dallas-Fort Worth metro area. The practice realized annual revenue of $2M+ and strong net cash flow of under 7 figures in 2021 and is on pace to grow significantly in 2022. The office is located in an attractive, free-standing building featuring 5 operatories and the real estate is available for purchase. EAST TEXAS (ID #486): Located in a growing east Texas community, this general practice caters to a dedicated multigenerational active patient base. The well-
644 Texas Dental Journal | Vol 139 | No. 10
appointed 2,500 sq ft space contains 5 fully equipped operatories, digital pano, plumbed nitrous, and computers throughout.
EAST TEXAS (ID #542): Large practice and real estate in east Texas with over 7 figures in revenue. The recently updated 2,400 sq ft facility features 5 fully equipped operatories with digital radiography, paperless charts, CBCT, digital Pano, and an iTero digital scanner. The practice serves a large FFS/PPO, multi-generational patient base with over 3,000 active patients and a stellar online reputation. The seller is open to providing a long-term transition period to the buyer. NORTHEAST TEXAS (ID #554): 100% FFS general dentistry practice in a desirable town in northeast Texas with 7 figures in revenue and strong net income. The turn-key practice features 4 fully equipped operatories with digital radiography, intra oral cameras, paperless charts, CBCT, and a digital scanner.
HOUSTON-NORTHEAST (ID #488): FFS/PPO practice and real estate, growing suburb 45 minutes NE of Houston. 1,800 total patients, steady flow of new patients, solid hygiene recall, and consistent revenue of high-6 figures per year. The office contains 6 fully equipped operatories, plumbed nitrous, digital X-rays, CBCT, and computers throughout. HOUSTONNORTH (ID #553): Large, extremely profitable practice and real estate in north Houston
(Spring/Woodlands). The 5,600 sq ft standalone building contains 10 fully equipped operatories, computers throughout, digital technology, and room for future expansion. The massive active patient base is comprised of Capitation (40%), PPO (35%), Medicaid (15%), and FFS (10%) with 175+ new patients visiting the office per month. The owner is open to exploring a sale to a DSO, multi-location owner, or a well-qualified private practitioner. The 10,000+ sq ft property is also available for sale which offers additional rental income and the possibility for future
McLerran & Associates is the largest dental practice brokerage firm in Texas. When it’s time to buy or sell a practice, we’ve got you covered.
PRACTICE SALES
Austin
PRACTICE APPRAISALS
www.tda.org | October 2022 645
www.dentaltransitions.com
DSO C S
Email: texas@dentaltransitions.com
512-900-7989 DFW 214-960-4451 Houston 281-362-1707 San Antonio 210-737-0100 South Texas 361-221-1990
ADVERTISING BRIEFS
development. SAN ANTONIO, ORTHODONTIC (ID #547): Rare opportunity to purchase a primarily FFS orthodontic practice in north central San Antonio. The facility has a modern feel and is equipped with a 3-chair open bay, 2 additional private treatment rooms, and digital radiography. In 2021, revenue was high-6 figures with strong net cash flow. The practice has been a staple in the community with over 40 years at its present location and is located near several highly desirable neighborhoods. SAN ANTONIO (ID #550): Established general dentistry practice and real estate in northeast San Antonio. The approximately 3,600 sq ft office is located in a free-standing building and is equipped with 7 operatories, digital radiography, intra oral cameras, and computers in operatories. The practice has a strong hygiene recall program, over 2,700 active patients, and provides tremendous upside potential. SAN ANTONIO (ID #557): Majority fee-for-service general dentistry practice in northwest San Antonio. The practice is situated in a high visibility retail center near a bustling intersection and features 4 fully equipped operatories with computers in all ops, a digital scanner, digital radiography, a digital Pano, and intraoral cameras. The office has a solid active patient count, a fantastic online reputation, and annual revenue of mid-6 figures year over
year. TO REQUEST MORE INFORMATION
ON MCLERRAN & ASSOCIATES’ LISTINGS:
Please register at www.dentaltransitions. com or contact us at 512-900-7989 or info@ dentaltransitions.com.
AUSTIN: 32-year-old female-led private practice in a 7-year-old facility in central Austin. Collections in 7 figures over the last 3 years. 85% fee-for-service and 15% PPO production. Primarily a restorative practice. Strong Invisalign program with all implants, ortho, endo, and oral surgery referred out. Great opportunity to buy a healthy practice to grow. Please email Practice Transitions Group for more information, info@ practicetransitionsgroup.com
BEAUMONT: GENERAL (REFERENCE
“BEAUMONT“). Small town practice near a main thoroughfare. 80 miles east of Houston. Collections in 7 figures. Country living, close enough to Houston for small commute. Practice in a stand-alone building built in 1970. The office is 1,675 sq ft with 4 total operatories, 2 operatories for hygiene and 2 operatories for dentistry. Contains, reception area, dentist office, sterilization area, lab area. Majority of patients are 30 to 65 years old. Practice has operated at this location for
646 Texas Dental Journal | Vol 139 | No. 10
ADVERTISING BRIEFS
over 38 years. Practice sees patients about 16 days a month. Collection ratio of 100%. The Practice is a fee-for-service practice. Building is owned by dentist and is available for sale. Contact Christopher Dunn at 800-930-8017 or Christopher@DDRDental.com. HOUSTON (SHARPSTOWN AREA): GENERAL (REFERENCE “SHARPSTOWN GENERAL“). MOTIVATED SELLER. Well established general dentist with high6 figure gross production. Comprehensive general dentistry in the southwest Houston area focused on children (Medicaid). Very, very high profitability. 1,300 sq ft, 4 operatories in single building. 95% collection ratio. Over 1,200 active patients. 20% Medicaid, 45% PPO, and 35% fee-for-service. 30% of patients younger than 30. Office open 6 days a week and accepts Medicaid. Contact Christopher Dunn at 800-930-8017 or Christopher@ DDRDental.com. HOUSTON (BAYTOWN AREA): GENERAL (REFERENCE “BAYTOWN GENERAL“). MOTIVATED SELLER. Well established general practice with mid-6 figure gross production. Comprehensive general dentistry in Baytown on the east side of Houston. Great opportunity for growth! 1,400 sq ft, 4 operatories in single story building. 100% collection ratio. 100% fee for service. Practice focuses on restorative, cosmetic and implant dental procedures. Office open 3 - 1/2 days a week. Practice area
is owned by dentist and is available for sale. Contact Christopher Dunn at 800-930-8017 or Christopher@DDRDental.com.
HOUSTON, COLLEGE STATION, AND LUFKIN (DDR DENTAL Listings). (See also AUSTIN for other DDR Dental listings and visit www. DDRDental.com for full details. LUFKIN— GENERAL practice on a high visibility outer loop highway near mall, hospital and mature neighborhoods. Located within a beautiful single-story, free-standing building, built in 1996 and is ALSO available for purchase. Natural light from large windows within 2,300 sq ft with 4 operatories (2 hygiene and 2 dental). Includes a reception area, dentist office, a sterilization area, lab area, and break room. All operatories fully equipped. Does not have a pano but does have digital X-ray. Production is 50% FFS and 50% PPO (no Medicaid), with collection ratio above 95%. Providing general dental and cosmetic procedures, producing mid-6 figure gross collections. Contact Christopher Dunn at 800930-8017 or Christopher@DDRDental.com and reference “Lufkin General or TX#540“.
HOUSTON—GENERAL (SHARPSTOWN). Well established general dentist with high-6 figure gross production. Comprehensive general dentistry in the southwest Houston area
www.tda.org | October 2022 647
ADVERTISING BRIEFS
focused on children (Medicaid). Very, very high profitability. 1,300 sq ft, 4 operatories in single building. 95% collection ratio. Over 1,200 active patients. 20% Medicaid, 45% PPO, and 35% fee-for-service. 30% of patients younger than 30. Office open 6 days a week and accepts Medicaid. Contact Chrissy Dunn at 800-9308017 or chrissy@ddrdental.com and reference “Sharpstown General or TX#548“. HOUSTON —GENERAL (PEARLAND AREA). GENERAL
Located in southeast Houston near Beltway 8. It is in a freestanding building. Dentist has ownership in the building and would like to sell the ownership in the building with the practice. One office currently in use by seller. 60% of patients age 31 to 80 and 20% 80 and above. Four operatories in use, plumbed for 5 operatories. Digital pano and digital X-ray. Contact Christopher Dunn at 800-930-8017 or christopher@ddrdental.com and reference “Pearland General or TX#538“. HOUSTON— PEDIATRIC (NORTH HOUSTON). This practice is located in a highly sought-after upscale neighborhood. It is on a major thoroughfare with high visibility in a strip shopping center. The practice has 3 operatories for hygiene and 2 for dentistry. Nitrous is plumbed for all operatories. The practice has digital X-rays and is fully computerized. The practice was completely renovated in 2018. The practice
is only open three and a half days per week. Contact Christopher Dunn at 800-930-8017 or christopher@ddrdental.com and reference “North Houston or TX#562“. WEST HOUSTON
—MOTIVATED SELLER. Medicaid practice with production over 6 figures. Three operatories in 1,200 sq ft in a strip shopping center.
Equipment is within 10 years of age. Has a pano and digital X-ray. Great location. If interested contact chrissy@ddrdental.com. Reference “West Houston General or TX#559“.
SAN ANGELO: To those desiring the perfect balance between work and play: Are you interested in taking over a successful readymade practice with a great salary low-to-mid 6 figures? Located in west central Texas, San Angelo is a city of 100,000+ but offers a small town feel and excellent quality of life. The city was named the Visual Arts Capital of Texas in 2021 and is alive with a vibrant mixture of arts and culture for children and adults. It is consistently ranked as one of the best small cities for business and employment. San Angelo is home to award winning Angelo State University, three lakes, the beautiful Concho Riverwalk, an incredible nationally ranked Art Museum, and one of the best preserved forts in the nation, Fort Concho—all with numerous kid-involved programs. As a Texas friendly
648 Texas Dental Journal | Vol 139 | No.10
ADVERTISING BRIEFS
city, live music is offered almost daily at one of many venues and one-of-a-kind restaurants in town. The community is diverse, with an active young professional group, outstanding medical facilities, ranked sports teams, great hunting and fishing, and a low cost of living. Easy traffic takes you anywhere in the city within 10 minutes. It’s a great place to raise a family and a great place to live, work, and play. The 2,400 sq ft newly remodeled dental office, built to accommodate two dentists, is a free-standing building with natural light in each operatory. An extremely healthy hygiene program is in place with 2 hygienists. There are 6 operatory rooms—four equipped. The majority of practice is FFS cash, with over 3,000 active patients. The practice has an excellent reputation in the local community. A bonus package is included for preferred equipment needs. Contact Geremy Haseloff @ 806-7774732 or geremy.haseloff@henryschein.com.
SAN MARCOS: Small dental office for sale. San Marcos, approximately 1,000 sq ft. Great location. 2 Operatories. Fully equipped and functional. Office only, no practice transfers. Recently retired. Email for info and photos. stevenmaycockdds@gmail.com.
WATSON BROWN PRACTICES FOR SALE:
Practices for sale in Texas and surrounding states, For more information and current listings please visit our website at www. adstexas.com or call us at 469-222-3200 to speak with Frank or Jeremy.
INTERIM SERVICES
HAVE MIRROR AND EXPLORER, WILL
TRAVEL: Sick leave, maternity leave, vacation, or death, I will cover your general or pediatric practice. Call Robert Zoch, DDS, MAGD, at 512517-2826 or drzoch@yahoo.com.
www.tda.org | October 2022 649
650 Texas Dental Journal | Vol 139 | No. 10 PRN Helpline (800) 727-5152 Visit us online www.txprn.com YOUR PATIENTS TRUST YOU. WHO CAN YOU TRUST? If you or a dental colleague are experiencing impairment due to substance use or mental illness, The Professional Recovery Network is here to provide support and an opportunity for confidential recovery. Anesthesia Education & Safety Foundation, Inc.....579 Choice Transitions ............................. Inside Back Cover Dental Expert Witness Training.................................636 JKJ Pathology ................................................................637 Keyway .........................................................................636 Law Offices of Mark J. Hanna ....................................632 McLerran & Associates...............................................645 Penumbra Diagnostics ...............................................583 Professional Recovery Network ................................650 TDA Perks ........................................... Inside Front Cover University of Texas School of Dentistry of Houston583 Watson Brown .............................................................633 ADVERTISERS