As the Cancer Center Celebrates 50 Years, a Longtime Survivor Tells His Story
“You’ve only got one life to live,” says the UR alumnus. “Make it count.”


Inside:
• Wilmot's World-Class Lymphoma Program
• Meet the New CEO at URMC
University of Rochester Medical Center 2024 Volume 1
Wilmot Cancer Institute
Letter from the Director
 Jonathan W. Friedberg, M.D., M.M.Sc. Director, Wilmot Cancer Institute
Jonathan W. Friedberg, M.D., M.M.Sc. Director, Wilmot Cancer Institute
Editor / Writer
Leslie Orr Leslie_Orr@urmc. rochester.edu
Contributors
Barbara Balcaen, Tyler Bowers, Sandra Parker
Graphic Design
Beth Carr, Kent Joshpe
Feature Photography
Erich Camping, Ben Lipowitz, Jeff Witherow, Matt Wittmeyer
The Wilmot Cancer Institute is a component of Strong Memorial Hospital.
Hello friends of the Wilmot Cancer Institute,
Our teams at Wilmot spend their days in an intense routine of caring for patients, investigating cancer in research labs, educating the next generation, maintaining our clinical trials operation, and planning for the future. Sometimes it is worthwhile to pause for a minute. This year marks the 50th anniversary of the founding of this cancer center on the University of Rochester campus, and we have much to celebrate.
Progress made since those days in the 1970s is almost unimaginable—from astonishing technological advances and life-saving drug discoveries to new ways in which we relate to each other in the workplace. Evolving from a single small footprint as an extension of Strong Memorial Hospital, our current Wilmot building houses almost 100 inpatients, comprehensive medical and radiation oncology outpatient care, and translational bench research. Remarkably, this represents only one of 13 care locations in our expanding catchment area.
I recently wrote an article entitled "An Oncology Renaissance" in which I reflect about the exciting and breathtaking landscape in cancer care and research. I have realized that in my own clinic caring for patients with lymphomas, every week I see patients living and thriving who would not have survived had they been diagnosed only a decade ago. Celebrating our wins and the promise of an even bolder future is so important amid daily work, and only increases the sense of urgency at Wilmot for continued improvement.
In this edition, you will read stories of advances, inspiration, and teamwork that result in offering our best care to patients. Incredible community support during the past 50 years makes these achievements possible. As we look forward to the next 50 years, I hope you share my optimism for Wilmot, our entire field, and most importantly for our patients.
My best to everyone and thank you, as always, for your steadfast support.
 Jonathan Friedberg, MD, MMSc Director, Wilmot Cancer Institute
Jonathan Friedberg, MD, MMSc Director, Wilmot Cancer Institute
On the Cover John Saunders, 66, of Gurnee, IL, is a cancer survivor of 48 years. He was treated for Hodgkin lymphoma as a freshman at University of Rochester. Photo by Ben Lipowitz
In this issue Reflections of a Longtime Cancer Survivor.........................................................2 Learn Why Wilmot’s Lymphoma Program is One of the Best..................................4 Patients and Families Impact Cancer Research...................................................9 Wilmot’s 50th Anniversary in 2024.................................................................10 The
has Deep Ties to Wilmot...................................12 News Briefs................................................................................................14 Wilmot Warrior Weekend and Community News................................................16 2023 Volume 2
New URMC Chief Executive
About Wilmot Cancer Institute
UR Medicine's Wilmot Cancer Institute is the largest cancer-care provider in the state outside of New York City. Its goal is to prevent and conquer cancer through innovation in science, patient care, education, and community outreach.
Based in Rochester, N.Y., as part of the University of Rochester Medical Center system, Wilmot serves approximately 3 million people in a 27-county region in western and central New York. Wilmot features an 87-bed flagship cancer hospital, 13 locations, and one of the state’s largest Blood & Marrow Transplant (BMT) programs. Wilmot is a component of Strong Memorial Hospital and home to the area’s first cancer survivorship clinic, one of the nation’s first specialized geriatric oncology clinics, and an integrative oncology center free to all patients.
Established in 1974, Wilmot has a long history of outstanding clinical and research breakthroughs—including pivotal contributions to the pioneering HPV cancer vaccine, and the study of cancer-related nausea and the role of anti-nausea drugs.
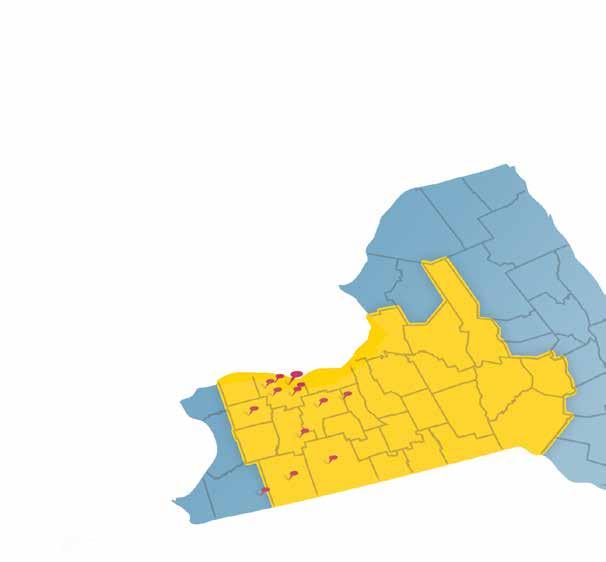
13 locations
27 counties
3M people

7,135 new cancer cases in 2022 Employs over 500 oncology nurses Employs over 195 oncology physicians
Trains over 351 future oncologists & researchers Employs over 100 researchers $30M in annual direct funding Offers nearly 200 clinical trials
Wilmot is proud to be part of the NCI National Clinical Trials Network, and to serve as a hub for the NCI Community Oncology Research Program.
WILMOT CANCER INSTITUTE 1

Make Life Count
It was college spring break week at the University of Rochester in 1976. John Saunders, 18 at the time and a first-year student, had just started dating a girl a few days earlier—but there would be no fun outings, no hanging out.
“I remember thinking: Hey! What are you doing for spring break? I’m having a splenectomy,” jokes Saunders, who is now 66. He had just learned from UR physicians that he was sick and needed surgery to remove his spleen as treatment for Hodgkin lymphoma, a type of cancer that afflicts young adults.
Cancer is not a typical concern of college students. They are busy figuring out campus life, meeting new friends, keeping up with studies. In 1976, swirling through colleges across the nation was an election that sent Jimmy Carter to the White House, and big news that two guys named Steve Jobs and Steve Wozniak had invented a computer and established a company called Apple in the garage of Jobs’ parent’s home. America was celebrating its bicentennial, and the #1 Billboard hit was “Silly Love Songs” by Paul McCartney and Wings.
The 1970s was also a time when only about half of all people
diagnosed with cancer would survive at least five years, although it was the start of a pivotal era for progress against the disease.
In 1971, President Richard Nixon signed the National Cancer Act and created a national infrastructure for world-class cancer research. At the UR, a group of clinicians, scientists, and academics had joined forces to officially establish a cancer center on campus, funded by a grant in 1975 from the National Cancer Institute. One of the leaders of that effort was the renowned and pioneering radiation oncologist Philip Rubin, MD, who ended up becoming Saunders’ doctor. (Rubin died in 2014.)
Saunders recalls sensing that Rubin was a big deal in his field, and he trusted him.
“I remember that he was reassuring. He said there had been a lot of advances in cancer treatment recently,” Saunders says. “And
find us on Facebook, LinkedIn, Twitter,
Instagram
and
2
I also remember that he said: Don’t go to the library and read about this, because they’ll say you’re going to die. And that’s not true.”
Taking that advice, Saunders shoved aside doubts—and focused on moving ahead.
Carrying On, Through Adversity
Saunders had first noticed something was wrong weeks earlier, following the Christmas holiday break. He found a lump under his left arm while putting on deodorant in his Susan B. Anthony Hall dorm room. He figured he had mononucleosis, a virus that’s fairly common among college kids. At the health center, doctors seemed concerned and ordered tests.
On Friday, Feb. 13th (the irony of that unlucky day was not lost on Saunders and his friends), he had diagnostic surgery to remove the lump and nearby lymph nodes. As it turned out, Saunders and his parents got the best news possible: the cancer was very early, stage 1A. With a cure in mind, doctors prescribed aggressive treatment. Surgeons performed the spring-break splenectomy, and then from April to July Saunders underwent daily radiation therapy to his entire torso from chest to belly button, and the left arm.
Side effects of treatment were minimal at first, although he did develop an esophagus burn and was on a liquid diet for a while. As a young guy who liked to eat, “that was really hard,” Saunders recalls.
What did he feel, emotionally, when all of this was happening?
“The story is intertwined with my Christian faith,” Saunders says. “I believed that I had things to do in life, and I hadn’t done them yet. So, it’s up to God to get me out of this alive. In some ways, I had an amazing amount of peace—but I also wasn’t looking forward to cancer treatment, right?”
Doctors advised him that many people leave college during treatment. “But I chose Option B,” Saunders says. “I wanted to carry on with my life.”
Throughout the ordeal, he lived fully. He took a regular course load as a physics/math major. His sister was married that winter, and Saunders attended the wedding. That summer, he stayed in Rochester and moved off campus, renting a South Wedge house with a buddy. He played piano and got a job at the Eastman School of Music in the instrument repair department, riding a bike to and from work, hoping that exercise would rev up his immune system and fight the cancer.
And he and that nice young woman that he met days before his diagnosis settled into a long relationship. They graduated together in 1979, got married in 1980, and she went on to earn an MBA from the Simon School of Business and a master’s degree in public health from the UR School of Medicine and Dentistry. Mary Ellen Saunders has been by his side ever since.
“At the end of that first spring break, she told me: ‘We’ll get through this.’ She’s a very strong woman,” Saunders says, “and has the ability to deal with tough situations.”
In June, John and Mary Ellen Saunders will have been married 44 years. They have been living in the Chicago area for decades and raised four children. In 2023, they welcomed their first grandbaby, Lila Rose.
Retired and Grateful
Saunders has been cancer-free since 1976.
But like many cancer survivors from that era, he suffered from what oncologists call the “late effects” of treatment. These can include cardiovascular problems, lung damage, and second cancers. Thankfully, Saunders has not faced the latter, but he has been through other health challenges.
About 20 years ago, Saunders was diagnosed with a thyroid disorder that his cancer-care team had warned him was a possibility. Then, 10 years ago, he developed radiation-associated retinopathy and distorted vision in his left eye. Eight years ago, he developed heart murmurs and aortic stenosis—again, from the earlier radiation treatment to his chest. Doctors monitored it closely until the condition progressed from mild to severe.
In January of 2022, Saunders had open-heart surgery at Northwestern University. It was scary, he says, and it took weeks of medication adjustments and cardiac rehabilitation for him to regain his footing. Eventually he was back to normal life and his exercise routine.
Louis (Sandy) Constine, MD, a professor of Radiation Oncology at the UR and Wilmot Cancer Institute, who has led several international research projects on the late effects of treatment, says Saunders’ case is not unusual—he calls it the “agony of victory”—but the future is much brighter for people being treated today. (See story on page 8.)
Modern radiation therapy machinery is “light years” better, Constine says. “With sophistication and elegance, we can do a much better job at targeting areas of the body that harbor lymphoma cells… We can use different angles and exclude much of the chest and heart. That’s a tremendous change in terms of the risk to the body.”
Recently, researchers discovered another, new treatment strategy—skipping radiation altogether, and using chemotherapy and immunotherapy to treat young people with HL. A landmark study led by Wilmot Director Jonathan Friedberg, MD, MMSc, cured more than 90% of patients with this new regimen. If Saunders were diagnosed in 2024, he would not get a splenectomy and would not likely receive radiation, Friedberg says. (See related story, page 4.)
Doctors did what they knew best at the time, and Saunders remains grateful. “It’s 48 years later and I’m alive,” he says. “That’s awesome!”
He retired from a lengthy career in information technology, first at Abbott Laboratories, then at AbbVie, the pharmaceutical company, where he appreciated being part of medical science. Now, he takes part in treasured family gatherings, Christian ministries, and a civic organization with a goal of reducing political polarization.
“You’ve only got one life to live,” Saunders says. “Make it count.”
3 WILMOT CANCER INSTITUTE

Lymphoma is a complex blood cancer with 60 different subtypes. Most cases fall into two major classifications: Hodgkin or non-Hodgkin lymphoma. The disease is rooted in the immune system, including lymph nodes, spleen, and bone marrow. Normally, healthy lymphatic tissue fights germs and infections. If cancer develops in the lymph system, it can spread throughout the body. The cause is not fully understood.
When
it Comes to “Curing” Cancer, Lymphoma Has Served as a Teacher and Leader
Lymphoma is not as common as breast or prostate cancer. Screening is not routinely available to detect it, like with colorectal cancer. And, unlike lung cancer, it is not linked to a modifiable habit such as smoking.
But one thing sets lymphoma apart from other cancers: It is relatively easy to study and therefore investigators who focus on lymphoma have been leaders in the effort to cure many types of cancer, says Jonathan Friedberg, MD, MMSc, a worldwide lymphoma expert and director of the Wilmot Cancer Institute.
“Lymphoma has been a teacher,” he says.
Why? Lymphoma cells are more accessible, via a simple blood draw, versus solid tumors that require surgery to get a sample. This allows investigators to easily obtain millions of lymphoma cells for research. Lymphoma was also the first cancer for which scientists conducted gene-expression profiling, which advanced the field for all; that initial gene-profiling paper from the year 2000 has more than 7,200 citations, one of the most highly cited research papers ever.
4 find us on Facebook, LinkedIn, Twitter, and Instagram
Wilmot's Lymphoma Team: Paul Barr, MD; Danielle Wallace, MD; Clive Zent, MD; Carla Casulo, MD; Jonathan Friedberg, MD, MMSc; Jamie Flerlage, MD, MS; Patrick Reagan, MD

“Blood cancer cells have also been more responsive to chemotherapy and radiation, which means we’ve been able to cure fractions of patients with blood cancers for more than 60 years,” Friedberg says.
He notes additional “firsts” that place lymphoma in a unique category: It was the first cancer to have an approved monoclonal antibody treatment, modern drugs that enlist the immune system to fight cancer. Hodgkin lymphoma was the first cancer for which the word “cure” was used, when survival rates reached 90%. And lymphoma was the first disease for which oncologists used CAR T-cell therapy. This is another state-of-the-art immunotherapy—one that involves taking a patient’s own immune cells out of the body, engineering them to attack cancer, and infusing them back into the patient.
“Survivorship is another area where lymphoma has been a teacher,” Friedberg adds. “We have patients who have survived for 40 or 50 years, and that allows us to better understand the treatment effects later in life.” (See related story on page 2.)
This golden era—where cancer deaths are falling and a confluence of events is driving innovation every day—is a “breathtaking” time in oncology, says Friedberg.
“In my own clinic caring for patients with lymphomas, every week I see people living and thriving who would not have survived had they been diagnosed a decade ago,” he says.
More about Wilmot Director and lymphoma program leader Jonathan Friedberg:
He grew up in a suburb of Milwaukee and is a huge Green Bay Packers fan. His father, a pediatric cardiologist, was intrigued with farming and bought 40 acres outside of the city, where they raised chickens and had a small beef cattle operation. Friedberg bailed hay in the summer heat and showed animals at 4-H fairs. “It was really hard work,” he says. “I have tremendous respect for people who farm.”
As a child, he also accompanied his father to work at the hospital, which fed his desire to go into medicine. During undergraduate years at Williams College, Friedberg enjoyed political science and remains interested in politics; people joke that this prepared him for the cancer center directorship. He attended Harvard Medical School and did advanced training in Boston at Massachusetts General Hospital and Dana-Farber Cancer Center. His thoughts on leadership? “Listen and incorporate information from a lot of sources. Be flexible and appreciate that your opinion can change, but ultimately be able to make decisions and not be paralyzed. You don’t want perfection to be the enemy of good. You must at some point make decisions and move on.”
“I’ve learned the importance of choosing good teammates and spending perhaps a disproportionate amount of time and thought into recruiting those individuals. You don’t want them all to be your friends. You need to have a team of rivals, I guess, like Abraham Lincoln did. But at the same time, you want to make sure you have respect for them, and they have respect for you, and that you can give them clear authority to make decisions themselves and make the whole organization better.”

5
WILMOT CANCER INSTITUTE *Contributor: American Society of Clinical Oncology
Teamwork Brings Progress
Wilmot has a rich history, and a large team, contributing to the lymphoma
Leadership in clinical trials. Keeping up with the fast pace of new therapies, Wilmot oncologists often enroll more patients than other cancer centers into clinical studies through the National Clinical Trials Network (NCTN). Paul Barr, MD, has been at the forefront of several large clinical trials testing another modern treatment—drugs in a class known as BTK inhibitors—transforming treatment of non-Hodgkin lymphoma. “We no longer use chemotherapy because of this new class of drugs,” Barr says. Hundreds of Wilmot patients have benefited from a BTK inhibitor (in pill form) through clinical trials and now in standard care.
Personalized medicine. It can be tricky to predict whether certain types of lymphoma will return after treatment. In collaboration with Wilmot’s dedicated lymphoma pathologists and other scientists, Carla Casulo, MD, has been studying an aggressive form of follicular lymphoma to discover what makes some patients’ cancer biologically different and how to care for this early-relapse group. She and Friedberg identified the characteristics of a high-risk subset of patients, and now they are collaborating with Barr, who is leading a national clinical trial to evaluate two novel therapies for these individuals. Study results are expected in 2024.
Novel immunotherapy. Wilmot was one of the first centers in the country to offer CAR T-cell therapy for lymphoma, led by Patrick Reagan, MD. This new category of treatment involves engineering a patient's own immune cells to seek and destroy cancer. Since the early days of discovery, several CAR T-cell therapies have been approved for blood cancers, and research is ongoing to refine the therapy and expand it to more types of cancer.
Nurse Navigation Some patients come in the door very sick and need a multitude of diagnostic actions. Anna Morrison, RN, OCN, has built a navigation program at Wilmot that quickly pairs each patient with the correct specialist. The goal is to make sure all imaging scans and other tests are readily available to oncologists, to give them a full picture of each person’s disease before meeting with the patient.

success
story
Advances for children and young adults. With a focus on pediatric Hodgkin lymphoma, Jamie Flerlage, MD, recently joined Wilmot and brought clinical trials expertise for this vulnerable group of patients. She runs a national pediatric Hodgkin research consortium and is working on pinpointing genetic variants that lead to blood cancers. Wilmot also has two exceptional young-adult cancer survivors as facul-ty— Lauren Ghazal, PhD, and AnnaLynn Williams, PhD—who conduct award-winning survivorship research and add a fresh perspective to the team.
Wilmot’s multidisciplinary, specialized team of physician-scientists, nurses, pathologists, clinical trials experts, and researchers have ambitious plans to make the elusive “cure” more common.
“Clinical trials can offer the chance to have less-toxic therapy, or to cure the cancer with less-aggressive amounts of treatment,” Flerlage says. “It’s a premise of ‘curing better’ “
Practice-Changing Study
As chair of the lymphoma committee for an international research network known as SWOG, Friedberg recently led a study that will change treatment for many young patients with advanced Hodgkin lymphoma. (See related story to the right.)
The results were outstanding: About 86% of the people in the standard treatment group achieved remission. In the group of individuals who received an experimental cocktail of drugs, 94% went into remission and remained there after one year The outcome, Friedberg says, "exceeded ourexpectations"
Several factors made it a landmark study:
• It was the first time in the modern era that a clinical trial included both adolescents and adults with advanced Hodgkin lymphoma. Often, these groups are treated and studied separately.
• A key part of the trial design was to enroll pediatric patients ages 12 and older. The standard treatment for children and teens has often been radiation therapy, which carries risks of serious side effects later in life, such as second cancers, thyroid dysfunction, and heart disease. By eliminating radiation for children enrolled in this trial, investigators reduced the risks of toxic, late side effects.
• Nearly 1,000 individuals took part in the study at more than 200 institutions in North America. The number of Black and Latino patients aligned with the general population, which was a goal of researchers. (Wilmot recruited the second-highest number of people with Hodgkin lymphoma to the trial, led locally by Casulo.)
Because of the impact of Friedberg's study, in 2023 the American Society of Clinical Oncology (ASCO) showcased the research at a plenary session at its annual meeting, the largest gathering of oncologists in the world. This year, Friedberg and co-investigators expect to publish the results in a high-impact medical journal.
6 find us on Facebook, LinkedIn, Twitter, and Instagram
Anna Morrison, RN, OCN
Luck and Science for a Nurse-Turned-Patient
Hannah Lundgren knows the value of Wilmot’s prominent lymphoma program and clinical trials.
In 2020, at age 27, she was working long hours as a nurse and felt exhausted, had lost weight, and found a swollen lymph node in her neck. After months of feeling ill but not getting clear answers, her physicians sent her to Wilmot, where she was diagnosed with stage 4 Hodgkin lymphoma (HL).
Jonathan Friedberg took over her care, and, as luck would have it, he was enrolling patients in what would turn out to be an historic and groundbreaking clinical trial for advanced HL, a rare cancer that afflicts mostly young adults.
The randomized, phase 3 study compared the standard treatment, chemotherapy plus brentuximab vedotin (brand name: Adcetris), against a new drug combo that included an immunotherapy, nivolumab (brand name: Opdivo), plus chemotherapy.
Lundgren enrolled and, as luck would have it, again, study coordinators randomly assigned her to receive the experimental immunotherapy in addition to chemo. (Oncologists were blind to patients’ placements in this trial.)
After her first treatment, the fatigue suddenly vanished. “It was crazy,” she says. “And I also didn’t have any more palpable lymph nodes.”
She continued infusions for six months and was cancer-free by December 2021.


Still in good health, Lundgren is taking on life with zeal: She ran a half-marathon, got married to Ryan Tolpa, and enrolled in a nurse-practitioner program while switching her career focus from orthopedics to oncology. She now cares for gastrointestinal cancer patients at Wilmot.
7 WILMOT CANCER INSTITUTE
Better days ahead
When Friedberg was a little older than Lundgren and launching his oncology career, he arrived on the ground floor of a decades-long positive trajectory for treating lymphoma. He had just become faculty at the Dana-Farber Cancer Institute in Boston when the U.S. Food and Drug Administration approved a drug called rituximab—creating a major pivot point for the disease, he says. “It was the start of a new era,” Friedberg says. “I joined the field at this amazing time.”
Doctors initially used rituximab, an early type of monoclonal antibody, to treat b-cell lymphoma but today the targeted therapy, sometimes in combination with other drugs, can attack and manage nonHodgkin lymphoma, follicular lymphoma, chronic lymphocytic
The “Agony
leukemia, as well as other blood diseases. And following rituximab, a whole new list of treatments has emerged for various blood cancers and to use in combination with older drugs.
The progress, which keeps coming, allows doctors to focus on survivorship: The five-year survival rates for lymphomas, taken as a group, range from about 75% to about 95%, depending on the subtype and stage of disease.
Even better days lie ahead, Friedberg believes. When surveying the lymphoma landscape, he likes to quote the lyrics of a favorite artist, Bruce Springsteen—“Meet me in the land of hopes and dreams.”
of Victory” No Longer Brings as Much Anguish

Louis (Sandy) Constine, MD, has been a specialist in radiation and pediatric oncology for 50 years. It is fitting to salute his work the same year that Wilmot Cancer Institute is celebrating its 50th anniversary, as Constine has been prominent and influential, guiding much progress in the field.
When he first started, doctors used radiation therapy and chemotherapy for nearly everyone with lymphoma. The treatments exposed children and young adults to toxicities and side effects that included second cancers and heart disease later in life. Young girls treated with radiation, for example, had a 30% chance of developing breast cancer. Overall, research shows, 60% to 90% of childhood cancer survivors treated in previous eras are likely to develop chronic health conditions.
Constine adopted the phrase “the agony of victory” to illustrate the double-edged sword of cancer treatment: yes, children and young adults may be cured of their cancer or go into remission for many years, but they will face serious health threats in the future.
To change this situation, researchers conducted collaborative, long-term studies to follow young patients as they aged. Because of this research—plus major improvements in technology—the outlook is vastly different for children and young adults treated today.
“Now we can celebrate our victories with less agony because the long-term side effects of treatment have diminished,” he says. “That’s a blessing to us all.”
Constine, the Philip Rubin Professor of Radiation Oncology and Pediatrics at the University of Rochester, has been at the forefront of this Herculean effort and the resulting improvements. Years ago, he established an international network of more than 150 physicianscientists, biostatisticians, physicists, and epidemiologists committed to investigating the toxic effects of cancer treatment for children and adolescents. This summer, the premier resource in radiation oncology, the International Journal of Radiation Oncology, Biology, Physics will spotlight the group’s 28 reports—a seminal contribution to the field—with Constine as the lead editor and frequent author.
One factor that makes the research so important, Constine says, is that the team looked at how cancer treatment impacts
the organs of children as a function of the stage of their development and the impact of chemotherapy. Scientists also established radiation dose and exposed volume data to inform planning and to reduce bad outcomes, identified knowledge gaps, and offered blueprints for future studies to stimulate young researchers.
The data will guide safer treatment planning for children with cancer around the world for decades, Constine says.
The series of reports is a fulfilling chapter, he says, in a career that began at Stanford University with notable mentors including Henry Kaplan, MD, a pioneer in lymphoma radiation oncology; Saul Rosenberg, MD, a pioneer in treating Hodgkin lymphoma; and Sarah Donaldson, MD, a central force in pediatric radiation oncology. He moved to Rochester to work with another major contributor, Philip Rubin, MD, who taught Constine to strive to ease the journey for all afflicted by cancer.
Constine advanced to lead many professional societies and physician research networks and was awarded fellowships in both the American College of Radiology and the American Society of Radiation Oncology.
His professional life, he says, is guided by these words: “For the survivor of cancer, the world is full, and each day is a celebration—for the physician, each patient is an inspiration; for the person fighting cancer, each day is precious and must be faced with courage.”
find us on Facebook, LinkedIn, Twitter, and Instagram
8
COE Community Outreach and Engagement improves the health of local and regional residents through partnerships. Research Action Councils (RACs), are one example of how community voices are impacting research at Wilmot Cancer Institute.
In Cancer Research, the Role of the Lay Person is Growing and Adds Value
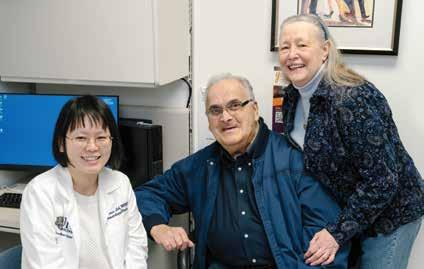
As the wife and caregiver of an 82-year-old man with leukemia, Karen Savino decided to join a group that would allow her to contribute to cancer research. She is 76 and a certified dyslexia therapist. Technically, she has no educational background focused on cancer, but because of her husband’s multiple diagnoses—first with lymphoma and then with leukemia—she has become quite knowledgeable on the front line.
A year ago, she became a member of a Research Action Council (RAC) for blood cancers at Wilmot Cancer Institute. RACs are organized by Wilmot’s Community Outreach and Engagement (COE) office, as a formal way for lay people to provide bidirectional communication to investigators about their research projects. RACs help physicians and scientists wade through problems, rethink questions, and provide a fresh and unique perspective to improve grant submissions or inform clinical and basic research directions.
“It’s been very interesting,” Savino says.
She and her fellow RAC members have been working with Kah Poh (Melissa) Loh, MBBCh BAO, MS, a Wilmot geriatric oncologist who studies the fast-paced and stressful shared decision-making that occurs when a person has leukemia.
With other types of cancer, a patient often has bit of time to make decisions. But acute leukemia usually presents as a crisis that needs immediate treatment. With so many decisions to make and tests to undergo, it can be overwhelming for individuals and their families during the hours and days following a diagnosis. In this setting, Loh says, there is little time to talk through treatment options or a patient’s values and goals for the future. She is an award-winning investigator who is finding ways to do this better, particularly with older adults, to promote a sense of control and peace for patients and improve the way oncologists present information.
The RAC members influence Loh as she mulls details of her projects.
For example, Loh was convinced that in the early days of an acute leukemia diagnosis, a patient would not want to hear about irrelevant topics, such as healthy lifestyle advice on nutrition or exercise. She was concerned that patients and families are emotionally unprepared to suddenly confront leukemia—and in this context, it might be inappropriate and distressing to bring up topics that are outside of what is most urgent.
The RAC members disagreed.
Focusing on nutrition or exercise “is something that we can do on our own; it’s about control,” Savino explains. “And what I can control, I want to do.”
Loh was impressed with this advice from the RAC group— especially since she had polled many oncology colleagues, and they had all agreed with her to leave out less-relevant information. But none of them wore the shoes of a patient.
“I was like, Okay!” Loh recalls. “It’s a good example of something that really reshaped our opinion. After getting reassurance from the RAC members that it was okay to talk about these kinds of topics, I was able to move forward.”
The dilemma in this case arose when Loh was applying for a large grant to evaluate a shared-decision-making intervention for older adults with leukemia. A National Cancer Institute grant reviewer had asked for more details, and that’s when Loh began to wonder what topics would be relevant or irrelevant for oncologists to discuss with their patients.
The RAC, which started with 10 community participants in 2022 and has grown to 12, meets every three months for wide-ranging discussions. Loh says she tries to stay in the background, to listen. The dynamics are getting more comfortable, and patients and caregivers in the group are not afraid to speak up.
“I love working with them,” Loh says.
Savino is satisfied, as well. “I think we’ve definitely had an impact on the ease of information, and how medical information is presented to patients and families.”
“It’s good to feel that you’re contributing and helping because the doctor is helping you,” Savino adds, noting that Loh is her husband Larry’s oncologist. “I’m so glad things have changed over the years in cancer because of better treatments and research.”
WILMOT CANCER INSTITUTE 9
Larry and Karen Savino meet with Dr. Kah Poh (Melissa) Loh at Wilmot.
WILMOT CANCER INSTITUTE'S
50th ANNIVERSARY
Cancer research and treatment is in its most exciting era yet.
A host of molecular discoveries, faster flow of data, modern technology, and intensive collaboration are fueling an oncology renaissance that ignites excitement in research laboratories and results in ever-more options for patients. As a consequence, an estimated 18 million survivors live in the U.S. today—and that number is expected to grow to 26 million by 2040.
But it was not always this way. The word “cancer” had been synonymous with shame, and death. The National Cancer Act of 1971 began to transform the nation’s view of the disease with a $1.6 billion investment into the National Cancer Institute. The Act became a symbol of hope, and shortly thereafter the University of Rochester’s cancer center came into existence in 1974 as part of Strong Memorial Hospital. Four physicians led that effort: Robert Cooper, MD, a surgical pathologist; John Bennett, MD, a hematologist/oncologist; Philip Rubin, MD, a radiation oncologist; and cancer surgeon Brad Patterson, MD.
The UR cancer center has since grown into the Wilmot Cancer Institute, named for local philanthropist James P. Wilmot—becoming the largest provider in the state outside of New York City. Wilmot serves three million regional residents with an 87-bed inpatient cancer hospital, 13 locations, and a robust clinical trials office.
“We do nothing today the way researchers did 50 years ago,” says Hartmut “Hucky” Land, PhD, Wilmot deputy director and cancer scientist who started in the field as an ambitious 25-year-old. “The types of research happening now were impossible to imagine 40 to 50 years ago, when we didn’t even have computers in the lab. I’ve been very privileged to witness—and luckily, I’ve been a little bit of a contributor—to many advances in cancer research.”
Milestones in Cancer
Two of the most important developments in cancer care and prevention have UR roots:
Groundbreaking studies by Gary Morrow, PhD, in the 1980s that defined nausea and vomiting as a major barrier to completion of cancer treatment. This led to anti-nausea drugs and opened the field of cancer control, for which UR has been a national leader for decades.
Pivotal contributions to the human papillomavirus (HPV) cancer vaccine; the UR was awarded patents in 2011 for an essential discovery by UR Medical Center virologists William Bonnez, MD, Richard Reichman, MD, and Robert C. Rose, PhD. In 2006, Gardasil became the first vaccine to protect against HPV-related cervical cancer.
A native of Germany, Hucky Land was on the team in the 1970s that cloned the first gene in that country. It was the dawn of the field of molecular biology, from which today’s cancer treatments have emerged. The UR recruited him in 1999 and Land built a distinguished career, earning awards for studying the fundamental similarities between diverse types of cancer while also taking leadership roles at Wilmot and serving as the Robert and Dorothy Markin Professor and founding Chair


find us on Facebook, LinkedIn, Twitter, and Instagram 10
ANNIVERSARY
Examples of other watershed changes from the past 50 years:
Research. The Cancer Genome Atlas Project and other investigations in the early 2000s confirmed that cancer is not a single disease, but different diseases based on unique tumor characteristics. This yielded the concept of “precision medicine” to target cancer mutations. It prompted new ways to categorize cancer by its molecular abnormalities and not solely by organ site. Clinical studies and tests for genomic profiling followed. Among the largest: In 2015, the NCI launched the MATCH trial to test more than 20 drugs and drug combinations based on molecular analysis of tumors in adults with cancer, followed by a MATCH trial for children in 2017.
Research. In 2020, the Nobel Prize went to scientists for developing a revolutionary tool known as CRISPR to edit the genome. This discovery shifted the landscape again, allowing scientists to alter the genetic code, study cancer cell behaviors, and design new treatments.
Screening. In 1950, scientists first linked cigarette smoking to lung cancer. It wasn’t until 2010 that the first lung cancer screening trial took place. Other screening studies for other types of cancer (such as colorectal), have continued to show that screening saves lives and allows for earlier diagnosis and treatment. Today, longtime smokers can receive prevention screening for lung cancer; women 40 (or younger) can receive mammography or other advanced imaging scans to screen for breast cancer.
Prevention. Modern studies are investigating precancerous tissue, identification of biomarkers for cancer, proper screening for hereditary syndromes, lifestyle changes, supplements, anti-inflammatory agents, and effective ways to quit smoking, for example.

Treatment. Removing tumors in the operating room is a mainstay of treatment. Modern innovations include less-invasive laparoscopy, robotic surgery, and techniques such as ablation; a less-is-more approach also has taken hold in some cases, such as in breast-conserving surgery, first proven effective in 1985. In medical oncology, traditional chemotherapy and radiation therapy are still widely used today, but decades of research has spawned a multitude of other options: targeted treatments that interfere with tumor growth or induce cancer cell death while sparing health cells. Deploying the immune system to kill cancer is perhaps the most promising development in cancer care. Available treatments include CAR T-cell therapy (first FDA-approved in 2017), stem cell transplants, and drugs such as monoclonal antibodies. That field is moving swiftly to match immunotherapy for more types of cancer and researchers are studying how to make it more effective. Finally, decades of advances in radiation oncology offers more precise treatment, avoiding injury to the heart and lungs and other healthy organs while pinpointing cancer cells.
*Sources: National Cancer Institute, American Cancer Society, American Association for Cancer Research


WILMOT CANCER INSTITUTE 11
MEET THE NEW CEO
THE FIRST SURGICAL ONCOLOGIST TO ASCEND TO THE TOP OF URMC
David Linehan, MD, says he loved the jobs he had before becoming the highest-ranking person at the University of Rochester Medical Center. He was a surgical oncologist and ardent pancreatic cancer researcher; he was also chair of the Department of Surgery at URMC and an associate director at the Wilmot Cancer Institute, where he led a transformation of the clinical trials operation. He was among the earliest and most enthusiastic supporters of Wilmot’s journey to receive a special National Cancer Institute designation as a top cancer center, which is still ongoing.
Linehan aspired to the higher office and, beginning February 1, 2024, became CEO of URMC and Dean of the School of Medicine and Dentistry. The last time an oncologist held either position was in 1995—and he is the first surgeon and oncologist to have the dual role.
With Linehan as CEO/Dean, it demonstrates a clear commitment by the university toward Wilmot’s strategic goals.
“I understand better than any other CEO or Dean what the challenges are for cancer-care delivery and research.”
Ten years ago, Linehan arrived in Rochester, recruited from Washington University in St. Louis, where he built his career as a surgeon-scientist. He trained at Memorial Sloan Kettering in New York City and in the Harvard University system in Boston. UR leaders were struck by his exceptional skills and a spirit of collegiality. At the UR, he has flourished in all missions—patient care, research, education. He also has embraced community outreach and, for example, was a major proponent of launching a bicycling event that added a new fundraising dimension to Wilmot Warrior Weekend in 2023.
Although he is not from this area and has no relatives in town, Linehan says he has developed a love of Rochester and the Finger Lakes region. He resides in the city with his wife, Janice; they launched two young-adult sons. In the summer, his favorite place to relax is on the coast of Maine, grilling farmers-market food or lobster on his Big Green Egg.

find us on Facebook, LinkedIn, Twitter, and Instagram 12
It’s been a long road from Linehan’s hometown, Boston, where he grew up in the inner city under difficult circumstances: Linehan’s father died when he was a baby, leaving his mother a widow in her thirties with three children under five years old. She sustained herself in an era when “women had to have their husband co-sign to get a credit card,” he says, raising her children alone and founding and directing a small rehab facility for men who struggled with alcohol and drug addiction. That facility is still operating today, 50 years later, with Linehan’s sisters serving as board members.
His mother passed away 25 years ago from leukemia. “My one regret is that my mother isn’t here to see this,” he says, from his C-suite office at URMC.
Following is an edited transcript of a conversation about Wilmot and his transition to CEO.
YOU SERVED AS AN EXECUTIVE FOR NEARLY 10 YEARS. HOW DID YOUR LEADERSHIP ROLES AT WILMOT PREPARE YOU FOR CEO/DEAN OF URMC?
One of the nice things about Wilmot is that it really focuses on all three of our missions, right? Research, education, and outstanding clinical programs. So, everything that is important for the CEO/Dean to have as an experience, I got there.
As the associate director for Clinical Research, I could really roll up my sleeves and get into the nuts and bolts of how to provide administrative support and enroll patients on clinical trials… and clinical trials are hugely important to any academic center. YOU ARE A RENOWNED CANCER SURGEON. WILL YOU BE ABLE TO CONTINUE WITH THAT WORK?
It’s sort of hard to dabble in pancreatic surgery, but it’s important that I maintain a clinical footprint for many reasons. It gives you credibility. You see and hear things when you’re out and about taking care of patients that you wouldn’t necessarily hear and see when you’re sitting in the C-suite. I’m going to continue to follow my current cancer patients; I follow everyone for five years. And I’m going to take some surgical on-call work on the weekends… where I’ll likely end up in the operating room doing some emergency cases.
PEOPLE HAVE DESCRIBED YOU AS A CARING PERSON WHO HAS A TRUE SENSE OF THE URGENCY AROUND PANCREATIC CANCER RESEARCH AND A STRONG CONNECTION TO PATIENTS. WHAT MOTIVATES YOU?
Yeah, I mean, you just come into my clinic, and you see why. In the last 25 years, the five-year survival rates for pancreas cancer have only budged from 5% to about 12%, so there is still a lot of research to be done. It’s not hard to be passionate about it and understand the need to do more when you’re sitting with a dying patient who’s 50 years old and has three kids. We need better solutions.
My research lab (which is studying how to use the immune system to fight pancreatic cancer) will continue its work, but my role will be scaled down. I still have several investigatorinitiated clinical trials that are up and running or about to open. Scott Gerber, PhD (associate professor and co-director of Center for Tumor Immunology Research) and I are partners on an NIH grant. He’s a brilliant scientist. I’m also going to turn over some of the fundamental science work to Brian Belt, (manager of the Tumor Immunology center) who has partnered with me for two decades; and the clinical research will go to Darren Carpizo, MD, PhD, (professor, surgical oncologist, and
co-director of Wilmot’s Genetics, Epigenetics and Metabolism research program). We all work together closely anyway, so it’s easy for us to make this transition.
At the University of Rochester and Wilmot, we’re small enough that we know each other, and translational research tends to happen more organically, unlike some other places that I have been.
YOU’VE WORKED AND TRAINED AT SOME EXCELLENT CANCER CENTERS BEFORE COMING TO ROCHESTER. WHAT DEFINES AN OUTSTANDING CANCER CENTER?
If you look at it from the NIH (National Institutes of Health) perspective, it’s all about research. And not just doing research for the sense of it but showing an impact with your research. Another big piece is community outreach and engagement—that bidirectional communication between the community and our researchers. To understand the needs of the population near Rochester, the cancer burden, and the unmet clinical needs. In all those areas, we’ve made remarkable progress under Dr. Paula Cupertino’s leadership. Going through the preparation for NCI designation has made us a better place.
Community engagement is important for other reasons, too. Wilmot is building these great programs for cancer screening and prevention, and they’re not doing any good if people aren’t participating in them. So, I think it’s about educating our communities.
There is a lot of misinformation out there. When it comes to our health, we want sources of information you can trust, and that’s where we need to be. You build community relationships so that when you go out there with programs, people will say: “These folks are okay. We trust them.”
Patient care is also something we should be very proud of. Every time I make rounds at the Wilmot Cancer Institute, I get rave reviews from patients about the care they get here. And the good reviews are for everyone from the cleaning staff, the nursing staff, the nutrition staff, the physical therapists, etc. We’re talking about people who have just been through something huge, and they’re scared out of their minds because they have cancer—and yet they never fail to compliment the caregivers.
YOU’VE TOLD US THAT YOU ENJOY BEING OUTDOORS: SKIING AT BRISTOL MOUNTAIN, FLY FISHING IN OATKA CREEK, WALKING YOUR DOG IN ELLISON PARK, GOING TO THE ROCHESTER PUBLIC MARKET. YOU’VE ALSO BEEN A HUGE INSTIGATOR FOR THE BIKE RACE THAT WAS ADDED LAST YEAR TO WILMOT WARRIOR WEEKEND. ARE YOU AN AVID BICYCLIST?
Well, I wouldn’t say that (laughs), but I bought a nice bike, and we did a bunch of training rides last summer before the Warrior Weekend in the fall. Helen (Peck, RN, MA, CCRP, executive director of Wilmot’s Clinical Trials Office) encouraged me to go on those rides and they were really fun! It’s a great way to exercise and enjoy the beauty of the region. We did one ride all around Canandaigua Lake—that was a hard one, very hilly. Every time we got to a hill Helen would blow by me effortlessly. We call her “Helen the Hill Slayer.”
Events like the Warrior Weekend are so important for cancer centers. The nice thing is that all the money stays local, and the event relies on small donations, all of which goes to research here at Wilmot. I tried for 10 years to bring that to Rochester, and we finally succeeded. I think you’ll see that it will grow and grow.
13
THE UNIVERSITY OF ROCHESTER MEDICAL CENTER was first in the nation to use an innovative therapy for patients with cancerous tumors in their liver. The modern technology allows doctors to use high-intensity sound waves to remove cancerous liver tissue without any incisions.
The non-invasive procedure, called histotripsy, applies technology developed by HistoSonics. It can be a standalone procedure or serve as a bridge to liver tumor resection or transplantation, especially for those with colorectal metastasis or primary liver tumors. Working with the Wilmot Cancer Institute, a URMC liver care team on December 18, 2023, treated the first person in the nation with histotripsy.
It is important to note that size and location of the tumor can determine whether the new procedure is feasible.
RESEARCH ROUNDUP
News from Wilmot's Bench

TO DEVELOP NEW CANCER TREATMENTS and study how tumors respond, researchers collect tissue and other genetic material from patients, with their consent. Where are these specimens stored? In a Biobank, which is a core facility shared by many scientists. Recently, New York state boosted the Biobank Shared Resource at Wilmot by providing $339,850 to fund renovations and for new technology. Wilmot estimates the investment will result in eight new jobs. Empire State Development awarded the grant through the Finger Lakes Regional Economic Development Council.
John Ashton, PhD, MBA, is director of Wilmot Shared Resources, and Brad Mills, PhD, leads the Biobank.
A GROUNDBREAKING CLINICAL TRIAL, coming soon for pancreatic cancer, is the result of a fundamental scientific discovery at Wilmot. A team led by Darren Carpizo, MD, PhD, was investigating how pancreatic cancer cells genetically reprogram themselves and become stronger as they travel outside of the pancreas to the liver, where pancreas cancer typically spreads. Because of this genetic reprogramming, the cancer in the liver ends up with a different biological makeup than the primary tumor in the pancreas, allowing the metastasized cancer to resist standard treatment.
What drives this process?
A gene known as Netrin-1— and for the first time, Wilmot scientists showed the complex mechanisms that allow Netrin-1 to fuel the genetic changes in pancreatic cancer cells and how Netrin-1 primes the
 PhD
PhD
liver to host cancer. They also discovered in mice that an existing experimental anti-cancer drug suppresses the dangerous Netrin-1 activity. The journal Cell Reports published the findings.
The research team is planning a clinical study at Wilmot for this summer. Eligible patients would take two cycles of the experimental drug before surgery, undergo surgery to remove the cancer, and then take more of the experimental medication along with chemotherapy after surgery for up to six months, says Carpizo, a surgical oncologist and co-leader of Wilmot’s Genetics, Epigenetics and Metabolism (GEM) research program.
Pancreatic cancer is aggressive and has a dismal survival rate because it spreads so quickly and easily. In 85% of patients, the cancer has already metastasized by the time it is discovered.
BURNING/SHOOTING PAIN in the feet and lower legs impacts many cancer patients who take common chemotherapies. Known as “neuropathic pain,” it leads to impaired walking, balance issues, and lower quality of life. There are a couple of drugs available to treat chemotherapy-induced neuropathy, although they do not work for everyone.
A Wilmot clinical study, however, showed that patients can get relief from a wearable, app-controlled device that stimulates the nerves in the lower limbs. Called TENs therapy (transcutaneous electric nerve stimulation), it has some key advantages: TENs devices are available online and at many stores; they are safe, convenient, and the one used in the Wilmot study is already approved by the U.S. Food and Drug Administration to treat fibromyalgia pain.

Study co-author Jennifer Gewandter, PhD, MPH, is excited about the possibilities for cancer patients, but cautions that individuals should consult with an oncologist or primary care doctor before using the device. People with pacemakers and/or epilepsy should avoid TENs therapy.
“Painful neuropathy is such a challenge for patients with cancer and many are reluctant to add more medications to their list,” says
14 Find us on Facebook, Twitter, and Instagram
NEWS BRIEFS
Darren Carpizo, MD,
Wilmot Biobank
Nimish Mohile, MD, neuro-oncology division chief at Wilmot. “This study opens up an option that is safe and will not interact with other treatments that they might be undergoing.”
The Wilmot team was the first to test TENs therapy in cancer patients, and their work was reported in the Journal of Pain
WILMOT’S COLORECTAL CANCER PROGRAM is a national leader in what is known as watch-and-wait organ preservation, having practiced this approach to care for nearly 10 years.

In a recent study in JAMA Oncology, the Wilmot team showed that the number of patients opting out of rectal cancer surgery rose 10 percent between 2006 and 2020. These patients have already responded well to radiation and chemotherapy, and now they undergo frequent follow-ups with experienced oncologists over five years, allowing them to avoid surgery that could alter their bowel function and quality of life long-term.
Study leader Fergal Fleming, MD, MPH, associate professor of Surgery and Oncology, compares it to the evolution in breast cancer care, thanks to continuous research. “Patients used to have very extensive mastectomies and resections,” he says, “whereas now breast conservation is offered wherever feasible.”
Organ preservation for rectal cancer is not yet the standard of care, but it is often available to patients through clinical trials.

RESEARCH SHOWS THAT LOWERING THE DOSE of chemotherapy and adjusting the schedule of how oncologists give chemotherapy to older adults with advanced cancer can make life better for patients, without compromising their treatment goals.
A Wilmot team of geriatric oncologists have been conducting this research for several years to learn how older adults tolerate chemotherapy and its toxic side effects, while retaining the ability to perform daily functions, such as bathing, dressing, eating, and walking. The goal: to help oncologists design the best treatment plans for their oldest patients. The journal JAMA Network Open published the current study, which was led by Mostafa Mohamed, MD, PhD.
Researchers analyzed data from more than 600 study participants over the age of 70 who took part in a national clinical trial known as GAP70+. Compared with patients who received standard chemotherapy, patients who had lower doses had a 15 percent reduced risk of serious toxic effects, a 20 percent reduced risk of functional decline, and 32 percent lower odds of having a worse composite score on all adverse events.
PEOPLE WHO LIVE IN RURAL AREAS and struggle with cancer confront unique challenges related to farm life.
In a Wilmot study of rural-dwelling, older adults who agreed to candid interviews, dairy farmers spoke of challenges around finding someone to take over cow-milking duties during cancer treatment, and other farmers expressed a loss of feeling young and active after cancer struck. All of them had received treatment at one of Wilmot’s 13 locations in a 27-county area near Rochester.

Studying this group of individuals is a major step toward meeting the needs of people in rural areas who have been excluded from clinical trials in the past and are underserved in cancer care.
The objective was to heighten awareness of survivorship needs from the perspective of the patients. Results pointed to a demand for expanded services (including telehealth options), and to create deeper doctor-patient relationships. Importantly, it confirmed that older adults in rural areas are willing to participate in Wilmot clinical trials.
The journal BMC Cancer published the research. Senior author is Supriya Mohile, MD, a pioneer in geriatric oncology and co-leader of Wilmot’s Cancer Prevention and Control research program; co-author Jason Zittel, MD, is a Wilmot oncologist located in rural Dansville, N.Y., at the Ann and Carl Myers Cancer Center.

15 WILMOT CANCER INSTITUTE
Mostafa Mohamed, MD, PhD.
Fergal Fleming, MD, MPH
Supriya Mohile, MD
SAVE THE DATE–Wilmot Warrior Weekend–September
21 & 22, 2024

Organizers have made some adjustments to the 2nd annual Wilmot Warrior Weekend to create an even better experience for team participants, and to provide room to grow as the event expands. The new location is the Xerox Webster Campus, a 1,000-acre complex off Route 104 in eastern Monroe County.
The second annual Wilmot Warrior Weekend will begin on Saturday, September 21, 2024, with packet pickup and a kick-off celebration for fundraisers with food and entertainment. The next day, Sunday, September 22, will feature the signature recreational events: Warrior Walk & 5K and the Wilmot Breakaway Ride. New this year: a beginner-friendly 12-mile biking route, and flatter roads for all cycling events including the 25-mile, 50-mile, and 75-mile ride. Details to come on specific routes and start times for cycling, and the one-mile walk and 5K run.
Bringing the walk, run, and bicycle ride together at the same place on the same day will ramp up enthusiasm and show the strength of Wilmot’s community of supporters and corporate sponsors who are invested in “leaving cancer in the dust,” organizers say.
Last year, more than 1,500 cancer survivors, families, and community members raised over $353,000 for Wilmot’s cancer research and survivorship programs during Warrior Weekend. The impact of the fundraiser resulted in Wilmot leadership presenting a first-ever team science pilot funding award to Brian Altman, PhD, and Minsoo Kim, PhD. They are investigating whether a disruption in circadian rhythms, or the “biological clock” or “sleep-wake cycle,” makes cancer cells less receptive to immunotherapy.
Wilmot Warrior Weekend has something for everyone— walk, run, ride, or volunteer. To learn more and to register: www.WarriorWeekend.urmc.edu.

Support for Wilmot Cancer Institute comes from communities in Rochester and across the upstate New York region. During the past five years, these community supporters have donated a total of $1.9 million to benefit Wilmot cancer research and survivorship programs.
Most donations come from grassroots charity events, including lemonade stands and school fundraisers, tractor pulls, craft fairs, music festivals, cornhole tournaments, athletic events, motorcycle rides, and golf tournaments. No event or donation is too small, and every dollar raised stays local. Thank you to all of Wilmot’s long-standing community partners, groups, organizations, and to the cancer survivors and families who dedicate their time to raise awareness and donate funds to Wilmot. To join the cause, or for more information, please contact: Barbara Balcaen at Barbara.balcaen@rochester.edu

Save the Date for 2024 Survivors Night with the Rochester Red Wings
Anyone impacted by cancer is invited to celebrate the tenth year of Wilmot Cancer Institute’s Survivors Night with the Rochester Red Wings on Friday, July 26. As in years past, the evening will include a pregame presentation and on-field survivors flag ceremony as well as post-game fireworks. More details to come; check www.Wilmot.URMC.edu or watch Wilmot’s Facebook, Instagram, and Twitter/X accounts as the date gets closer.
16 find us on Facebook, LinkedIn, Twitter, and Instagram
ADVANCEMENT NEWS

" " I walk to honor my friends and family, and the Wilmot Cancer Institute doctors, nurses, and researchers–they’re making a real difference and saving lives. They’re all part of my team. Emily Robbins, T-Cell Acute Lymphoblastic Leukemia survivor #WilmotWarrior Register | Form a team | Sponsor warriorweekend.urmc.edu WARRIOR WEEKEND September 21-22, 2024

Wilmot Cancer Institute
601 Elmwood Avenue, Box 704 Rochester, NY 14642
@wilmotcancer
@wilmotcancerinstitute
585 Cornhole Group
A Night of Laughter Fundraiser
Adding Candles BE uninTIMidated
Big Dan Classic Cornhole Tourney
Breaking Ribbons Fundraiser
Brighton Field Hockey Booster Club
Calkins Road Middle School
Compane Trattoria Golf Tournament
Coop Cup Tournament
Crosby’s Fund-Kelly Family Cuidiu Foundation
Crossroads Chiropractic
Cruisin’ Against Cancer
Del Lago Resort and Casino
Edelman Gardner Cancer Research Foundation
Wilmot
Advisory
Mark
R.
Patrick
Ralph
Barbara
Elizabeth Amisano Ovarian
Cancer Education Fund
Farmhouse Fabulous
Flavors of Fall
Foot Performance Center, Inc.
Forbes Memorial Golf Tournament
Good Causes, Inc.
Goodness Fest
Haylee & Presley – lemonade stand
Hilton Jr. Cadets Football & Cheerleading
Italian American Sport Club
John J. Memorial Golf Tournament
KM Memorial Group
Kovalsky-Carr
Margery Coughlin Pawluk Golf Tournament
Marriott “Ditch the Uniform Day”
Mary’s Angels
MC’s Dugout Brian Reed Memorial Golf
Mendon Center Elementary
MO Open Golf Tournament
Nancy & Friends
Northstar Christian Academy “Dress Down Day”
Notre Dame Alumni
Oswego Lacrosse Team
Palmer/Head-Strong
Pancreatic Cancer Association of WNY
Peak Performance PT
Pittsford Federal Credit Union
Pull for the Cure
Retired Professional Fire Fighters Cancer Fund
Saints Sports Booster Club
Scare Brain Cancer Away 5k/Walk
St. Agnes School
STEEL Lillies
Steve Coleman Memorial Golf Tournament
Strollin’ for the Colon
Trails for Travis
Warsaw Central School
Webster Schroeder High School
Webster Thomas High School
Women’s Golf Association
Gregory
Colleen Wilmot
Thomas Wilmot
Bruce Zicari, II
Non-Profit Org. U.S. Postage PAID Permit No. 780 Rochester, NY
/wilmotcancerinstitute @wilmotcancer
Cancer Institute
Board Members,
Yates, Chair
Biddle Moore
'23-'24 Richard
Geri
Cleary
Scott Burdett
Cunningham Garth Hankinson
Landers
McKenna
Kathy
John
Olney
Parkes
Walter
Pluta-Randall
Pluta
Pluta
Stanat Eduardo Torrado Rev. Virginia Tyler Smith Jerome Underwood Angela Uttaro Kristin Vanden Brul Paul "PJ" Wilmot Keith Yeates John Zicari Emeritus Members Judy Linehan Jim Ryan, Jr.
Members Kellie Anderson Clare Flanagan
W. Friedberg, MD, MMSc Hartmut “Hucky” Land, PhD Honorary Board Members Dr. George Abraham Elaine Bucci Michael Buckley Rina Chessin Elaine Del Monte Richard DiMarzo Malik Evans Joan Feinbloom Janet Felosky James Hammer Paul Hanrahan Gary Haseley Mark Kokanovich Michael Linehan Ronald Maggio Steve McCluski Jett Mehta Carol Mullin Michael Norris Jeff Pierce Cheryl Pohlman Larry Rabinowitz Don Rhoda
Mary
Ronald
Erika
Ex-Officio
Jonathan
Smith
Whitman
Steve
Williams
Timothy W.
Dennis Wilmot
Timothy P. Wilmot
Thank you to our incredible community partners who fundraise for Wilmot Cancer Institute!
