M A Y 2 0 2 3
Stroke: How We Communicate and Recover After a Stroke
May is National Stroke Awareness month. There’s a lot to know and understand about stroke. Stroke is not only experienced in the elderly population. Stroke can happen to anyone, at any time. In fact, one in five people who have a stroke are under the age of 55. As many as 10% of people who experience stroke are under the age of 45. However, the majority of strokes happen in people 65 years and older.
According to the National Heart Association’s 2023 updated statistics, stroke ranks #5 of all causes of death in the United States, and results in over 160,000 deaths. This number has dropped within the last few decades. Prior to 2008, stroke was the 3rd leading cause of death in the United States. In 2008, it became the 4th leading cause. Just 5 years later, in 2013, it dropped to the 5th leading cause, indicating progress in prevention and treatment of stroke. As of 2019, stroke was the 2nd leading cause of death and lost-years due to disability worldwide.
Stroke affects groups of people differently. People of African American, Hispanic and Asian/Pacific Islander descent are at higher risk for stroke. Central, Southeast and East Asia, Oceania and Sub-Saharan Africa have the highest rates of overall stroke mortality. Black Americans have a higher prevalence of stroke (and the highest mortality rate) than any other racial group.
continued on page 6
ASK THE EXPERT: MENTAL HEALTH
FEATURE 1: STROKE: HOW WE COMMUNICATE AND RECOVER AFTER A STROKE
FEATURE 2: HUNTINGTON’S DISEASE: WHAT YOU NEED TO KNOW

MAY 2023 - 1
Don’t worry. It was decaf.
October is a gentle month. There are constant reminders of change. we are lucky, toward each other. We have lingering conversations over the flames flicker. Smoke dances around us in a circle. We zip our jackets
Well, it’s official: fall is here. I had my first pumpkin-spiced latte just two days ago, as the evening temperature dipped low enough to merit a fleece.
Don’t worry. It was decaf.
can name the unnameable and communicate the unknowable.
May is here, the opening of summer for those of us in the south. Our allergies have kicked in. The flowers are in full bloom, and we hopefully sit somewhere lovely with an iced beverage, sighing before the heat of summer begins clinging to the skin.
 - LEONARD BERNSTEIN
- LEONARD BERNSTEIN
This month, we’re heavy on the sciences as we explore stroke and Huntington’s disease (HD). May is both National Stroke Awareness Month and Huntington’s disease Awareness Month. We have much to learn about each health issue. We’re grateful to have experts in both fields offering insight, advice and knowledge for ONC readers and the community.
In this month’s feature, we’re starting an important conversation: care community for ourselves or a loved one? Fox Hollow Senior Robin Hutchings offers inside perspective for making this decision.
October is a gentle month. There are constant reminders of change. We turn inward, toward warmth we are lucky, toward each other. We have lingering conversations over tea. We burn fires and sit in silence the flames flicker. Smoke dances around us in a circle. We zip our jackets and consider hats.
In Ask the Expert, Amy Natt answers a reader’s question regarding what away without any estate planning. Without a will or access to important
Dr. Claudia Testa, Founding Director of the UNC Huntington disease (HD) Program, helps ONC readers gain awareness and understanding of Huntington’s disease, a disease causing a breakdown of nerve cells in the brain. Dr. Testa provides answers to our questions about HD’s disease process, the symptoms of HD and how lifestyle changes can impact a person’s symptoms and quality of life.
In this month’s feature, we’re starting an important conversation: how do we choose the proper care community for ourselves or a loved one? Fox Hollow Senior Living’s Sales and Marketing Director, Robin Hutchings offers inside perspective for making this decision.

Physical therapist Dr. Sara Morrison of Total Body Therapy and Wellness potential diagnostic tools used in physical therapy to help diagnose and these tools differ from what other doctor’s offices may offer.
It has always been universally understood that listening to favorites is enjoyable and can lift one’s mood. However, during the past few years we’ve come to better understand the therapeutic value music can have on those with dementia.
For qualified individuals, AOS & Friends Care o ers a program which provides a music player loaded with personalized songs.
Speech Language Pathologist and Integrative Health Coach Abbe Simon helps us understand how stroke affects communication, how to help those living with stroke recover and build new neural pathways, and how care partners can collaborate and support this growth. Simon’s 26 years in the field offer not only the technical knowledge we need regarding stroke but also the human, social connection we must make to help our loved ones (and ourselves) heal.
In this month’s Ask the Expert, Care Manager Ashley Seace responds to a reader feeling depressed and lacking motivation. She explores mental health and gives actionable advice for what to do next if you’re feeling down.
I’m going to agree with Nathaniel Hawthorne this month, who wrote:
We value your trust and loyalt y. O ur commitment to your s afet y remains our numb er O NE priorit y. We're e xcite d to we lcome you back to a s afe
I cannot endure to waste anything so precious as autumnal sunshine spent almost all the daylight hours in the open air.
In Ask the Expert, Amy Natt answers a reader’s question regarding what to do when a loved one passes away without any estate planning. Without a will or access to important accounts, what does a family Physical therapist Dr. Sara Morrison of Total Body Therapy and Wellness helps readers understand potential diagnostic tools used in physical therapy to help diagnose and treat pain. You’ll want to learn these tools differ from what other doctor’s offices may offer.
We are happily accepting new patients!

I’m going to agree with Nathaniel Hawthorne this month, who wrote:
Here’s to enjoying the October sunshine, falling leaves and daylight hours.
Finally, we have the privilege of honoring mothers across the world and in our own homes this month. Happy Mother’s Day to everyone who is a mother and has loved a mother in our lifetime.
I cannot endure to waste anything so precious as autumnal sunshine by staying in the house. So I spent almost all the daylight hours in the open air.
Here’s to enjoying the October sunshine, falling leaves and daylight hours.
facebook.com/agingoutreach/ instagram.com/agingoutreachservices/
e in Aging Well Experts

2 - MAY 2023
LETTER FROM THE EDITOR
Amy Phariss, Editor-in-Chief , OutreachNC | editor@outreachnc.com AOSNC.com
OCTOBER 2022 - 2
LETTER FROM THE EDITOR
instagram.com/agingoutreachservices/ Amy Phariss, Editor-in-Chief , OutreachNC | editor@outreachnc.com We are passionate about helping older adults navigate the many challenges of aging. 910.692.0683 AOSNC.com Age the Way You Choose LETTER FROM THE EDITOR Amy Phariss, Editor-in-Chief, OutreachNC | editor@outreachnc.com
facebook.com/agingoutreach/
MAY 2022 - 15 305 Page Road | Pinehur st , NC
Music
WhatCan WE DoToHelp ? To learn more about the Personal Music Player and other AOS & Friends Care programs/services: 910.585.6757 info@aosfcare.org www.aosfcare.org www.facebook.com/AOSFriendsCare e in Aging Well Experts 910.692.0683 | AOSNC.com Schedule a care management consultation in May to receive a copy of our Life Planning Guide.



















MAY 2023 - 3 Join us for a week of fun! Benefits the Alzhiemer’s Association For more info, visit www.racquetclubatsevenlakes.com POWER FOR PURPLE PALOOZA June 17. Murder Mystery Night Seven Lakes CC June 19. Golf Tournament Seven Lakes CC June 21. Tennis Pro Give Back Racquet Club @ Seven Lakes June 23. Music/Food Truck Sandhills Winery June 24. The Longest Day Events Racquet Club @ Seven Lakes 5K Fun Walk/Run, Tennis, Pickleball, Cornhole, Music, Car Show, Silent Auction, Bake Sale, Raffles and more Together, we’ll raise funds and awareness for Alzheimer’s care, support, and research. 305 Page Road | Pinehur st , NC We value your trust and loyalt y. O ur commitment to your s afet y remains our numb er O NE priorit y. We're e xcite d to we lcome you back to a s afe We are happily accepting new patients! LorenzCreedLaw.com Our 2022 Tyler Chriscoe Attorney at Law Tyler@LorenzCreedLaw.com Margaret “Mia” Lorenz Attorney at Law MLorenz@LorenzCreedLaw.com LorenzCreedLaw.com | 910-695-8688 230 N Bennett St. Southern Pines, NC Our Practice Is Your Solution ∙ Estate Planning & Elder Law ∙ ∙ Real Estate ∙ ∙ Business Law ∙ ∙ Probate & Guardianship ∙ The Lorenz & Creed Law Firm represents cases pertaining to:
Question:








Lately I’ve been feeling a little down and my family thinks I may be depressed. I just have no desire to do things I once loved, and I cannot find joy in my life. Do you have any advice on what I can do to change my situation?

As the days grow longer and the sunshine more consistent, there is hope in the air. I find myself sitting outside in the evenings, before the mosquitoes devour my ankles, and watching the sun set. I stop every now and then, on a walk with the dogs, and look out over a field or pasture and stand in awe of something as simple as the slight movement on a pine tree in the spring air. In many ways, there is an awakening in May, a transition to summer that we feel in every area of life. We’re out more often with friends. We’re taking our meals to the back porch. We’re opening windows, sweeping away the pollen and putting ice in our drinks as the afternoon rolls around. Sweater weather is officially gone.
Answer:
Great question! It is very common for people to go through depressive episodes at any point in their lives, and they don’t always have a trigger for causing them. You are not alone in your situation, and everything you are feeling is completely valid.
At ONC, we love a little gardening for the May issue. This year, we explore the idea of returning to our roots, literally, in a time when costs are rising and our waistlines expanding. Keith Wells, who just moved to the Sandhills in his own retirement, helps us dig into home gardening and, specifically, herbs and spices. If you’ve ever wanted to eat healthier, fresher, homecooked food, this article is for you.
In this month’s Ask the Expert, Ashley Seace responds to a reader’s question about deciding on care for a loved one.

And we’ve got recipes for you to use those herbs and spices in your cooking, whether you grew them or bought them. In the end, good food brings us together, nourishes our bodies and reminds us that what we need is below us, above us and all around us.
We must agree with the words of Aristotle:
Happy digging,


The first thing you should do is talk to your doctor. If you notice you’re feeling depressed, with no desire to do things you love, you should seek medical attention. Your doctor may encourage you to see a psychiatrist trained in mental health disorders. A family doctor and a psychiatrist (or psychiatric nurse practitioner) can both determine if medication is an option for helping with your depression, and both can prescribe these medications. Your doctor can also identify any other health issues that may be contributing to these feelings including side effects from other medications. Seeing your primary care doctor is a great first step in the right direction to feeling better.
In addition to seeing your doctor, many people begin counseling with trained mental health counselors (Licensed Clinical Mental Health Counselor or Licensed Clinical Social Worker). These counselors are professionals who encourage you to talk freely about what is going on and why you might be feeling the way you do. They can also explore with you multiple forms of therapy which may be helpful. The website PsychologyToday allows you to select different filters to find a therapist in your area. Your therapist will help you find tools to use when you’re feeling depressed. If you don’t think your first therapist is a good fit, you aren’t alone! Many people go through a few therapists until they find one that is just right for them. There are various types of therapy including Cognitive Behavioral Therapy, EMDR, EmotionFocused Therapy or Dialectical Behavioral Therapy. Your therapist will help you determine which one will work best for your situation. Mental health disorders can be scary because they are invisible. In actuality, you are not alone; a majority of people will experience some type of mental health problem in their life. It is hard to remember this on the bad days, but your thoughts and feelings are completely valid, and you are allowed to have them. Try not to forget that sometimes it’s OK to not be OK.

4 - MAY 2023
Ashley Seace, AOS Care Manager | ashleys@aoscaremanagement.com MAY 2022 - 2 LETTER
Amy Phariss, Editor-in-Chief , OutreachNC | editor@outreachnc.com
ASK THE EXPERT: MENTAL HEALTH
FROM THE EDITOR facebook.com/agingoutreach/ instagram.com/agingoutreachservices/
In all things of nature there is something of the marvelous.
Age the Way You Choose. e in Aging Well Experts 910.692.0683 | www.AOSNC.com We understand family caregivers deserve a break! We can refer carefully screened private-duty caregivers who will work according to your needs and schedule. AOS At Home Care is the first accredited Caregiver Registry in North Carolina
continued from page 1
STROKE: How We Communicate and Recover After a Stroke
by Amy Phariss
Women experience more stroke than men and are more likely to die from stroke than from breast cancer. In the United States, for example, the lifetime risk of stroke for women is approximately 21%. For men, the risk of stroke is lower, at 1417%.
While these statistics are sobering, there is good news. According to the CDC, 4 in 5 strokes are preventable. We can take action to prevent stroke. Lifestyle changes can have big preventative impacts including limiting alcohol, stopping (or avoiding) smoking, eating a healthy diet, getting plenty of exercise and controlling chronic illness such as diabetes, high cholesterol, high blood pressure and others. In addition to stroke prevention, treatment and support post-stroke can greatly improve recovery and quality of life.
As we gain awareness of this important health issue, ONC is grateful to speak with Speech
Language Pathologist (SLP) Abbe Simon, who works regularly with people recovering from and impacted by stroke. Simon answers our questions about how stroke affects communication, how to treat stroke-related neurological language disorders and how care partners and loved ones can best help those recovering from stroke. We are thankful for Simon’s 26-years of experience in the field, allowing us a window into how consistent skilled therapy can impact not only stroke survivors but their families and loved ones, too.
ONC: One of the most common neurological communication issues faced by those who’ve had strokes is aphasia. Can you explain aphasia and how it relates to stroke?
Abbe Simon: Aphasia is an acquired language disorder that can impact a person’s ability to comprehend language, read, write and speak. Aphasia is a 7-letter word most Americans have
MAY 2023 - 5
never heard of unless it shows up in their life. About 25 to 40% of strokes cause aphasia, and stroke is the leading cause of aphasia.
Aphasia is strictly a disruption in a person’s ability to access their language. Aphasia does not affect one’s intellect. All of the information and knowledge they had before the stroke is completely intact. Aphasia presents itself differently depending on where in the brain a stroke occurred. This location in the left hemisphere of the brain, determines what type of language impairment a person might have. Language includes speaking, understanding, reading and writing. Someone with aphasia could have impairments in all or some of these areas. And depending on the location of a stroke, a person can have impaired speech production that results from a motor speech disorder or muscle weakness. This refers to conditions known as apraxia or dysarthria that impact articulation from being produced clearly. Communication results from a person’s ability to use language and when there is damage to part of the brain responsible for language, successful communication can be challenging. With the guidance of a skilled SLP, a person with aphasia can improve and effective communication can be achieved. Without the proper types of communication tools or supports, a person with aphasia is without their communication right. Just because a person is unable to speak like they once were, it does not mean they have nothing to say or ask. It’s a disservice if anyone attempts to speak to someone with aphasia and determines that they’re not competent or capable because they’re not able to communicate, if they haven’t offered them different options of communication.
ONC: What are the primary symptoms of aphasia?
AS: The primary symptom is the feeling of a word being on the “tip of your tongue” and not being able to say the word in the moment you want to say it. It’s called “word finding difficulty,” which a lot of people can experience if they haven’t had a stroke. It’s like knowing you know a person’s name, but you can’t say it at that moment
There are different kinds of aphasia that are present differently depending on the location, size, and severity of a stroke. Sometimes people produce words that are effortful and faulty, so speech comes across as choppy and not as smooth as a regular conversation. This is called non-fluent aphasia. Fluent aphasia can be described as connected sentences that do not necessarily contain real or intended words. This type of language pattern can be tricky to decipher and often includes comprehension deficits so a person may be less aware of their errors. A trained SLP will be able to know the type of aphasia one has and the therapies needed. Another thing about aphasia is how isolated people can feel. When you add a communication disorder on top of any kind of physical symptoms that might result from a stroke, other people may not know how to respond. They can feel intimidated or scared or turned off by these new communication symptoms. Unconsciously they may avoid the person who has had the stroke or not allow the time and space for them to express their new communication needs. And that most importantly, they are still the same person.
ONC: What is the biggest myth about aphasia?
AS: That it can never improve, that there is a plateau to one’s ability to improve their aphasia. This is completely untrue. The brain benefits from neuroplasticity and can continuously make changes given the proper input. When a person is motivated to make a change, you are never, ever too old to make changes.
ONC: What other communication problems can affect someone after a stroke, besides aphasia?
AS: When a stroke happens on the right side of the brain, you might have cognitive or cognitive linguistic issues, which include skills of higherlevel thinking such as insight, problem solving, and reasoning. These impairments can affect your ability to communicate. And as I mentioned before, some strokes can affect the production and intelligibility of speech. Lastly and location dependent, swallow function can be altered.
ONC: Which treatments can help with speech and communication issues following a stroke?
6 - MAY 2023
AS: So, working with a skilled speech therapist who understands acquired language disorders in adults, who can recognize that all treatment needs to prioritize the individual person’s goals, will be able to incorporate evidenced-based therapies that target the communication strengths and weaknesses. These are determined by the therapist and assessed all the time.
A CLIENT’S MOTIVATION, WILLINGNESS AND BELIEF ARE INSTRUMENTAL IN THE PROGRESS THEY CAN MAKE IN SPEECH THERAPY.
What they do in speech therapy must be done 10x more outside of the therapy environment. So, having the support of communication partners is essential to maximizing recovery.
ONC: What is a communication partner?
AS: Anybody who has a relationship with the person who has a communication problem – your hairdresser, your doctor, your neighbor. Anyone with whom you need to communicate is a partner. Since partnerships are didactic, a partner needs to understand and learn how a person with a communication impairment can be successful expressing themselves. It’s like someone who has crutches or is in a wheelchair, they need a ramp, maybe or someone to help them up. Communication partners help someone who needs assistance to be able to understand and express themselves successfully, whether that means verbally or alternatively. When a communication partner is made aware of another person’s communication needs, they have to adapt the style of communication. It’s kind of like, if you are talking to someone who is hard of hearing and they tell you that when there is a lot of background noise, it’s hard to hear, you’d go in another room or ask others to be quiet. Someone who has a communication problem, if you write down the words that are key or salient to the context, it will help them better understand the information. Facial expressions can also help. A communication partner needs to know how best to support someone with a struggle. All communication does not have to be verbal.
ONC: What does “recovered” look like for most patients? Can someone fully recover speech and communication skills after a stroke? Do people return to pre-stroke ability?
AS: That’s the million-dollar question. There’s definitely not a clear-cut answer to that. We know the brain has an ongoing ability to change. When we think of “recovering” we think of two things: rehabilitation (restore a lost function or compensate for something you can’t do anymore). So, you might try to regain vocal quality, for example, to restore your ability to be heard better. But if something is just really impaired, we have to think of ways to compensate for the loss. So, if pronouncing complicated words like celebration or philosophy is hard for somebody to say, we might have these words written down (if they use them frequently) or we’d ask a person if they’re capable of writing them or offer them written choices. So, we have back up means when spoken language is not available. When we are working on speech therapy, we’re working with neuroplasticity, so we’re building new neural pathways in the brain. We can’t get back what was lost, so we’re working with the healthy brain tissue. It takes a lot of time and work, a lot of redundancy and persistence, but it really does work. The brain’s ability to regain doesn’t only happen in a short period of time. There are so many factors. People can make progress and change years later, no matter how long it’s been. But this doesn’t mean every single person is going to achieve the same level of progress.
MAY 2023 - 7
WE ALL HAVE THE RIGHT TO COMMUNICATE. IF SOMEONE DOESN’T GIVE US THE OPPORTUNITY TO ACCESS COMMUNICATION THE WAY OUR BRAIN IS ABLE TO, THEY ARE TAKING AWAY OUR RIGHT.
ONE PERSON’S PROGRESS DOES NOT DICTATE ANOTHER’S, AND NO TWO STROKES ARE THE SAME.
Again, it’s so important to mention one of the principles of neuroplasticity: “use it or lose it.” So, when you learn new things, you have to apply them and use them, or the brain won’t be able to do them consistently.
ONC: As caregivers and loved ones, what do we misunderstand about speech after a stroke? What are we missing?
AS: The biggest myth is that in the absence of prestroke speech, the person is a different person and shouldn’t be included in conversation. Just because a person’s speech is different doesn’t mean they don’t have anything to say.
At the same time, it’s okay for a care partner to be frustrated. There is validity to those feelings. Being open and honest about that can’t be ignored. Being open about feelings and frustrations is really important. Care partners need support too. They need help and education. But when the “patient” is discharged with a list of prescriptions and referrals, there is no prescription for the care partner. You’ll notice I use the word care partner instead of care giver. That is because of how strongly I feel about relationships being a partnership and that even after a stroke, that person can still find ways to give and take and that none of us should “only” give.
As a health coach for care partners, I realize they need support too. There can be feelings of resentment, frustration, overwhelm and even fear. Care and communication partners may not prioritize their own needs while nurturing and supporting someone after a stroke. Once a new routine has been established and a new sense of “normal” is felt, care partners’ health, wellness, and self-care may need attention. And even though the stroke didn’t occur in their brain, care partners’ lives are impacted, in often a pretty big way. Coaching sessions allow care partners to discover ways to address their own needs without feeling guilty.
ONC: Can you talk about the frustration caregivers feel in not being able to communicate? I imagine the frustration is on both sides, for the person who survived the stroke as well as for loved ones and caregivers.
AS: I think that when things happen in our life that we weren’t expecting or can’t control, we don’t know how to respond. When a stroke shows up in someone’s life, they can be 27 or 72 years old, the reaction is often a sudden, drastic, traumatic experience. People tend to rise to the occasion and do whatever they can for the person who’s had the stroke. They try to do anything they can to prevent another one. All the focus happens on the stroke survivor. If the needs of the family members and care partners are not met or even acknowledged, the relationship can become resentful and frustrated. And like in any relationship, communication is key. So now in the setting of relationship strain, we add a communication impairment, what do you imagine happens? More resentment and frustration for sure. To alleviate and improve this, counseling and supportive communication environments can allow these issues to be addressed. I feel so lucky that my dual role as SLP and health coach allows me to be an integral person in this process. I love watching progress unfold.
ONC: Finally, what advice would you give for someone who is struggling to communicate after a stroke? Any words of wisdom from someone who works in the field and has supported many people in recovery?
AS: Believe that you can communicate. Accept that it doesn’t only have to be spoken. Be sure to advocate for your communication needs.
IT’S YOUR RIGHT TO EXPRESS YOUR THOUGHTS AND BE INCLUDED IN DECISION MAKING .
Communication goes two ways. It’s not only your responsibility to communicate effectively. The other person has a responsibility as well that might include learning something new or different. And any time any of us are learning something new, we are doing good things for our brain’s longevity!
8 - MAY 2023
HUNTINGTON’S DISEASE WHAT YOU NEED TO KNOW
by Amy Phariss
For many of us, thinking about age-related cognitive dysfunction means two words: dementia and Alzheimer’s disease. We are familiar with these diagnoses. Many of us love someone living with Alzheimer’s disease. The media often focuses on the latest studies or information regarding treating Alzheimer’s and dementia. We know these words and diagnoses.
In fact, dementia is not a disease at all but an umbrella term including a group of conditions. These conditions typically involve thinking and social symptoms that interfere with daily functioning. Symptoms might also include forgetfulness, limited social skills and memory loss, among others. Dementia may take the form of Alzheimer’s disease, mixed dementia, Lewy Body dementia, frontotemporal dementia or vascular dementia.
Under this umbrella of conditions are also disorders including dementia and other neurological disorders, one of which is Huntington’s disease (HD). One of these disorders is Huntington’s disease (HD). Many of us have never heard of HD; if we have, we know little about the disease or it’s progression. In the United States, HD occurs in about every 1 in 10,000 to 20,000 people. It affects men and women equally and affects people of all ethnicities and backgrounds. As a genetic disorder (explained in the interview below), HD can be passed from parents to children. Roughly 50% of children with parents with HD will inherit the gene, which makes testing and awareness of the symptoms of HD particularly important.
As May is Huntington’s Disease Awareness month, OutreachNC is thrilled to sit down with Dr. Claudia Testa, Founder of the UNC Huntington Disease Program and Professor of Neurology at UNC School of Medicine.
ONC: First, can we talk about what Huntington’s disease is and how it fits into memory and cognitive disorders? Is HD a form of dementia?
HD is a monogenic neurodegenerative disorder with a range of possible movement and neuropsychiatric symptoms, and progressive cognitive changes. Let’s break that down:
Monogenic means all of HD is caused by a specific genetic change.
Neurodegenerative means brain cells (neuro) are lost at rates faster than regular aging (degenerative).Range of symptoms means each person with HD will have their own unique experience with what symptoms they have, and which ones get in their way. Everyone eventually develops progressive motor symptoms and cognitive changes that slowly progress to dementia. Dementia is cognitive change that is serious enough to interfere with a person’s usual day-to-day activities.
So, HD is a form of inherited dementia, with symptoms like extra involuntary movements in addition to the cognitive changes.
Many people are familiar with Alzheimer dementia, which has an outsized impact on memory and language. HD can also impact memory and language processing but has the biggest impact in other areas of cognition such as executive function. Executive function includes multitasking, complex sequencing tasks, motivation, and impulse control.
Movement symptoms include trouble walking, talking, and trouble with involuntary extra movements.
Neuropsychiatric symptoms include mood changes like depression, anxiety, and irritability.
MAY 2023 - 9
Parkinson disease is an example of a more common neurodegenerative movement disorder, that also has a range of possible movement and non-motor symptoms.
ONC: Huntington’s Disease has a genetic component. Are there environmental factors contributing to the development of this disease?
HD is always caused by a specific genetic change [called a CAG repeat expansion].
HOWEVER, JUST LIKE OTHER NEURODEGENERATIVE DISORDERS, ENVIRONMENTAL AND “LIFESTYLE” FACTORS MAY STRONGLY IMPACT SEVERITY OF SYMPTOMS AND SPEED OF PROGRESSION.
We think of these as things all brains like, and all brains with cognitive disorders really like. Examples are exercise, limiting alcohol, MIND or Mediterranean style diet, social engagement and healthy sleep habits.
ONC: Can you describe the development of the disease, the progression? Are there supports or interventions that can slow the progression of HD?
People usually develop outward symptoms in mid-life. However, there is a very wide span of age of onset. About 10% of people develop symptoms in childhood, and a similar number develop symptoms in their 70s or later. People may notice motor or cognitive symptoms first; everyone develops both eventually. These both slowly worsen over many years. Neuropsychiatric symptoms can develop at any time in the disease course. These symptoms appear to be more variable person to person, and over time. Some of these symptoms may come up and then fade out, while others may be more persistent.
The slow progression of cognitive features and variability of neuropsychiatric symptoms is similar to other neurodegenerative dementias, like Alzheimer’s disease. Right now, the main things that may slow the progression of HD are general brain health interventions like exercise and the MIND or Mediterranean diet.
Because HD is strongly inherited, knowing a parent or grandparent has HD can be a motivator for young adults to make positive brain health choices, like avoiding smoking.
KNOWING THERE ARE POSITIVE STEPS WITH REAL IMPACT THAT PEOPLE WITH HD AND AT-RISK FAMILY MEMBERS CAN TAKE CAN HELP RESTORE A SENSE OF CONTROL AND POSITIVE AGENCY IN THE FACE OF A
PROGRESSIVE COGNITIVE DISORDER. ONC:
When someone is first diagnosed with HD, what are the best first steps to take in terms of treatment?
Figuring out where that individual is in their unique journey with HD is important. Do they have any symptoms? What are their current symptom concerns, if any? Do they have family or friend support? A health care team that has access to information about HD? Do they have prior experience with HD through family, or a lot to learn about this new diagnosis? That process helps identify what the person, their support system, and their health care team need to prioritize in order to maximize everyday quality of life and brain health for that individual.
ONC: In terms of treatment and research, what do we still need to learn about HD? Where are the gaps in knowledge?
There is still a lot to learn about how a change in one gene leads to a neurodegenerative disorder. Also, why do people who have the same genetic variant have such different experiences? For example, people with the same genetic variant start showing outward symptoms of HD in their 30s, 40s, 50s, or 60s. Why such a large spread? And how can we leverage that to push everybody’s start of symptoms later and later?
We also do not fully understand what the huntingtin protein does. This is the protein that is altered by the genetic mutation that causes HD. Understanding normal huntingtin functions helps researchers with new therapeutics design, especially disease modifying agents.
On a pragmatic level, we don’t fully understand the barriers to health care that families impacted by HD face. Are people going without a diagnosis? Do they live in an area without neurologic care or genetic counseling access?
WE KNOW THAT AT LEAST 60% OF PEOPLE WITH HD ARE NOT BEING SEEN IN HDSPECIALTY CLINICS AND ARE LIKELY NOT UNDER ANY KIND OF NEUROLOGY OR MENTAL HEALTH CARE.
How can we get them the symptomatic care we know works now, and the cures of the future?
ONC: Three of the disease’s most troubling symptoms include chorea (involuntary movements), irritability and obsessive-compulsive thoughts and actions. Can you speak more about the neuropsychiatric symptoms of HD?
There are several possible neuropsychiatric symptoms in HD. Every person with HD is impacted in their own way and is very unlikely to experience all the possible
10 - MAY 2023
neuropsychiatric symptoms themselves, some are more common. Irritability can be corrosive. It’s difficult as loved ones react to the irritability, but then the person with HD quickly recovers, or when something small generates an out of proportion reaction.
No one likes to be in pain. In fact, I have spent the past 20+ years helping people get out of pain. The most common question I hear is “How can I get this pain to go away?” The answer to this is simple. We first need to know Why you are hurting. Then we can figure out how to stop the pain. So, why are you hurting? There are many different reasons for pain to occur in our bodies. Pain can be due to a problem in the Muscles, Joints, Tendons, Organs or Nerves. It can also be due to Medication, Psychological reasons, or Nutrition
people impacted by HD. In addition to the international HD Youth Organization, HDBuzz, and Huntington Study Group, and national Huntington Disease Society of America and Help4HD, North Carolinians have unique support through the nonprofit HD Reach. You are not alone!
MANY HEALTH CARE PROVIDERS ARE FAMILIAR WITH DEPRESSION, ANXIETY, OR OCD SYMPTOMS BUT ARE NOT TRAINED TO ASK ABOUT IRRITABILITY, SO THIS MAY GO UNTREATED.
One hopeful thing about neuropsychiatric symptoms in HD is that there are many treatment options – this is the area where we have the most to offer, can do the most to alleviate symptoms.
ONC: What are the most recent, cutting-edge treatment options for HD? Are there any trials currently ongoing that may lead to better understanding of HD and possible treatment options?
There are several exciting trials underway. One set of trials is looking at a medication to help cognitive symptoms in HD. If this medication works, it would be a unique opportunity to specifically support cognition in HD. [Disclosure: UNC is a site for these trials – these are the Sage Pharmaceutical trials DIMENSION and SURVEYOR].
Many health care professionals diagnose pain by Special Tests. During these tests, your practitioner will use their hands to push, pull and twist the areas that are causing you pain. These tests are very useful to find what structure is causing you pain. If you place stress on a structure and it increases your pain, it is likely that structure is contributing to your symptoms. Although helpful, many of these special tests are only 60-80% accurate. While this may look good at first, changing the way the question is framed will show that this also means they are 20-40% inaccurate. Misdiagnosis of pain can be very costly. At best it keeps you in pain longer, while in other cases it can allow symptoms to intensify. When you are dealing with pain, missing your favorite activities and sleepless nights… you want to be as accurate as possible!
Other trials are focused on disease modifying agents. These potential therapeutics are designed to slow down the disease process. Different types of agents are being used to target the mutated RNA and prevent brain cells from making mutated huntingtin protein. This is the current cutting edge: directly targeting the genetic cause of HD, ONC: What does support for HD look like? What can a caregiver or loved one do to help someone with a HD diagnosis have a happy, healthy life?
Fortunately, there are a lot of resources out there for
The addition of Diagnostic Imaging in Physical Therapy has revolutionized the way pain is addressed. By utilizing Diagnostic Imaging, PT’s are now able to look inside you
and diagnose your pain with over 98% accuracy. That means that we can find the real problem, or problems, and address them from the beginning. No more trial and error. No more “try this for a few months and if it doesn’t get any better we will try to get an MRI”. With the addition of Diagnostic imaging, your Physical Therapist can now say “From my evaluation it looks like you have a problem in ____. We are going to do a Diagnostic Ultrasound and confirm this and fully check your joint.” In a matter of a few days, we can have your test performed, results given to you and a new, more comprehensive plan to improve your pain.
CAREGIVERS AND LOVED ONES CAN LEARN ABOUT HD, CONTINUE TO RECOGNIZE THE PERSON INSIDE THE BRAIN DISEASE, AND MOST IMPORTANTLY TAKE CARE OF THEMSELVES SO THEY HAVE THE ENERGY TO SHOW UP FOR THE PERSON WITH HD.

Diagnostic imaging in physical therapy includes:
1. Musculoskeletal Ultrasound (MSKUS)
ONC: Finally, how can we all protect our memory and cognitive health? Even if we can’t prevent genetic disease entirely, what can we do to strengthen our cognitive function as we age and give ourselves the best possible brain health outcomes?
Thankfully, all brains like the same things! Cognitive health can be a shared family project that benefits people with inherited dementias and their family members too. The examples I spoke about above (exercise, limiting alcohol, MIND or Mediterranean style diet, social engagement) are great for anyone concerned about brain health. It’s never too late (or too early) to start giving our brains what they love.
ONC thanks Dr. Testa for her insight and knowledge regarding Huntington’s Disease. We also thank Latorius Adams, a frequent contributor to ONC, who currently works with Dr. Testa as the Family Support Specialist for the UNC Huntington Disease Program. Ms. Adams’ commitment to providing information and support is invaluable for our readers and the community.
MSKUS is a safe, non-invasive, and painless diagnostic tool. It is used to diagnose structures such as tendons, muscles, bursas, ligaments, nerve entrapment/pinching and joint structure changes. Like a video, MSKUS captures real-time images of body structures and can assess a joint/area while it moves. This feature is especially useful as many times pain does not occur at rest, only with movement.
MAY 2023 - 11
OCTOBER 2022 - 10 PT: WHERE DO
SYMPTOMS COME FROM?
Open Arms Retirement Center Assisted Living | Memory Care | Music & Memory Certified 612 Health Drive | Raeford | 910-875-3949 www.openarmsretirement.com Let us help you in making a decision about the care you are seeking. “Making a Difference in the Lives of Others”
Dr. Sara S. Morrison, T, DPT, CDT, FCE, CFT, Cert DN, Cert FMT | Owner -Total Body Therapy & Wellness
Friday Flicks
At One Medical Seniors, we believe in building strong relationships with our patients and the local community. We are currently offering in-practice and community events at no cost to keep our senior population healthy and connected.

Come enjoy a film with others in the community and bring your friends and family! We will have refreshments, but feel free to bring popcorn or your favorite movie-watching snack.
May 12, May 19 and May 26
10am
MoRA Practice
4014 Connection Point Blvd., Suite C
Charlotte, NC 28212
May 12 and May 19
1:30pm
Pineville Practice
8332 Pineville Matthews Road, Suite 205
Charlotte, NC 28226
To learn about more about our events, scan the QR Code or visit o oms-clt.eventbrite.com

Looking for a doctor?
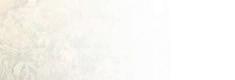
GRAY MATTER GAMES
ACROSS
1. Relay mail delivery
4. Quamash (var. spelling)
10. Egg on
14. Always, in verse
15. Functional
16. Coastal raptor
17. One of three equal parts
19. “Darn it all!”
20. “___ on Down the Road”
21. Santa’s reindeer, e.g.
22. Auditory
23. Undetectable bomber
25. Do, for example
26. Cantankerous
27. “I do,” for one
30. Persia, now
31. Complain
34. In perfect condition
35. Encyclopedia, e.g. (2 wds)
39. The “B” of N.B., Latin
40. Bow
41. “Cast Away” setting
42. Calypso offshoot
43. Certain tribute
48. Attempt
49. Scottish wind instrument
51. Fine-grained sedimentary rock used as fertilizer
52. Cold shower?
55. Length x width, for a rectangle
56. Advocate
57. Science of liquids in motion
59. Caddie’s bagful
60. Upper-story bay windows supported by brackets
61. Deception
62. “B.C.” cartoonist
63. Be a snitch
64. “Absolutely!”
DOWN
1. Can’t stand
2. Freshen
3. Indonesian dagger with a scalloped edge
4. Nod, maybe
5. English race place
6. Sports event in which teams compete to win
7. Not much (2 wds)
8. ___ gin fizz
9. Cast
10. Famous Am. Apache Indian chief
11. Handel bars
12. Designed for defense against armored vehicles
13. Downward slope
18. Accommodate
24. Harp’s cousin
27. Any of various periwinkles
28. “___ bitten, twice shy”
29. Garden intruder
32. “-zoic” things
33. Eat like a bird
35. Stop on the way (2 wds)
36. Equipment that makes a photo bigger
37. Weakest
38. “Lulu” opera composer
39. Atomic number 83
44. Girasol, e.g. 45. In a jaunty manner 46. Coin
Come-ons
MAY 2023 - 13
Cut, maybe 58. “It’s no ___!”
47.
49. Military wear 50. Ever (2 wds) 52. Attempt 53. Vega’s constellation 54.
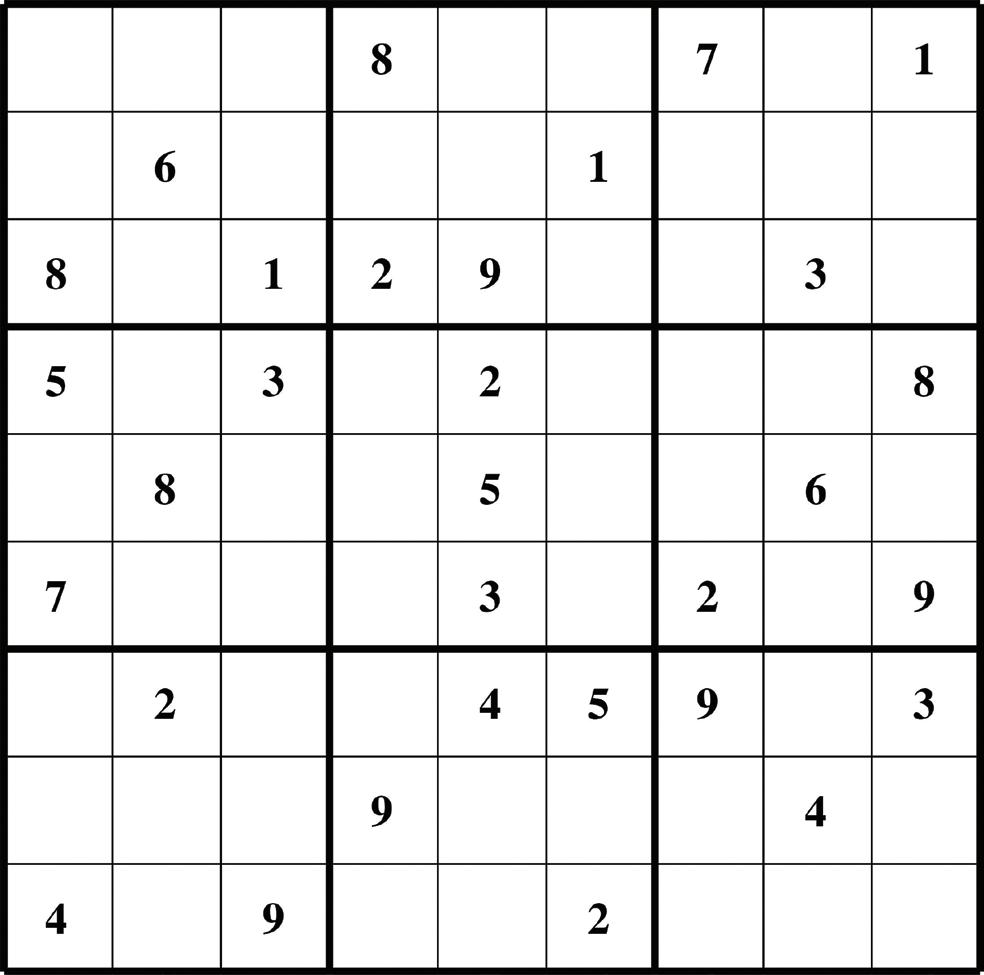
Gray Matter Games Solutions



It has always been universally understood that listening to favorites is enjoyable and can lift one’s mood. However, during the past few years we’ve come to better understand the therapeutic value music can have on those with dementia.

For qualified individuals, AOS & Friends Care loaded with personalized songs.




























To learn more about the Personal Music Player and other AOS & Friends Care programs/services: 910.585.6757



info@aosfcare.org
www.aosfcare.org
can name the unnameable and communicate the unknowable. WhatCan WE DoToHelp ?
www.facebook.com/AOSFriendsCare
14 - MAY 2023
Relay Conference Captioning (RCC) service is available for individuals who have a hearing loss or a speech disability to actively participate in teleconference calls or webinars by reading live captions on their laptop, mobile device or tablet. To inquire, contact kim.m.calabretta@t-mobile.com or visit relaync.com/rcc Accessible Communication with Captions! Relay Conference Captioning
Music


MAY 2023 - 15 I say all of this to tell you healthcare is local and you will get We’re here to help you navigate all things aging! www.AOSNC.com info@AOSNC.com | 910.692.0683 Find current & previous issues of OutreachNC Read the latest from our blog Join our free digital mailing list Sign up for home delivery of OutreachNC; Only $16 for 12 issues Send us your questions RESOURCES. EXPERIENCE. SOLUTIONS. 155 Blake Blvd. Pinehurst, NC 28374 © 2023 Quail Haven Village INDEPENDENT LIVING | ASSISTED LIVING SKILLED NURSING | REHABILITATION On any given day, you’re given a range of options to fuel your passions, satisfy your cravings and indulge your whims. Learn more about luxury senior living at QuailHavenVillage.com or schedule a visit at 910.537.6812 INDULGE your palate & your passions A Life Plan Community offered by Liberty Senior Living 123064 quail haven indulge your palate ad-outreach nc.indd 1 2/15/23 4:17 PM

16 - MAY 2023OCTOBER 2022 - 16 At Fox Hollow Senior Living, our residents have the opportunity to do everything they’ve always loved. With Five Star Dining, days filled with friends and adventures, you can be yourself again – while we take care of the rest. Make Every Day Five Star FOX HOLLOW SENIOR LIVING COMMUNITY 190 Fox Hollow Road • Pinehurst, NC 28374 910-695-0011 • www.FoxHollowSeniorLiving.com ASSISTED LIVING • MEMORY CARE RESPITE/SHORT-TERM STAYS ©2021 Five Star Senior Living Call to visit and explore our community.

