
How We Got Here, Where We Are Now, Where Things are Going
OPIOIDS : SPRING 2024 A Recognized World Center for Advancing Health Care through Science, Education & Technology Plus... The Doctors Lounge Pitt Drops A Bombshell











WE MAKE CARDIOLOGY CONVENIENT. APRIL 5-14 • READING, PA 33RD ANNUAL TICKETS ON SALE NOW! berksjazzfest.com
Philadelphia County Medical Society
2100 Spring Garden Street, Philadelphia, PA 19130 (215) 563-5343
www.philamedsoc.org
EXECUTIVE COMMITTEE
John M.Vasudevan, MD PRESIDENT
Ricardo Morgenstern, MD
IMMEDIATE PAST PRESIDENT
Oneida Arosarena, MD, FACS SECRETARY
Dom Bucci, MD TREASURER
BOARD OF DIRECTORS
Sharon Griswold, MD
Cadence A. Kim, MD, FACS
William King, MD
Elana McDonald, MD
Max E. Mercado, MD, FACS
Natalia Ortiz, MD, DFAPA, FACLP
Dhruvan Patel, MD
David A. Sass, MD, FACP
Katherine Sherif, MD
Walter Tsou, MD
Graeme Williams, MD Rhea Trainson
FIRST DISTRICT TRUSTEE
Michael A. DellaVecchia, MD, PhD
EXECUTIVE DIRECTOR
Mark C. Austerberry




Hoffmann Contents SPRING 2024 Philadelphia Medicine is published by Hoffmann Publishing Group, Inc., Reading, PA HoffmannPublishing.com | (610) 685.0914 FOR ADVERTISING INFO CONTACT: Tracy Hoffmann • Tracy@Hoffpubs.com • 610-685-0914 x201 The opinions expressed in this publication are for general information only and are not intended to provide specific legal, medical or other advice or recommendations for any individuals. The placement of editorial opinions and paid advertising does not imply endorsement by the Philadelphia County Medical Society. All rights reserved. No portion of this publication may be reproduced electronically or in print without the expressed written consent of the publisher or editor. 4 The Doctors’ Lounge: A PCMS program to bring back casual intellectual conversation from doctor to doctor. 8 OPIOIDS: How We Got Here, Where We Are Now, and Where Things are Going 14 Pitt Drops A Bombshell: The PA Health and Environment Studies on Fracking 18 Physicians’ Corner 20 Negotiating Key Employment Contract Terms 22 Communities Join to Tackle Medical Debt in Pennsylvania 24 Edith P. Mitchell, health-care trailblazer, civil rights pioneer, and retired Air Force brigadier general, has died at 76 26 This is Your Lane : Growing Coalition of Physicians Takes On Gun Violence 29 The Legislative Year in Review 2023 31 Humanitarian Medicine
Editor Tracy

The Doctors’ Lounge:
A PCMS program to bring back casual intellectual conversation from doctor to doctor.

4 Philadelphia Medicine : SPRING 2024
philamedsoc.org FEATURE
Pictured left to right: Dr. Wilson Jackson, President of PAMED
Dr. John Vasudevan, President of PCMS
Dr. Baligh Yehia, President of Jefferson Health
Photo was taken at the 1st Doctors’ Lounge session “How to Improve Your Administrative Leadership Skills without an MHA”
 By William King, MD, PCMS Boardmember
By William King, MD, PCMS Boardmember
The Philadelphia County Medical Society was organized in 1895 by physicians coming together to encourage scientific collaboration and clinical cooperation between practicing physicians. The defining word in our group is “society.” Fundamentally the process of bringing together individual clinicians into a cooperative is social. Our current president, John Vasudevan, wants to bring back some of the magic of old fashioned social connection between our members with an educational series called “The Doctors’ Lounge.”
Dr. Vasudevan explains the concept this way. “My father is also a physician, and I grew up in an era when doctors’ lounges in hospitals were more common than the rarity they have become today. Even as a child, I was able to visit these lounges when my dad had to work on the weekends, and witnessed something special: a casual place where physicians could relax, refresh, and connect. Most conversations were polite and cursory as someone popped in for a cup of coffee and a pastry. However, there were other times when I witnessed physicians across specialties sharing stories and insights not only about patient care, but about business, finances, the health care system as a whole, and even
common challenges of life. It was a place not only to commiserate and communicate, but to inspire one another to improve and excel. The best part was that there was no pressure or formality to these lounges, and the topics discussed were what the physicians in the lounge needed to hear at that time. This is what I hope to recreate – at least, to some extent – in our Doctors’ Lounge events: a place where we mix socializing, food and drink, and casual conversations that might inspire us to maximize our skills as physicians.”
The first program occurred on November 9th, 2023. We were pleased to have Dr. F. Wilson Jackson III, the President of the Pennsylvania Medical Society, and Dr. Baligh Yehia, the President of Jefferson Health, speaking candidly about their pathways to success. The focus was on “How to improve your administrative skills without an MHA,” and both of these physicians provided perspectives on how to influence those in health care administration, and how to take the reins ourselves to optimize health care delivery. Dr. Vasudevan was fortunate to have a long-time personal relationship with each of these colleagues during years of involvement in organized medicine
continued on next page
philamedsoc.org 5 SPRING 2024 : Philadelphia Medicine
FEATURE continued
The Doctors’ Lounge: A PCMS program to bring back casual intellectual conversation from doctor to doctor. continued from page 5


at the national and regional level, and was able to bring these relationships to the PCMS members in a casual evening of conversation. The program had a promising start. Dr. Daniel Dempsey, Emeritus Professor of Surgery at the University of Pennyslvania, has been a decades-long member of the Medical Society, serving as a past President of the PCMS. He responded to the email announcements, and attended the November Doctors’ Lounge. Dr. Dempsey stated, “This was an excellent discussion about pathways to physician leadership. Dr Vasadusen moderated a discussion led by Dr. Yehia from Jefferson and Dr. Jackson, President of the Pennsylvania Medical Society. All three of these doctors are physician leaders and it was interesting to learn how they got to where they are today. The different types of leadership positions held by the physicians as well as their diverse career pathways were very enlightening and generated an evening of stimulating discussion. And as usual the food and drink were very good.”
The November program was off to a good start, and we are looking forward to hearing about the next Doctors’ Lounge February 8th. Our next event will be focused on “How to improve your business strategy without an MBA.” The event will feature Dr. John Pagan, President and CEO of the Pennsylvania Collaborative Clinically Integrated Network, as well as one of the teachers of his MBA program, Dr. Thomas Beeman, a Professor at St. Joseph’s University who worked as an administrator helping to merge Pennsylvania Hospital with Penn Medicine. The goal is to help us understand how to best develop business plans that are effective, and to determine the value of getting an MBA to achieve our career goals. Dr. Vasudevan hopes this intellectual salon will continue beyond his term. “All of my initiatives this year, including the Doctors’ Lounge, are intended to develop relationships throughout our medical community in Philadelphia which can create sustainable activities for years to come. I believe the value of membership in organized medicine should go beyond political advocacy, and that activities that connect us to our community, patients, and each other will strengthen our dedication to organizations such as the Philadelphia County Medical Society.” As we enter 2024, we look forward to enjoying these events for years to come. •
6 Philadelphia Medicine : SPRING 2024 philamedsoc.org
Tom Beeman
John Pagan
DOCTORS LOUNGE
The Philadelphia County Medical Society and the College of Physicians of Philadelphia welcome you to the Thursday, April 11, 2024
Thursday, February 8, 2024
How to Improve Your Business Strategy Without an MBA
How to Improve your Community Engagement Without an MPH
Facing rising rates of burnout and loneliness, some doctors are calling for the return of physician lounges. Once a fixture of hospitals, these dedicated spaces for health workers to rest and socialize went out of style in recent decades as a result of cost-cutting measures.
featuring guest speakers Pennsylvania Secretary of Human Services Dr. Val Arkoosh and Susan and Stanley Plotkin Chair in Public Health at the College of Physicians of Philadelphia, Dr. René Najera.
Our Doctors Lounge series is designed to bring physician and trainee members of the Philadelphia County Medical Society and College of Physicians of Philadelphia together over food and drink to socialize and learn from expert panelists on how to use one's medical degree to advance their goals in business, public health, leadership/administration, and politics. Attendees are welcome to bring a guest.
Event Timeline:
6 - 6:30 PM - Reception
Our second Doctors Lounge will feature a panel discussion on how you can improve your business skills in healthcare without having to obtain an MBA. Learn how you can better position yourself as a credible participant in discussions about organizational direction or in decisions that affect your professional life or specialty.
Speakers:
6:30 - 7:15 PM - Panel discussion

Thomas E. Beeman, PhD, LHD (hon), LFACHE
Professor of Practice
Haub School of Business
About the Doctors Lounge Series:
Saint Joseph University
Rear Admiral (U), USN, (ret)
7:15 - 8:00 PM - Open discussion & socializing
John Pagan, MD, MBA, FACS Chair and CEO
Scan QR for tickets
Pennsylvania Collaborative CIN (PACIN)
General Surgeon
Saint Lukes University Health Network
Facing rising rates of burnout and loneliness, some doctors are calling for the return of physician lounges. Once a fixture of hospitals, these dedicated spaces for health workers to rest and socialize went out of style in recent decades as a result of cost-cutting measures.
Format: 6:00 PM to 6:30
6:30 PM to 7:15
7:15 PM to 8:00

Our Doctors Lounge series is designed to bring physician and trainee members of the Philadelphia County Medical Society and College of Physicians of Philadelphia together over food and drink to socialize and learn from expert panelists on how to use one’s medical degree to advance their goals in business, public health, leadership/administration, and politics. Attendees are welcome to bring a guest.
Cost: $20 for physicians,
Reception Panel Discussion Open Discussion & Socializing
Register here:
https://13284a.blackbaudhosting.com/13284a/ Doctors-Lounge-How-to-Improve-Your-Community-Engagement-Without-an-MPH
***Trainees, please register as a Student to purchase the $10 ticket.
Save the Date for Future Doctors Lounge Events:

• February 8 - How to Improve Your Business Strategy Without an MBA
• June (TBA) - How to Improve Your Political Success without Running for Office
All programs are held on Thursdays and will begin at 6:00 PM unless otherwise noted.
Stay tuned for future Doctors Lounge programs! • April 11 - How to Improve Your Community Engagement Without an MPH • June (TBA) - How to Improve Your Political Success Without Running for Office All programs are held on Thursdays and will begin at 6:00 PM unless otherwise noted.
$10 for
Scan QR for tickets Click Here to Register
trainees
PM
PM
PM

OPIOIDS :
How We Got Here, Where We Are Now, Where Things are Going
Contributing:
Dr Juan Lopez Tiboni – Internal Medicine Resident, Pennsylvania Hospital
Dr Joseph Dorazio – Toxicology and Addiction Medicine, Cooper University Health System, formerly of Temple University
Dr Barbara Westerhaus –Primary Care Physician and Director of J Edwin Wood Clinic, formerly working for Philadelphia’s Ambulatory Health Centers
Catherine Abrams – Program Coordinator, Substance Use Response, Guidance, and Education (SURGE) group of the Health Federation of Philadelphia
8 Philadelphia Medicine : SPRING 2024 philamedsoc.org FEATURE
Philadelphia is a city known for many things: the cheesesteak, the Eagles, the Mummers, and now, Fentanyl. In 2022, 1171 people died in the city from an opioid overdose 1. ‘Philly Dope’, as many patients call it, is unlike other opioids used throughout the United States. Evolving exponentially in its potency out of the not-so-secret open air opioid markets in the city, many patients and providers find themselves in uncharted territory in the struggle against opioid addiction. This new frontier has brought many shifts in addiction medicine practice during the last decade. With the help of some of those breaking new frontiers, Philadelphia Medicine Magazine brings you an update on how we got here, where we are now, and where things are going.
Opioids in the United States
From 1999-2021, 645,000 people died from an opioid overdose in the United States2. In Philadelphia in 2022 alone, 1171 people lost their lives to opioids1, not to mention the immeasurable healthcare utilization and disability burden among those who live with opioid dependence. In Philadelphia in 2012, the number of opioid deaths was 413, close to a third of what it is now.
How did we wind up here?
In order to understand this question, one has to first understand that 0pioids and the United States have long been intertwined. This is not the first wave of opioid abuse in American history. Opioid dependence dates back first to the Civil War, and the same fields of combat where many soldiers lost their lives where wives and daughters grew poppies for opium. In the years that followed, ‘Soldiers disease’, a complex syndrome of pain and trauma in veterans, contributed to the uptake of opium and morphine as a substance of abuse, particularly in the South3. 1920s and ‘30s also saw the rise of heroin in urbanized centres, percolating most notably in the Jazz scenes of John Coltrane and Charlie Parker of the northeast where ‘junkies’ stole discarded materials to sell for scrap to feed their addiction4. Some baseline abuse of heroin remained thereafter, but it didn’t rise to national prominence again until the Vietnam war; at one time it was estimated that up to 20% of US soldiers had some form of heroin dependence. Notably, despite fears, not many of them remained addicted once returning to the US to a change in scenery and social supports. Still, heroin didn’t just disappear at the end of the Vietnam war, and up until the 1990s, nearly all of the heroin use was in urban centers, not widespread throughout America from coast to coast at the level it is now. So what changed?
The arrival of Oxycontin
In 1996, the arrival of OxyContin was promised to be the solution to uncontrolled pain. Purdue Pharmaceuticals, a drug company based out of Connecticut, advertised it to physicians as a wonder-drug with less than 1% potential for addiction. This lack of addictive potency was attributed to its sustained release formulation of the previous availably Oxycodone, that prevented users from getting a true opioid high. Purdue, keen on selling their new drug, launched a targeted marketing strategy at primary care doctors in small, working class towns with high chronic pain burden tied to coal mining throughout the Appalachians. They specifically targeted states with less stringent prescription controls for schedule II drugs5, while simultaneously lobbying heavily for changes in medical practices to more aggressively treat pain through back door funding to groups like the American Pain Society6. Due largely to their efforts, these medications started being prescribed with little reservation in large quantities. Over the span of a few years, it became apparent that the pill was menacingly addictive to those with chronic pain. Additionally, recreational users and prescription abusers alike realised that by crushing the pill, or sucking down the external coating the continuous release mechanism could be circumvented to produce more euphoric effects. This made prescription Oxy abuse commonplace throughout the northeast in small suburban towns all through the late nineties into the mid-2000s7, before the wave of abuse spread outwards into urban centers, the Great Lakes, and throughout to the West Coast. Purdue Pharmaceuticals ultimately plead guilty to its role in the current day opioid crisis, first with a 600 million dollar settlement in 2007 which has since spiralled into an ongoing 6 billion dollar Supreme Court bankruptcy deal8. This relationship with Oxy set the stage for the current opioid crisis nationwide.
continued on next page

9 SPRING 2024 : Philadelphia Medicine philamedsoc.org
OPIODS: How We Got Here, Where We Are Now, Where Things are Going
continued from page 9
Heroin and Fentanyl in Philadelphia
Anecdotal evidence in Philadelphia will tell you that most of our patients suffering from opioid addiction started on prescription pills. To that point, a data review of American heroin users published in 2015 showed that 80% start on prescription opioid tablets, commonly sourced from prescriptions written for themselves or friends and family9.
As part of the 2007 settlement from Purdue, OxyContin was reformulated in 2010. This made accessing and abusing prescription Oxy more difficult, leading users in the city to heroin as it was cheaper and enabled them to better satisfy their withdrawal symptoms and cravings. A quote from a heroin user in the 2018 book Dopesick articulates this transition: ‘If you tried to crunch ’em, they’d gel up on you. You couldn’t even snort ’em, let alone shoot ’em. After that, the pills either went dry or were just too expensive to get. And everybody who used to deal pills starting dealing heroin instead4.’ Over time, the heroin supply on the east coast, funneled through the ports of Philly and Baltimore, was replaced by the exponentially more potent fentanyl produced overseas. The compound is stronger, more addicting, and far more lethal than heroin, which has been largely responsible for the increasing rate of opioid overdoses. ‘I miss heroin,’ I had a patient tell me once in the emergency department. ‘It’s all gone now. Fentanyl is the only thing out there and I hate it.’
Philly dope is now more concentrated with fentanyl than ever before, with conservative estimates that one bag of fentanyl contains the equivalent of 50-100mg of PO oxycodone. ‘There is objectively more fentanyl per bag now than there was before, and this makes controlling withdrawal more difficult. We are talking about patients taking the equivalent of 150 to 200mg of IV hydromorphone daily,’ said Dr Joseph D’Orazio, an emergency medicine trained toxicologist and addictions medicine physician formerly of Temple and now at Cooper. ‘We also have counterfeit opioids in the city that are made outside the US and channeled in through the typical drug smuggling routes. Patients think they are buying prescription caliber opioids which are actually counterfeit fentanyl and xylazine pressed into what looks like an oxycodone 30mg IR tablet,’ he pointed out.
Increasing concentrations of fentanyl are a large contributor to the rise in mortality from overdoses, but so are other compounds now entering the drug supply. ‘90% of the fentanyl on the street in Philadelphia now contains Xylazine (an animal tranquilizer that has euphoric properties but is also more addicting’) Dr. D’Orazio told us. Xylazine, or “tranq,” is not typically used alone but has become a common additive to bags of heroin and fentanyl in the Northeast. It has similar sedative properties to benzodiazepines but behaves somewhat differently, especially when injected, causing necrotic wounds on a scale that hadn’t been seen with injection drug use behaviour of the past. ‘The
necrotic wounds you see with Xylazine. We don’t really know why it causes such severe wounds. There are hypotheses out there that there are caustic effects of the compounds or vasoconstriction mediated effects. More research needs to be done,’ Dr. D’Orazio said. Furthermore, higher potency opioids are already starting to emerge in the drug supply in the form of Nitazines, a new synthetic opioid ten times more potent than fentanyl identified in some autopsy cases since 202110. Physicians on the frontlines of opioid and xylazine-induced toxicity are facing new challenges, and the field of addictions overall has changed massively to try and improve outcomes over the last ten years.
Hospital Management of Withdrawal
We asked Dr. D’Orazio how management has shifted for hospitalized patients with addiction. ‘The major innovation or thinking change in the last decade is giving opioids to patients suffering with opioid use disorder,’ he said. This may seem counter-intuitive, but one has to consider how these cases unfold in the hospital. ‘Patients would come in with cellulitis or a local abscess at a wound site, get seen in the ED, admitted, and then barely get one or two doses of antibiotics before they’d leave to get opioids on the street to self-treat their withdrawal because we stood firm on not ‘indulging their addiction’. They would enter and leave through this revolving door: a cellulitis would become a bacteremia and then an endocarditis, an abscess would become an osteomyelitis; all because none of the medical complications were being appropriately managed up-front due to uncontrolled withdrawal,’ I had a hospitalist at Pennsylvania Hospital tell me once. Dr. D’Orazio echoed how our practice now better helps to address medical issues before they spiral; ‘ten years ago patients had one option and that was to taper and not get opioids.’ Another consideration is that our objective in the hospital should not necessarily be to get people off of opioids, but treat their medical complications first. ‘Not every patient is looking for abstinence or to stop using drugs, and these patients still deserve care the same way that other patients coming in with a medical condition will still get care if they decline certain other elements of care.’ Dr. D’Orazio explained. If anything, trying to get patients off of opioids when they are not interested only places them at greater risk of overdose when they return to the community with a lowered opioid tolerance and use the same doses they did before admission.
Still though, administering opioids for withdrawal is not as easy as it sounds. The ever-changing potency, and new substances entering circulation, means that physicians and hospitals need to be willing to adapt on a year to year basis, making treatment nuances fluid. ‘Ten years ago when we gave patients 30 of methadone for their injection heroin use that was more than enough to control their symptoms but now that’s not going
10 Philadelphia Medicine : SPRING 2024 philamedsoc.org
continued
FEATURE
to touch them. The doses we are able to give in the hospital will just pale in comparison (to how much they get on the street). We have to administer such high numbers that it makes people nervous,’ Dr. D’Orazio noted. This is where multidisciplinary collaboration through nursing, pharmacy, medical, and administrative staff becomes imperative for patients to get effective management. ‘(Temple University Hospital) will administer patients 100mg of extended release q8 for patients that are using a bundle of fentanyl a day, but that’s not a practice that developed overnight. It took us a lot of steps and collaboration over several years to get there,’ Dr. D’Orazio said.
For those that are interested in recovery, groundwork is made in the hospital with the end goal of seeing them long term in the outpatient setting. ‘We try to catch them in a good therapeutic moment to show patients that there are good options for recovery and recovery is not so bad. The recovery numbers for patients coming to the hospital for care of medical complication will never be as good as someone who walks into a clinic off the street. But the goal is to get these patients in the clinic,’ Dr. D’Orazio said.
Outpatient Management
When you’re ready to make a difference, we’re ready to help
We are proud to support Philadelphia County Medical Society by advising them for more than a decade.

Nash Wealth Management Group
Merrill Lynch Wealth Management
1200 Howard Blvd.
Suite 300
Mount Laurel, NJ 08054
856.231.5575
Merrill Lynch, Pierce, Fenner & Smith Incorporated (also referred to as “MLPF&S” or “Merrill”) makes available certain investment products sponsored, managed, distributed or provided by companies that are affiliates of Bank of America Corporation (“BofA Corp.”). MLPF&S is a registered broker-dealer, registered investment adviser, Member SIPC and a wholly owned subsidiary of BofA Corp.
Transitioning out of the hospital and into the clinic is a different arena entirely making its own advances, and it starts with a frameshift in our approach. ‘We need to start thinking about opioid use disorder as a chronic medical disease like hypertension, diabetes, or asthma. With patients who have been injecting opioids for years, it is often a lifelong disease. We are not ‘curing this disease’ the same way that we are not ‘curing diabetes’ in most patients. Nobody has decided to have this problem the same way that patients don’t decide to have cardiovascular disease. It is contributed to by both genetic and environmental factors. We don’t end addiction, we manage opioid use disorder the same way that we manage diabetes or hypertension,’ Dr. D’Orazio said. Furthermore, we shouldn’t have punitive expectations to setbacks, and instead approach the disease more like we do other chronic diseases
Investment products:
Are Not FDIC Insured Are Not Bank Guaranteed May Lose Value
© 2023 Bank of America Corporation. All rights reserved. | MAP5448947 Vault-BA1KP6 |
MLWM-243-AD
470945PM-0323 | 03/2023
influenced by lifestyle. ‘If your diabetes patient comes in and on this day their sugar is high, we work with them and assess their social determinants of health to find out what is their barrier to getting good diabetes control. Just like other disease there are some that get prescribed a medication and hit the ground running and there are others who have comorbid psychiatric conditions convoluting their management that benefit from counseling. This is a stigmatized disorder as many people continue to think that substance use is a moral failure,’ Dr. D’Orazio pointed out.
continued on next page
philamedsoc.org 11 SPRING 2024 : Philadelphia Medicine
OPIODS: How We Got Here, Where We Are Now, Where Things are Going
continued from page 11
The medical tools at our disposal continue to evolve as well. Methadone maintenance therapy, once the standard, is now just one of many different medications for opioid use disorder (MOUD). Catherine Abrams, Program Coordinator of the Substance Use Response, Guidance, and Education team of the Health Federation of Philadelphia, offers training for providers who are interested in learning how to prescribe buprenorphine and she walked us through the different tools. Buprenorphine is a partial opioid agonist with stronger affinity to the opioid receptor than opioids of abuse. Buprenorphine is available as a sublingual strip called Suboxone or as a long-acting injection (Sublocade and Brixadi). ‘The newest player is Brixadi, a differently formulated injectable buprenorphine recently approved by the FDA, and a lot of people are very excited about it,’ she told us. Learning how to prescribe these agents is relatively easy through groups like the Health Federation of Philadelphia. They provide free training for interested physicians and bi-monthly meetings for providers to come together and discuss specific challenges. Their goal is to get more physicians comfortable with prescribing these medications to help reduce the overall burden in the city.
Dr. Barbara Westerhaus, a primary care physician and medical director of the J Edwin Wood Clinic at the Univeristy of Pennsylvania, has experience in treating this population and rallying other physicians to join the fray. For many years she worked at the City Health Centers integrating MOUD into her primary care practice. ‘This is a medical condition that we have to manage, and until we accept that, it remains stigmatized. We view this as a primary care problem. Primary care doctors can’t just say ‘I am not treating Covid or diabetes’, and the same goes for opioid use disorder. A primary care doctor should never be turning away a patient for lack of knowledge with substances like suboxone. I just don’t think we can say no at this point with so many people dying every year,’ she told us. This primary care-based model seems to be the new way forward. ‘We would advise against isolating into suboxone ‘clinics’ and instead integrate this with primary care,’ Catherine Abrams said. Likewise is the sentiment from Dr. D’Orazio, ‘Primary care physicians are perfectly aligned with treating substance use disorder. They have all of the skills to manage it, and as long as we think about it as a chronic medical disease they are best equipped. Just look at how PCPs manage HIV now; that has been a big frameshift that we could apply to primary care similarly. There are also levels where it gets out of the realm of a PCP and has to go to a specialist the same as diabetes or cardiovascular disease.’
Harm Reduction and Community Support
MOUD is only one element of opioid use management, however, with a new focus shifting towards harm reduction as a more important principle to reduce human suffering. ‘When we talk about harm reduction, we mean reducing the risk for infection, transitioning from injection to other methods, clean needles, alcohol swabs. I have to say over the last decade physicians have become more comfortable with these conversations and realising that by having these discussions we are not condoning drug use but helping people in this situation,’ Dr. D’Orazio said. This is where non-medical groups in the community play a large role, not just in the Kensington area but throughout the city. Groups like Narcotics Anonymous, the Savage Sisters (who run several recovery houses and outreach events handing out hot meals, clean needles and wound care packs), Unity Recovery (who provide naloxone training and recovery counseling services), and Prevention Point Philadelphia (who started as a needle exchange service in the 1990s and now include homeless and behavioural health services as well as HIV, hepatitis, and PrEP clinics). ‘Our big objective has been to promote harm reduction strategies which have been missing for a long time. Access to adequate housing, prevention of peri-natal mortality, HIV transmission reduction, reducing streetside births and vertical transmission of syphilis, are all crucial elements in the fight,’ said Catherine Abrams.
Other medical outreach groups go directly into the community and bring the medical services there, although uptake tends to be more difficult long term. ‘These patients (treated by the mobile vans acutely) often get referred to City Heath for long-term care and follow up isn’t great, but sometimes just part of the cycle of recovery. If for every ten of these patients only one or two make it in, that’s okay’ Dr. Westerhaus told us.
Many Barriers Remain Systemic
Despite all of the progress, it’s clear that the problem continues to worsen with escalating rates of opioid-related mortality and morbidity and the reasons are multi-faceted. For one, the fragmented nature of US healthcare is such that it prevents one body from coordinating the effort in a large city like Philadelphia. ‘We have four different health systems all with different approaches to pain management and the treatment of addiction,’ Catherine Abrams told us. This patchwork also means that no single actor takes responsibility for gaps or deficiencies, as

12 Philadelphia Medicine : SPRING 2024 FEATURE continued philamedsoc.org
evidenced by the holes left from the closing of two large hospitals in the last decade. ‘Losing Hahnemann and the conversion of Mercy Hospital to the Penn network led to a big gap and new turbulence for many of these patients,’ Catherine Abrams said. Dr. Westerhaus agrees the system is not conducive to effective efforts. ‘The city is fairly disjointed with this’ she told us. ‘This is starting to get better now since it’s starting to be spearheaded more by the academic centers and they are starting to talk to each other a little bit more instead of saying ‘we do it this way and you do it that way’ trying to come up with a best practice. Then we have groups like Prevention Point who do a lot of work but aren’t necessarily tied to an academic center or the city.’ Likewise, at the level of the municipality, we have different structures engaged in different elements of addressing the crisis with no true central coordination to reduce redundancy, optimize, or even ensure congruence between them. ‘The City has an ambulatory health branch and also a public health branch involved in this, and at times they have difficulty staying abreast of what exactly the other one is doing,’ Dr. Westerhaus said.
One other barrier is that opioid use disorder requires patience and time investment from providers, and a lot of these principles of harm reduction are new age. ‘We simply don’t have enough providers in the city,’ she said. ‘Not every physician is in the know, and patients oftentimes have to get lucky for someone to open the door for them to get good care. Patients shouldn’t have to get lucky to get a provider on a given day that knows what to do for your problem and what direction to point you,’ Catherine Abrams said. This lack of provider comfort applies both in the hospital and in the clinic as Dr. Westerhaus pointed out. ‘Clinics aren’t forcing physicians to treat opioid use. The City Health Centers are a primary care service that provides MOUD to patients regardless of their insurance status as well as drug coverage assistance. They are not Suboxone clinics, so one of the caveats is that in order to get Suboxone with the City, they have to become your PCP. If a patient wants to keep their PCP but can’t MOUD from them, they are stuck. Part of the question over the last five to ten years is why, why aren’t people doing it? I think the biggest obstacle is time. Physicians just don’t have the time, you don’t have the luxury to spend 30 minutes with a patient every week.’ There is a large gap in number of providers willing to treat this condition and how many patients stand to benefit.
Also is the reality that fundamentally this is not a profitable disease to treat. The patients most in need of care are on Medicaid or uninsured. Patient outcomes are also generally fairly poor, especially when we consider days of stay as the benchmark for quality care. A patient that stays longer as an inpatient to start on MOUD or to see their medical problem appropriately treated before discharge winds up costing hospitals more. Dr. D’Orazio agrees. ‘Our health systems are not incentivized to provide good care for patients with substance abuse disorder. We create unnecessary barriers and the access to care is a high bar. If we had more providers, more access to outpatient clinics, or specialty training for ancillary staff within the hospitals things could be very different.’
Where can I start as a Physician in the City?
So where can the curious and motivated PCP go to learn about how to help the cause? Philadelphia Medicine Magazine compiled the following list of resources for both patients and providers:
For Physicians
• SAMHSA - federal group that lets you look up a provider that prescribes suboxone anywhere in the US. Also provide links for practitioners to be trained in suboxone prescription. https://www.samhsa.gov/
• UCSF clinical substance use warm line - if you are in a bind with a patient in front of you wanting to start care. https:// nccc.ucsf.edu/clinical-resources/substance-use-resources/
• Substance Use Response, Guidance, and Education (SURGE) – provide free training and support resources for physicians to start treating OUD with MOUD https://surge. healthfederation.org/
For Patients
• Care connect warmline - provides short prescriptions for substance use and is navigator to help patients estabilish care 484 278 1679 https://penncamp.org/get-help/
• Ophelia group - telemedicine suboxone https://ophelia. com
Active Non-profits:
• Savage Sisters - https://savagesisters.org/
• Unity Recovery - https://unityrecovery.org/
• Prevention Point - https://ppponline.org/ •
References
1. Health PDo. Unintentional Drug Overdose Fatalities in Philadelphia, 2022. 2023.
2. Prevention CfDCa. Understanding the Opioid Overdose Epidemic. 2023.
3. Booth M. Opium: A history: St. Martin’s Griffin; 2013.
4. Macy B. Dopesick: Dealers, doctors and the drug company that addicted America: Bloomsbury Publishing; 2018.
5. Alpert A, Evans WN, Lieber EMJ, Powell D. Origins of the Opioid Crisis and its Enduring Impacts*. The Quarterly Journal of Economics. 2021;137(2):1139-79.
6. Fauber J, Gabler E. Doctors with links to drug companies influence treatment guidelines. Milwaukee Journal Sentinel Retrieved February. 2012;21:2022.
7. Office USGA. Prescription drugs OxyContin abuse and diversion and efforts to address the problem: report to congressional requesters: DIANE Publishing; 2003.
8. Delouya S. SCOTUS to scrutinize controversial opioid crisis settlement that would give Sackler family immunity. ABC7 Chicago. 2023.
9. Muhuri PK, Gfroerer JC, Davies MC. CBHSQ data review. Center for Behavioral Health Statistics and Quality, SAMHSA. 2013;1:17.
10. Pergolizzi Jr J, Raffa R, LeQuang JAK, Breve F, Varrassi G. Old Drugs and New Challenges: A Narrative Review of Nitazenes. Cureus. 2023;15(6).
philamedsoc.org SPRING 2024 : Philadelphia Medicine 13
Pitt Drops A Bombshell THE PA HEALTH AND ENVIRONMENT STUDIES ON FRACKING

 By Dr. Ned Ketyer, President, Physicians for Social Responsibility Pennsylvania
By Dr. Ned Ketyer, President, Physicians for Social Responsibility Pennsylvania
14 Philadelphia Medicine : SPRING 2024
philamedsoc.org FEATURE

Since the fracking boom began in Pennsylvania 20 years ago, a large and growing body of public health and scientific data has been collected showing unequivocally that unconventional shale gas development (horizontal drilling, high volume/high pressure hydraulic fracturing or “fracking”) threatens the health and safety of people who live and work near well pads, compressor stations, pipelines, processing facilities, and other natural gas infrastructure. The closer residents live to fracking operations, the research tells us, the greater the risk of harm. Residents who are most vulnerable to health damage from fracking include pregnant women, infants and children, the elderly, people living in poor and marginalized communities, and people suffering from chronic medical conditions.
None of this, of course, should be surprising. Although fracking has been going on in the commonwealth for two decades, drilling for oil and gas has been inherently dangerous since Drake drilled the first conventional (vertical) oil well in Titusville, PA 164 years ago. It is now well-established that fracking degrades the environment and pollutes the air, water, and soil we all share, in violation of Article 1 Section 27 of the PA Constitution guaranteeing the right to clean air, pure water, and the preservation of a safe environment for all Pennsylvanians, present and future. It is also undeniable that fracking pours greenhouse gases into the atmosphere and accelerates climate change. And we know that fracking makes people who live near it sick.
In May 2019, David Templeton and Don Hopey published
“The Human Toll” in the Pittsburgh Post-Gazette, uncovering 27 cases of Ewing sarcoma — a very rare and frequently fatal bone cancer of childhood — and 40 cases of other rare cancers, for a total of 67 rare cancers in children, teenagers, and young adults living in four heavily fracked counties in Southwestern PA between 2008-2018 (Washington, Westmoreland, Greene, and Fayette).
Only about 200 cases of Ewing sarcoma are diagnosed in the United States each year. In Washington County, Pennsylvania’s most heavily fracked county (where I live and work), six cases of Ewing sarcoma and 30 other rare childhood cancers were counted. These numbers are far more than would be expected to occur in a similarly populated, mostly rural area over a 10-year period, and new cases keep popping up. Parents and pediatricians like me are very concerned that pollution and toxic waste from shale gas operations may be to blame for this outbreak of rare childhood cancers.
Six months after “The Human Toll” was published, I had the chance to travel to the Statehouse along with dozens of community members whose health had been impacted by fracking. We spoke with then-Governor Tom Wolf and other lawmakers and demanded a thorough and transparent investigation into the causes of these rare pediatric cancers. Four days after our visit, Gov. Wolf announced the creation of three studies to be conducted by the Pennsylvania Department of Health and the University of Pittsburgh Graduate School of Public Health. Two studies examined health impacts in heavily fracked
continued on next page
15 SPRING 2024 : Philadelphia Medicine philamedsoc.org
Pitt Drops A Bombshell: The PA Health and Environment Studies on Fracking continued from page 15

counties in southwestern Pennsylvania on birth outcomes and asthma, and the third study examined the plausible link between fracking and some of those rare childhood cancers.
On August 15, 2023 — nearly four years after the studies were promised — University of Pittsburgh researchers and staff from PADOH announced the results. Unsuprisingly, the results mirrored dozens of other epidemiological research, hundreds of other medical and scientific peer-reviewed studies, and hundreds more government reports and media investigations contained in the latest edition of the Compendium of Scientific, Medical, and Media Findings Demonstrating Risks and Harms of Fracking and Associated Gas and Oil Infrastructure, showing the damaging impacts of fracking on human health, on the environment, and on the planet’s climate system.
For the asthma study, the researchers evaluated children and adults diagnosed with asthma using the University of Pittsburgh Medical Center (UPMC) electronic medical records from 20112020. They discovered that asthmatics living in southwestern Pennsylvania within 10 miles of one or more unconventional gas well had 4-5 times the risk for having a severe asthma attack, being seen in the ED, or needing hospitalization to treat their asthma attack compared to people living more than 10 miles away. The biggest association was seen not during the well’s construction, which may take a few weeks, or during the drilling and fracking phase, which takes several weeks or a few months. The biggest risk was later, during the production phase, when gas is flowing out of
the well to the surface. The production phase lasts for many years, even decades, after the drilling and hydraulic fracturing of the shale is completed. So even if fracking were to stop tomorrow, the threat won’t stop.
In Washington County, no one lives more than 10 miles away from a fracking well. Most of us live much closer to wells, but also pipelines, compressors, processing facilities, landfills where toxic and radioactive fracking waste is dumped, and all the diesel emissions resulting from fracking activities.
For the cancer study, the researchers examined the PA DOH Cancer Registry between 2010 and 2019. They looked only at 4 types of cancer in children — leukemia, lymphoma, brain and CNS tumors, and bone tumors like Ewing sarcoma — and found 498 cases in the 8-county area of SWPA. The study found that children living within 1 mile from one or more fracked gas wells had 5-7 times the risk of developing lymphoma compared to kids living more than 5 miles away. While a 2022 study from Yale University found a 2-3 times higher risk of acute lymphoblastic leukemia in children living within 2 km of a fracked well in Pennsylvania, the Pitt researchers found no link to leukemia, to brain/central nervous system tumors, or to bone cancers like Ewing sarcoma.
The birth outcome study used the PA DOH Birth Registry data of more than 185,000 births in the 8-county area of southwestern PA from 2010-2020. They found associations between living up to 10 miles from fracked wells and low
FEATURE continued philamedsoc.org
16 Philadelphia Medicine : SPRING 2024
birthweight and small for gestational age (SGA). They also found the well-known association of prematurity as a result of exposure to PM 2.5 during pregnancy from any source (not just fracking) in SW PA. Again, the risk of abnormal birth outcomes was seen up to 10 miles from fracked wells. The well site preparation phase and the production phase, which can last for decades, was associated with the greatest risk.
What the Pitt studies tell us with certainty confirms what we’ve already learned from prior research: There is something about fracking that increases the risk of developing health problems for people living and working nearby. We also know quite clearly that the closer you live and work to fracking operations — to well pads, pipelines, compressor stations, gas processing facilities, and landfills that accept fracking waste — the higher the risk of developing health problems. And we now know that something related to fracking interferes with normal fetal growth.
The studies don’t tell us with certainty what exactly is causing those health problems, though it isn’t hard to speculate that endocrine-disrupting chemicals and other toxics used by the shale gas industry could be the culprit for poor birth outcomes. Perhaps volatile organic compounds released during shale gas operations contaminating the air and water — like benzene, a carcinogen, or toluene, a neurotoxin causing permanent nerve damage — or heavy metals and radioactivity brought up from the Marcellus Shale to the surface are what is causing health symptoms in people exposed to fracking pollution. Maybe it’s the stress that residents in Pennsylvania’s gas patch live under; the studies don’t tell us with any certainty.
But that level of certainty isn’t required for doctors to begin taking steps to prevent harm to their patients. And absolute certainty isn’t required for Gov. Josh Shapiro and the PA legislature to finally adopt health-protective policies to prevent further harm to our health, to our land and water and air, and to Earth’s climate. Enough studies have been done about the health impacts caused by fracking. Now it’s time for action. •
About the Author: Dr. Ned Ketyer is President of Physicians for Social Responsibility Pennsylvania. He served on the External Advisory Board for the University of Pittsburgh health studies on fracking. Dr. Ketyer is a member of the American Academy of Pediatrics Council on Environmental Health and Climate Change and medical advisor to Environmental Health Project.
A Continuing Medical Education Program
Saturday, April 27, 2024
8:00 AM - 12:30 PM
Program Director:
Harvey B. Lefton, MD, FACP, FACG, AGAF, FASGE, past President, PCMS 2023 Recipient of the PA Society of Gastroenterology Lifetime Achievement Award
You’re invited to hear Philly’s Top Docs discuss the latest in the field of Gastroenterology! This is a free educational program and everyone including the general public is welcome to attend. The program is recommended for physicians, residents/fellows, medical students, nurses, physician assistants, psychologists and allied health care professionals and will be held as a Zoom video conference.
Topics to be discussed:
• Managing GERD in 2024
• 2024 Update in Advanced IBD Therapeutics
• What’s New in Liver Disease
• Update on Irritable Bowel Syndrome
RSVP Here!
https://philamedsoc.org/pcms-events/the13th-annual-clinical-update-in-gastroenterology/
Registration is required. No fee to attend. Program will be held as a Zoom video conference.
ACCREDITATION
This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of the Pennsylvania Medical Society and The Philadelphia County Medical Society. The Pennsylvania Medical Society is accredited by the ACCME to provide continuing medical education for physicians.
The Pennsylvania Medical Society designates this live activity for a maximum of 4.25 AMA PRA Category 1 Credits™. Physicians should only claim the credit commensurate with the extent of their participation in the activity.
philamedsoc.org 17 SPRING 2024 : Philadelphia Medicine

Physicians’ Corner
Measles Outbreak in Philadelphia Continues
For the latest updates visit: https://bit.ly/Measles2024PHL
Measles is a dangerous virus, especially for babies and young children. It is spread through the air when someone who has measles coughs, sneezes, talks or even just breathes. Germs can stay in a room for two hours after someone with measles has left. Fortunately, Philadelphia has high community immunity. At least 93% of children are fully vaccinated against measles by age 6. However, about 90% of unvaccinated people who have close contact with an infected person will get measles. Children younger than 5 years of age and adults older than 20 years of age are more likely to suffer from complications. Measles spreads more easily than other respiratory viruses. You can get infected and pass measles on to other people even before you have a rash. This is why it is so important to remind anyone who thinks they have been exposed to stay home and contact their healthcare provider for next steps. PDPH strongly recommends anyone who may have been exposed to measles should quarantine themselves by staying home and away from others and contact their health provider to find out next steps.
Philadelphia locations and exposure dates are updated here: https://bit.ly/Measles2024PHL
• Please check the list in this link to see if you have been exposed.
• Use this link to learn if you are immune to measles, to
find the measles vaccine (MMR) and receive updates on this response in real time.
• Flyer attached here: http://tinyurl.com/5n8ebvtb
UPHS and Doylestown Health Plan Merger
The University of Pennsylvania Health System and Doylestown Health are pursuing a merger. The health systems announced in early January 2024 that they have signed a letter of intent under which Doylestown Health, parent company of Doylestown Hospital in Bucks County and one of the region’s last independent community hospital operators, will become part of Penn Medicine. Doylestown Health, like most health systems in the region, has struggled financially due to rising expenses for supplies and the ongoing labor shortage. The merger process is expected to take most of the year to complete. The next step is for the organizations to complete their due diligence and sign a definitive agreement before submitting it to the appropriate federal and state regulators for approval.
State Lawmakers Introduce Moratorium and Study on For-Profit Hospital Ownership
Lawmakers in Harrisburg hope to address the issue of high health care costs by understanding the impacts the recent increase in for-profit hospital ownership has had in Pennsylvania. In early
18 Philadelphia Medicine : SPRING 2024
philamedsoc.org FEATURE
January, they introduced legislation to establish a moratorium for 24 months on the transfer of ownership of a hospital or health system in Pennsylvania if the acquiree or the acquirer is a forprofit entity. It directs the Joint State Government Commission to study for-profit hospital and health system ownership, including the causes for the increase in for-profit ownership and the costs/ benefits of for-profit versus non-profit ownership. If passed into law, a moratorium on approvals of new for-profit hospitals will give legislators the time needed to conduct a comprehensive review of for-profit hospitals and their impact on health care in the state.
Another Orphan Residents program
Crozer-Chester Medical Center’s surgical residency program’s accreditation has been removed by the Accreditation Council for Graduate Medical Education (ACGME), with the program needing to close by Jan. 12, 2024. This residency program, which had 15 filled resident positions, has been withdrawn “under special circumstances” on ACGME’s website, acgme.org. ACGME’s policies and procedures list states that its review committee can withdraw a sponsoring institution or program’s accreditation in the event of “a catastrophic loss of resources, including faculty members, facilities, or funding” or “egregious non-compliance with accreditation requirements.”
Crozer was notified by the ACGME that their surgical residency program needed to close by Friday, January 12. The Fall 2019 closure of Hahnemann University Hospital left more than 550 residents and fellows without a program accredited by the ACGME. All residents and fellows from every specialty at Hahnemann had to scatter across the country to find new programs within the span of a month. Many of these residents and fellows had to pay exorbitant fees to break their leases, while extending their residency training to prove themselves again to another institution.
PCMS Announces Annual Awards Program
Know a Philadelphia colleague or mentor that deserves to be recognized. Nominations are now open for:
• The Strittmatter Award
• Practitioner of the Year Award
• Vanitha Appadorai Vaidya, MD Award for Humaneness in Medicine
• Cristol Award
Awardees will be honored by PCMS during the formal Presidents Installation event in early June 2024. It’s a great way to say “Thank you!” Won’t you please nominate a colleague today? Deadline is March 4.
Membership
It’s time to renew your PCMS/PAMED membership! Renew now to maintain access to great member benefits like our License Resource Center. www.pamedsoc.org/PayMyBill. Thanks also to everyone that has already renewed.
PA Legislation on Consent for Examinations
The law requires health care providers overseeing or participating in professional instruction or clinical education to obtain specific informed consent prior to performing a pelvic, rectal, or prostate examination on a patient who is anesthetized or unconscious. The requirement for specific informed consent does not apply if the examination is within the scope of care ordered for the patient or is necessary in the case of a medical emergency. The law was effective beginning January 21, 2024.
What’s next at the Doctors’ Lounge?
Master of Business Administration (MBA) is one of the most popular graduation-level programs in the world. This degree certainly enhances the business knowledge and managerial skills. However, an MBA also has its own advantages and disadvantages. Physicians are sometimes interested in pursuing a formal business education for a whole host of reasons like the desire to effect change within their organizations or even health care delivery as a whole. For others, an MBA or Master of Medical Management degree (MMM), or the Certified Physician Executive (CPE) credential, is viewed as a way to better position themselves as credible participants in big-picture discussions about organizational direction or in decisions that affect their professional lives or their specialty’s future.
Please joins PCMS & CPP for our second Doctors’ Lounge on Thursday, Feb 8 at 6:00 PM for a panel discussion on: “How to Improve Your Business Skills in Healthcare without obtaining an MBA.” https://13284a.blackbaudhosting. com/13284a/Doctors-Lounge-How-to-Improve-Your-BusinessStrategy-Without-an-MBA •
19 SPRING 2024 : Philadelphia Medicine philamedsoc.org

NEGOTIATING KEY EMPLOYMENT CONTRACT TERMS
By Karen E. Davidson, Esq.

Physician employment contracts encompass relationships between doctors and savvy hospitals/health systems, academic medical centers and private practices. These contracts have evolved into sophisticated instruments drafted principally for the benefit of the employer. They specify the duties and obligations of the physician (from clinical hours to on-call duties), outline compensation, address professional liability insurance coverage, and delineate termination rights. This article seeks to raise awareness of four key contract areas and highlight some related negotiation tips.1
1. Compensation.
While physician compensation historically was a set amount with annual increases, changes in reimbursement and the health care marketplace have vastly increased compensation complexity, often shifting risk to physicians. What exists now are elaborate compensation models that typically provide guaranteed base compensation for one or two years, after which the base and/ or bonus is subject to incentives and productivity benchmarks. These include work relative value units (wRVUs) (a measure of physician work effort) or collections, quality measures and others that serve as targets to determine if a physician will retain, lose or garner certain compensation. Anticipated compensation should be analyzed based on a specialty’s compensation survey data (available through subscription). Physicians should fully understand their compensation/incentive targets, ascertain if they are likely to achieve them and estimate the amount or range of compensation to which they ultimately will be entitled.
Negotiation Tip: Seek to negotiate compensation that is definitive for as long as possible through set compensation with specified bonus amounts including perhaps sign-on or retention bonuses, with set increases, whether established amounts or
percentages. For variable portions of compensation (such as floating base or productivity bonuses) seek lower target thresholds for wRVUs or collections, and greater wRVU dollar values based on compensation survey data.
2. Professional Liability Insurance.
Most physician contracts specify that the employer will purchase professional liability insurance covering the physician for services rendered during the period of employment. They should also address which party is responsible for purchasing a post-termination extended reporting endorsement (i.e., tail coverage) if the underlying policy was written on a “claims made” basis. Absent an express obligation by an employer to purchase tail coverage, physicians are generally liable for the cost. It is critical that the contract clearly specifies the party responsible for tail coverage cost and the circumstances under which such party will assume tail responsibility. It has become increasingly important to ascertain if there is any limit on the extent of tail coverage. This is because some employers limit tail coverage to the applicable statute of limitation period, leaving the physician open to potential future liability.
Tail coverage is expensive, ranging from 100% to 200% of a physician’s annual professional liability premium. The cost can be exorbitant for high risk specialties with costly annual premiums. For example, an OB/GYN physician’s tail coverage could cost upwards of $80,000 during the first year of medical practice. Regardless of the tail arrangement, the physician should fully understand the extent of tail coverage liability he/she could be obligated to assume.
Negotiation Tip: Negotiating tail contract provisions can be tricky because who pays the tail may depend on the type of termination. Ascertain if the employer will assume the full cost of unlimited tail coverage upon termination regardless of the termination reason. If that is not possible, consider seeking to
20 Philadelphia Medicine : SPRING 2024
FEATURE philamedsoc.org
have the employer assume the full tail coverage cost if it terminates the contract “without cause” or if the physician terminates “for cause.” Alternatively, it may make sense simply to seek a cap on the physician’s tail obligation amount or propose that the parties share the cost equally.
3. Term/Termination.
Physicians are often told by prospective employers that they are being offered a multi-year contract. Yet, the contracts often allow the parties to terminate for any reason (i.e., without cause) at any time upon relatively short notice (e.g., 60 or 90 days). Contracts also typically include “for cause” termination provisions allowing an employer to immediately terminate due to acute circumstances such as loss of licensure or professional liability coverage, or contract breach. These provisions can be based on subjective factors and drafted too broadly, so should be carefully reviewed.
When assessing the impact of termination provisions, physicians should ascertain what the fall-out will be under “without cause” and “for cause” circumstances. That is, under what termination circumstances might the physician be liable for tail coverage (discussed above), be obligated to repay a sign-on bonus, moving expenses, educational loan amounts or other items, or lose a productivity, quality or other bonus or compensation. Note that a physician may only be entitled to certain incentive compensation payments if he/she is employed at the time of payment, which is often many months after it is earned. Bottom line, physicians should try to limit such losses and repayments as much as possible.
Negotiation Tip: Ascertain if it makes sense to seek a “no cut” deal where neither party has the right to terminate the contract “without cause” for 1 or 2 years. Doing so may limit the need to repay certain items. Also, if a significant obligation (such as tail cost) is triggered by a “for cause” termination, try to negotiate objective, narrow “for cause” provisions. Physicians should also seek to reduce repayment obligations by negotiating burn-offs that gradually reduce repayment amounts over the course of one or two years.
4. Non-Compete Clauses.
Non-compete clauses typically limit physicians from practicing within certain geographic areas (often based on a mileage radius around a location or multiple sites) for a specified time-period following contract termination. Most states uphold non-compete restrictions that legitimately protect an employer from unfair competition and that are reasonable in geographic area and time. Time restrictions of one to two years are usually upheld as reasonable. Reasonableness of mileage restrictions may depend on whether the employer is in an urban, suburban or rural area. For example, a 10-mile non-compete may be reasonable in a suburban locale, but unreasonable in the heart of a city. Note that a Spring 2024 Federal Trade Commission vote is anticipated on its proposed rule banning non-competes; however, such a ban is not
expected to apply to non-profit entities/organizations.
In the meantime, physicians should carefully analyze noncompete restrictions and ascertain all locations from which a mileage restriction applies. Online distance calculator tools can facilitate examination of an anticipated restricted area. If a restricted area is extensive and applies to several of an employer’s sites or locations, the physician should ascertain if he/she will have to relocate upon termination of employment.
Physicians need to understand the extent of the non-compete restriction(s) and determine where they could work if subject to the non-compete. Some contracts contain remedies for noncompete violations including liquidated damages which can be a multiple of the physician’s annual compensation. For physicians leaving a position which is subject to a non-compete restriction, care must be taken to ensure that any new position will not be violative. Ultimately, physicians should not sign a non-compete with which they do not intend to comply.
Negotiation Tip: Seek to limit a non-compete to locations where the physician renders services for the employer. This may entail a further limitation if the physician covers multiple locations, perhaps limited to the location where the physician primarily renders services but delineated with as much specificity as possible. If there are realistic future employment opportunities within certain geographic areas, try to reduce the mileage or negotiate zip-code or institution carve-outs where the physician might seek employment after termination.
Summary
Physician employment contracts are sophisticated instruments with potential for significant adverse impact on physicians. They should be carefully analyzed and negotiated to limit physicians’ exposure to financial loss and other liability. •
About the Author: Karen E. Davidson, Esq., managing member of Law Offices of Karen E. Davidson, LLC, is a veteran attorney focused on representing health care professionals. She has over 30 years’ experience serving the legal needs of her clients in business, regulatory and reimbursement matters. Ms. Davidson is a graduate of Temple University – James E. Beasley School of Law, licensed to practice law in the Commonwealth of Pennsylvania, State of Maine and the District of Columbia (inactive), and a member of the Bar Associations in those jurisdictions. She is also a member of the American Health Law Association and Board of Directors of Southeastern Pennsylvania Area Health Education Center. Ms. Davidson speaks regularly to professional groups providing insight into legal issues in professional practice. She can be reached by telephone at (610) 940-4041 or email at karend@ kdavidsonlaw.com, or through www.kdavidsonlaw.com website.
1 This article is solely for informational purposes and does not constitute legal advice. The advice of a qualified attorney should be sought in connection with review, interpretation and negotiation of any employment contract.
21 SPRING 2024 : Philadelphia Medicine philamedsoc.org

Communities Join to Tackle Medical Debt in Pennsylvania
By Jessy Foster, Deputy Director of Policy and Partnerships Pennsylvania Health Access Network
Medical debt is not rare. A trip to the emergency room for a car accident or medical crisis, a planned surgery, or even the birth of a child can mean hundreds to thousands in unexpected medical bills that most Pennsylvanians simply can’t afford to pay, leading to widespread medical debt. Moreover, medical debt can present in ways beyond a hospital collections bill. According to a 2023 study by Altarum1, 1 in 3 Pennsylvanians are struggling to pay their medical bills, reporting that they were reported to a collections agency (15%), used up all or most of their savings (11%), had to sacrifice paying for basic necessities like food, heat or housing (11%), racked up large amounts of credit card debt (9%), borrowed money, took out a loan, or got another mortgage on their house (8%), or were placed on a payment plan (7%).
According to the same study, 1 in 4 reported having bills that are overdue (i.e. they are in medical debt). Since 2015, the costs of seeking hospital-based care have increased as much as 31% nationally, growing more than four times faster than most workers’ paychecks2. A Kaiser Family Foundation report3 found that 1 in 7 people with medical debt said they’ve been denied access to a hospital, doctor, or other provider because of unpaid bills.
This means the levels of medical debt are very high, and many who aren’t in debt are achieving that by forgoing basic necessities, taking out loans or second mortgages, or using up their savings. At the Pennsylvania Health Access Network (PHAN), we have been talking with people from across the state over the last year about their experiences accessing healthcare, and how medical debt has impacted them. Through petitions, surveys, focus groups, and one-on-one conversations, many Pennsylvanians shared with us examples of the financial and health impacts on their lives.
Seniors shared that because of a medical expense in years prior, their retirement savings were wiped out, forcing them to continue working despite their age and declining health. Other
families noted that even though they are insured, high deductible plans with high copays mean they are still left to shoulder most of the bill, meaning thousands in out-of-pocket costs. Patients are forced to choose whether or not to pursue recommended care, some sharing how they put off care for years out of fear they would get a medical bill they could not afford, and now face the long-term impacts to their health and well-being as conditions have deteriorated. Despite the availability of financial assistance programs directly from hospitals, few patients report any knowledge about these programs. Often, patients are instead referred to long-term payment plans, that do not take into account limited fixed incomes or ongoing health needs. Lack of information about resources was even greater among immigrant and limited-English-proficient communities.
In September, PHAN joined national partners for a Day of Action in Washington DC where patients shared their personal stories directly with members of the Biden Administration. Shortly after, we have seen federal policymakers begin to take action. The Biden Administration announced support for the Consumer Financial Protection Bureau, which has launched a new rulemaking process to prevent medical debt from impacting credit scores4. Their proposal would help remove medical bills from consumers’ credit reports, stop creditors from relying on medical bills for underwriting decisions, and stop coercive collection practices.
While this is a great first step, we continue to push for state level measures. Medical debt can be prevented before a patient ever receives a medical bill, and the programs to prevent medical debt already exist. The vast majority (91%) of Pennsylvania hospitals are tax-exempt, and therefore required by law to create and publicize financial assistance programs that provide free or discounted care to eligible patients. Yet, many patients are not aware of these programs, meaning that the bills they receive for medical care do not reflect the discounts they should receive. HB78 would provide relief and reduce predatory practices by
Politics & Medicine 22 Philadelphia Medicine : SPRING 2024 philamedsoc.org FEATURE

collection agencies for Pennsylvanians already experiencing medical debt. More importantly, it will prevent medical debt altogether by
• Creating a single, uniform application for financial assistance
• Screening more people for eligibility for health coverage
• Providing information about available financial assistance and coverage in an easy to understand format
• Requiring clear, direct notices right on bills that assistance is available
HB78 passed the PA House twice on a bipartisan basis, once as a standalone bill and once as part of the fiscal code bill, HB1300. At the time this article is
being written, we are disappointed to say the language was not included in the budget code bill passed by the Senate, but the fight does not stop here. We will continue to advocate for these commonsense patient protections through the stand-alone version of the bill and the governor’s budget address in the new year. We continue to hear from Pennsylvanians about their experiences and will seek to monitor enforcement and additional patient protections.
PHAN has created a petition for physicians and healthcare providers to sign on to show support for action on medical debt and share anecdotes about how they have seen medical debt impact their patients’ lives, to show policymakers the need for meaningful change: https://pahealth.salsalabs.
org/hb78providersignon. If you have questions or want to get involved in PHAN’s work to prevent medical debt, reach out to jessica@pahealthaccess.org. •
1 Altarum Healthcare Value Hub: Pennsylvania Survey Respondents Struggle to Afford High Health Care Costs; Worry about Affording Health Care in the Future; Support Government Action Across Party Lines
2 Families USA: Bleeding Americans Dry: The Role of Big Hospital Corporations in Driving Our Nation’s Health Care Affordability and Quality Crisis
3 Kaiser Family Foundation: Health Care Debt In the US: The Broad Consequences of Medical and Dental Bills
4 Consumer Finance Protection Bureau: CFPB Kicks Off Rulemaking to Remove Medical Bills from Credit Reports
23 SPRING 2024 : Philadelphia Medicine philamedsoc.org

Edith P. Mitchell, health-care
trailblazer, civil rights pioneer, and retired Air Force brigadier general,
has died at
76
Dr. Mitchell became president of the National Medical Association in 2015.Tom Gralish / Staff Photographer
by Gary Miles, Philadelphia Inquire
Published Feb. 2, 2024
Obituary Highlights by William King, MD, PCMS Boardmember
The first female physician to become a brigadier general in the Air Force, she transformed care for disadvantaged cancer patients at Thomas Jefferson University and elsewhere around the country.
Edith P. Mitchell, 76, of Newtown Square, longtime physician, professor, and program director at Thomas Jefferson University, civil rights pioneer, and retired Air Force brigadier general, died Sunday, Jan. 21, at Mercy Fitzgerald Hospital in Darby. The cause of her death has not been disclosed.
Called a “woman before her time” and a “monumental contributor” to cancer and gastrointestinal research and treatment by colleagues, Dr. Mitchell was also a trailblazing champion for minority health care providers and medically underserved communities in the United States. She evaluated hundreds of new drugs and treatment procedures over her 50-year career in medicine, was a mentor to many, and, closest to her heart, dug deep to understand how disadvantaged patients could be better served.
“We all know that there is not racial equality in this country,” she told The Inquirer in 2015, “and the lack of racial equality extends into health care.”
Dr. Mitchell joined Jefferson in 1995 and served as clinical
professor of medicine and medical oncology at the Sidney Kimmel Medical College, and director of the Center to Eliminate Cancer Disparities at the Sidney Kimmel Cancer Center. She was known for her humility, wit, compassion, and dedication as well as her medical achievements, and colleagues at Jefferson said in a tribute: “Dr. Mitchell’s impact will continue to be seen and known for generations to come.”
Julia A. Haller, chair of the board of trustees of the College of Physicians of Philadelphia, noted Dr. Mitchell’s “commanding intellect, integrity, and commitment to our country, our profession, and our society.” Robert Winn, director of the Massey Comprehensive Cancer Center at Virginia Commonwealth University, said in an online tribute that she “created a model for a life worth living and inspired us all.”
Dr. Mitchell was past president of the National Medical Association and active with the American Cancer Society, National Institutes of Health, Royal College of Physicians in London, and many other organizations. She earned Jefferson’s 2018 Achievement in Medicine Award and the Pennsylvania Medical Society’s 2023 Distinguished Service Award.
Last year, a worldwide group of cancer research centers renamed its awards for minority trainees the Edith Peterson
24 Philadelphia Medicine : SPRING 2024 FEATURE philamedsoc.org
Mitchell Health Equity Travel Scholarships.
“We don’t use a one-shoe-fits-all theory. All the factors that are social determinants of health have to be addressed.” — Edith P. Mitchell in 2018 on how to improve health care in disadvantaged communities.
Dr. Mitchell enlisted in the Air Force in 1973, became certified in aerospace medicine, and served as a flight surgeon and in other roles during her more than three decades of active and reserve duty. She graduated from the Air War College in 1995 and became the first female physician to attain the Air Force rank of brigadier general in 2001.
She earned more than a dozen medals and ribbons during her time in the service, and worked often later with the Veterans Affairs Hospital in Philadelphia.

Dr. Mitchell and her husband, Delmar, were married for 52 years.Courtesy of the family
Featured many times in The Inquirer, Daily News, and other publications, Dr. Mitchell published more than 100 scholarly articles and book chapters about all sorts of medical subjects, and she spoke often about the inequities that scar the modern medical landscape.
“Most schools in the United States only admit a few underrepresented minorities a year,” she said in 2023. “We’ve got to increase the number of underrepresented individuals in medicine.”
Edith Faye Peterson was born Nov. 20, 1947, in Brownsville, Tenn. She graduated high school as valedictorian, and a local Black doctor who treated her family when white doctors would not inspired her to pursue a career in medicine.
She earned a bachelor’s degree in biochemistry at Tennessee State University in 1969 and a medical degree from the Medical College of Virginia, now Virginia Commonwealth University School of Medicine, in 1974. She met fellow student Delmar Mitchell at Tennessee State, and they married in 1969, and had daughters Dale and DeAnna. Her husband died in 2021.
Before Jefferson, Dr. Mitchell won a 1991 Distinguished Service Award as a professor of medicine at the University of Missouri and was stationed at Air Force bases and hospitals in Maryland, Washington, California, Missouri, and Illinois.
She was an engaging storyteller by all accounts and a celebrated member of Alpha Kappa Alpha Sorority. She liked to travel when she wasn’t working and tended her vegetable and flower gardens in Newtown Square to unwind.
She listened to jazz music, broke into dance whenever she heard “Shotgun” by Junior Walker and the All Stars, and tuned in as often as she could to watch Dallas on TV. “You have to do things to relax in your life,” she told The Inquirer.
Her daughter DeAnna said: “When she came into a room, she owned it. For many people, she was a superhero, a rock star. For me, she was a nurturer and the voice of reason. No matter where she was or what she was doing, I had her attention. For me, she was just mom.”

Dr. Mitchell (right) always made time for her family. Courtesy of the family
In addition to her daughters, Dr. Mitchell is survived by four grandchildren, a sister, and other relatives. Four sisters and a brother died earlier. •
25 SPRING 2024 : Philadelphia Medicine philamedsoc.org
This is Your Lane Growing Coalition of Physicians Takes On Gun Violence
By Adam Garber, Executive Director of CeaseFirePA Education Fund
It was November of 2018. In response to a new position paper by the American College of Physicians outlining a public health approach to preventing firearm deaths and injuries, the National Rifle Association scolded doctors to “stay in their lane.”
Maybe you remember what happened next.
An outpouring of frustration and exhaustion from physicians made clear that “this is our lane.” They started a movement that continues to grow five years later.
The toll of gun violence on our society is staggering. But as a healthcare provider, you see the impact much more up-close than most.
The emergency physician stabilizing a gunshot victim who’s about to bleed out. The surgeon sewing up a bullet wound. The psychiatrist tending to the mental trauma of a non-fatal shooting victim. The pediatrician counseling gun-owning parents about secure storage. The physiatrist rehabilitating a patient who lost the ability to walk.
Or the perfectly understandable, ever-present fear of workplace violence – already acute in healthcare settings – worsened by the growing ubiquity of firearms. Like the retaliatory incident last summer where over 50 shots were fired at three people standing

directly in front of Temple University Hospital’s ER. You could hardly be blamed for wondering: “could I end up being a gunshot wound patient myself?”
This epidemic is personal to you and the patients you are dedicated to healing. This is your lane.
And you also have a unique level of credibility and trust that makes your voice especially powerful in the public discussion about how we can drive down the incidence of gun violence and make our communities safer and healthier.
That’s why CeaseFirePA Education Fund, the Commonwealth’s leading gun violence prevention organization, is partnering with medical professional organizations, hospitals, and public health institutions across Pennsylvania to foster a space where healthcare providers can come together to educate the public and policymakers, and advocate for systemic change through a public health lens. We’re helping to lay the foundation and chart the course for “your lane” to lead to tangible changes in the public’s understanding of the gun violence crisis, and concrete reforms in Harrisburg that save lives and mitigate harm.
The Crisis
Gun violence is a public health crisis. We hear that said all the time. But what does it really mean?
It’s simple: we should use an empirical approach to understanding the drivers of firearm injury and death at a population-level, and then marshal the best evidence available to design and enact systemic, upstream reforms that address these causes and prevent harm and mortality.
And the harm is massive and widespread.
Gun violence took the lives of more than 1,900 Pennsylvanians in 2022, the latest year for which complete data is available. Another 3,500 survived a gunshot, but suffer physical, psychological, and emotional trauma. For context, this level of death and injury is roughly equivalent to the number of people who die from kidney disease and flu/pneumonia combined each year in Pennsylvania.
26 Philadelphia Medicine : SPRING 2024 FEATURE philamedsoc.org
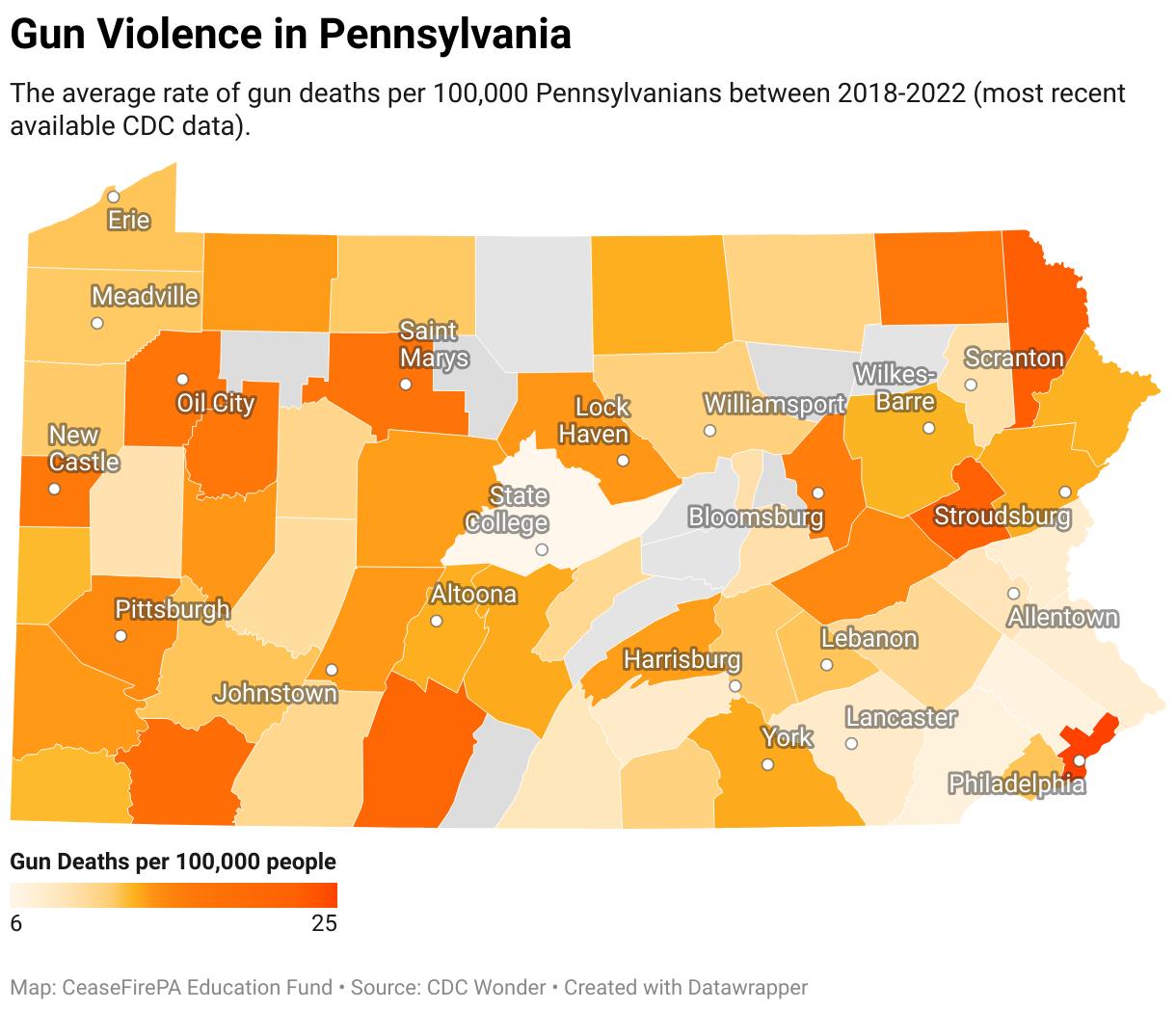
No part of our Commonwealth is left unscathed.
Contrary to popular understanding, the majority of gun deaths in Pennsylvania are suicides. This “silent killer” (compared to the high-profile nature of other gun deaths) disproportionately impacts rural counties, which on average have a 37% higher firearm death rate than urban counties.
The toll of firearm suicide also has a disproportionate impact on rural children, who are four times more likely to die by gun suicide compared to children in urban areas.
More broadly, gun violence poses a direct threat to the health and wellbeing of kids everywhere. In 2020, firearms became the top cause of death for children and teenagers in the United States, overtaking car accidents, according to the American Academy of Pediatrics. This is especially visible in unintentional shootings, which every year kill one-two dozen Pennsylanians – often children who access unsecured weapons that are improperly stored by irresponsible gun-owning adults.
And of course, community-based gun violence ravages Pennsylvania’s cities, with the impact concentrated among Black and Brown communities. Due to a confluence of social determinants of health, Black Pennsylvanians are 21 times more likely to be killed with a gun than white Pennsylvanians. Every shooting has second-order effects: children living near a shooting are twice as likely to visit an Emergency Room for mental health concerns.
Over 800 Pennsylvanians of all ages and backgrounds died from this type of community-based gun violence in 2022. And while 2023 did bring a 21% reduction in Philadelphia’s gun homicides, the impact on public health is still far too severe.
Mass shootings, while statistically much less common than community-based violence or gun suicide, are an especially visceral symbol of the constant feeling of unease that Pennsylvanians have now sadly become enured to. The recent shooting at a SEPTA bus stop that injured eight has reignited fears that violence can hit anywhere, at any time. Pennsylvania averages roughly 10 mass shootings per year, defining mass shootings as four or more people injured or killed, not including the shooter. The inability to go to

the store or send your kids to school without the nagging fear of mass violence is an indication that health and safety systems are not working.
And finally, domestic violence is a threat in every community across Pennsylvania, made significantly worse by the presence of firearms. The cause of death in 67% of domestic violence fatalities in Pennsylvania is a firearm. Abusers are five times more likely to kill their partner if they have access to a gun.
This bleak picture adds up to a Pennsylvanian being shot every two hours, on average.
While of course this is a human tragedy – one that physicians are left on the front-lines to address – it’s also an enormous financial burden on the healthcare system. One study found $1.57 billion in annual hospital costs alone from gun violence, which is likely an undercount that does not include physician and other costs. This is money spent treating the symptoms of a crisis that could surely be better used to improve health and wellbeing if we can address the root cause of gun violence: unfettered access to deadly weapons.
And you have a uniquely powerful ability to help do just that.
The Opportunity
The credibility and trust that your white coat, blue scrubs, and medical expertise affords you gives your voice a heightened impact when it comes to shifting the perspective of the public and decisionmakers, and mobilizing others to push for systemic change.
As a physician, you have a powerful opportunity to serve your patients in a new way, outside of a medical setting, to advocate for an environment that is more conducive to their health and safety, and that would free up the healthcare system to focus on other pressing public health issues. One might even argue that given your Hippocratic Oath to “improve the public health,” you have an obligation to get involved, even in a small way.
CeaseFirePA invites you to join us in this work, with two easy actions you can take:
continued on next page
27 SPRING 2024 : Philadelphia Medicine philamedsoc.org
Dr. Arvind Venkat, an Emergency Physician and now a first-term State Representative, speaks on the front steps of the State Capitol at CeaseFirePA’s 2023 “March For Our Lives: PA Advocacy Day”
Photo Credit: Michael Mason
This is Your Lane continued from page 27

1. Sign-up to join the “This is Our Lane” public health gun violence prevention coalition, a statewide network we’re building to give doctors, nurses, and other medical professionals opportunities to speak out for policy change.
2. Attend “End Gun Violence: PA Advocacy Day” in Harrisburg on Tuesday, May 7, 2024. Stand with us and dozens of other healthcare professionals for a rally at the State Capitol and engage state lawmakers on pending legislation.
The Solutions
The evidence is clear that states with stronger gun laws have less gun violence. And the good news is that research shows there are a number of effective policy prescriptions immediately available.
Among the many policies for which CeaseFirePA advocates, four core priorities form our Common Agenda to End Gun Violence:
1. Safe Storage to require that firearm owners secure their firearms when not in use. This has been shown to prevent school shootings, unintentional shootings, and suicides, especially by preventing children from accessing weapons.


2. Lost and Stolen Gun Reporting to prevent firearms from being illegally trafficked into communities for use in community violence.
3. Extreme Risk Protection Orders (ERPOs) to provide family members and law enforcement a tool to temporarily restrict access to firearms to prevent firearm suicides, mass shootings, and domestic violence killings.
4. Closing the loophole in PA’s background check system and enacting universal background checks will prevent violent felons and other dangerous individuals from accessing long guns including military-style, semi-automatic rifles.
One of the first things learned in medical school, nursing school, or other public health institutions, is that preventing disease and harm is better for the individual – and often cheaper – than reacting after the fact to treat the symptoms and injuries.
These policies are society-wide preventative care. And working together, we can get them passed into state law, and save lives. •
About the Author: Adam Garber is the Executive Director of CeaseFirePA Education Fund and lives in Philadelphia. CeaseFirePA’s mission is to organize with communities closest to the issue of gun violence, hold those in power accountable, and maximize the strengths of every member in its broad coalition — understanding that the strongest work is work done by many. Learn more at CeaseFirePA.org.
28 Philadelphia Medicine : SPRING 2024 FEATURE continued philamedsoc.org
A physician watches supportively as the PA House Judiciary Committee votes to advance a package of Life-saving gun safety legislation (March, 2023)
Photo Credit: Michael Mason
The Legislative Year in Review 2023
“Unpredictable” is probably the best word to describe the many changes that have taken place over the past year…both from a legislative perspective and a political one, although the two are often inextricably linked.
Shortly after the 2022 House of Delegates in October that year, the General Assembly approved Senate Bill 225, prior authorization reform legislation. This proposal was the result of nearly six years of stakeholder meetings, physician coalition discussions, meetings with PAMED physician leaders, and grassroots physician advocacy. The new law made changes to the time-frames health insurers have to make prior auth decisions, refined the definition of medical necessity related to prior authorizations, streamlined the process of medication step therapy and enacted changes to the qualifications of peer-to-peer reviewers. Passage of Senate Bill 225 was applauded by physician organizations across the Commonwealth along with members of the legislature. Though more work needs to be done when it comes to the relationship between physicians, health insurers and patients.
November 2022 also brought the election of a new Governor, Josh Shapiro, and a historic shift of power in the state House of Representatives with democrats edging out a one seat majority. These changes, coupled with the untimely death of Anthony DeLuca, a democratic member of the House, impacted the ability of the General Assembly to “hit the ground running” in early 2023. Adding to the political complexities of a new legislative session was the resignation of several democrat house members who had been elected to other offices, including Lt. Governor Austin Davis. As a result, the “business” of the House didn’t really get started in a serious way until April.
We were also happy to see the election of Arvind Venkat, MD, to the State House of Representatives, the first physician to do so since 1961. Since his swearing in, Dr. Venkat has made a positive impression with members of his caucus and has, more than once, influenced or helped shape health care legislation in Harrisburg. We anticipate that Dr. Venkat will continue to be a driving force, and trusted source of clinical knowledge, to many members of the legislature. It should be noted that PAMED’s political action committee, PAMPAC, was an early supporter of Dr. Venkat’s candidacy.
Politics aside, we have seen several proposals put forth this legislative session that has PAMED very much engaged. We saw the reintroduction of Senate Bill 25, legislation that would grant CRNPs with independent practice authority and expect to see a companion bill introduced in the House before the end of the year. Legislation was also introduced to allow pharmacists to prescribe medications. A public hearing on this measure, House Bill 1000, was held in September with future stakeholder meetings expected. Staying with the theme of scope of practice expansion, PAMED has been engaged with the PA Chapter of the American College of Obstetricians Gynecologists in considering a legislative proposal that would no longer require nurse midwives to maintain a collaborative agreement with an OB/GYN. As of early December, consideration of these proposals is not expected in the near term.
While PAMED spends considerable resources on scope of practice issues, there are a number of bills, unrelated to scope, on which we are actively engaged. These include, but are not necessarily limited, to the following in no particular order:
Pennsylvania orders for Life Sustaining Treatment (POLST)—PAMED continues to work on moving proposals in both the Senate and House to address the issue of POLST. Sen. Gene Yaw (R-Lycoming) has introduced Senate Bill 631 and Rep. Tarik Kahn (D-Philadelphia) has introduced the companion bill in the House as House Bill 1212. Committee consideration of House Bill 1212 could come in early 2024.
Insurer credentialing—PAMED has identified Sen. Ryan Aument (R-Lancaster) as a possible sponsor in the Senate for legislation to shorten the time it takes to credential providers with health insurers. PAMED is working on several fronts to gather documented information on the delays in the credentialing process. It should be noted that Rep. Steve Mentzer (R-Lancaster) has introduced a version of our credentialing bill in the House as House Bill 1510.
Non-Compete Agreements—As mandated by the PAMED House of Delegates, we continue to discuss the issue of noncompete agreements in physician contracts with many legislators. Interest in this area seems to be growing as lawmakers learn more about how these contractual agreements negatively impact patient
29 SPRING 2024 : Philadelphia Medicine FEATURE philamedsoc.org
The Legislative Year in Review 2023 continued from page 29
access and continuity of care. Sen. Michele Brooks (R-Venango) has re-introduced a proposal, Senate Bill 521, that would require a patient to be notified if their physician changes practices. Under the legislation, patients would receive the appropriate contact information for their physician should they choose to continue seeing their provider in another location. The bill would also void non-compete agreements when a physician is terminated “without cause.” The Hospital and Healthsystem Association of Pennsylvania opposes this legislation. In the House, Rep. Dan Frankel (D-Allegheny) has introduced House Bill 1633, a proposal that would outright ban the use of non-compete agreements in all physician employment contracts. PAMED will be working with Rep. Frankel, and other policy makers in the House, to move this proposal forward. While PAMED supports House Bill 1633, our support is contingent upon adding a provision that would permit the use of non-compete agreements by private physician practices.
Bio-markers—Legislation introduced by Sen. Devlin Robinson (R- Allegheny), Senate Bill 1754, would mandate that health insurers cover the costs associated with diagnostic tests to determine a given patient’s biomarkers related to a specific illness.
Rep. Kyle Mullins (D-Lackawanna) has joined with Rep. Bryan Cutler (R-Lancaster) in introducing House Bill 954, another biomarker proposal as well and a companion to the Senate version. PAMED, along with abroad coalition of provider organizations and patient advocacy groups, supports both legislative initiatives.
Telemedicine—PAMED is hopeful that a telemedicine bill may finally get to the Governor’s desk this legislative session. Sen. Elder Vogel (D-Beaver) has once again introduced Senate Bill 739 of which PAMED is supportive.
ED Overcrowding—PAMED has asked Governor Josh Shapiro to establish a task force on the issue of ED overcrowding. While no legislative remedy to this crisis has been introduced, PAMED hopes to work hand-in-hand with the Shapiro administration in identifying a solution and following through with its implementation.
Mental Health Access—PAMED, along with the Pennsylvania Psychiatric Society (PSA), has embraced the collaborative care model between psychiatrists and primary care physicians as a way of expanding mental healthcare services to patients in need.
House Bill 849, authored by Rep. Mike Schlossberg (D-Lehigh), provides funding to establish coordinated care models in primary
care offices. The language also includes a model that utilizes psychologists in care models as well.
Reproductive Health—PAMED has met with Rep. Leanne Krueger (D-Philadelphia) regarding her proposal to expand access to contraceptives. Her proposal, House Bill 1140, would remove limitations on the duration of prescriptions for patients taking medications that not only prevent pregnancies but also treat ailments such as endometriosis and Polycystic ovary syndrome. PAMED is working cooperatively with Rep. Krueger to “tighten” aspects of the bill to ensure that physicians ultimately have control of the prescription process.
Constitutional Amendment on Abortion—Rep. Danielle Friel Otten (D-Chester) introduced House Bill 1888, a constitutional amendment measure that would enshrine within the state constitution an individual’s right to exercise personal reproductive liberty related to pregnancy. A constitutional requirement to hold a public hearing on the proposal was satisfied on December 12, 2023. It is anticipated that the bill will be considered by the full House of Representatives in early 2024.
Although the current legislative session has been less than robust, a breast cancer related proposal authored by Sen. Kim Ward (R-Westmoreland) made it to the finish line in record time in May of this year. Senate Bill 8, lauded as a “first-ofits-kind” in the country to improve breast cancer screening coverage of necessary BRCA testing and screening for high-risk Pennsylvanians, had the support of PAMED and several patient advocacy groups. PAMED played an active role in helping to develop this legislation through several meetings between PAMED Board Chair and oncologist Ed Balaban, DO, and Sen. Ward’s legislative staff. The bill was signed into law by Governor Josh Shapiro as Act 1 of 2023.
As we begin the 2024 legislative calendar, PAMED is looking ahead strategically on many of the issues contained in this report. We anticipate a busy legislative agenda as lawmakers will be looking ahead to the state’s April primary election and of course, the Presidential election in November of 2024. As always, PAMED members are encouraged to develop relationships with their local state representatives and state senators. These relationships will play a key role in helping PAMED to achieve our legislative goals. •
30 Philadelphia Medicine : SPRING 2024 FEATURE continued philamedsoc.org
Humanitarian Medicine

My name is Juan, I am an Argentine-Canadian internal medicine resident working out of Pennsylvania Hospital in Philadelphia with a focus on humanitarian medicine, and these are my field journals.
Humanitarian work has always been my goal, even before I started medicine. As a final year medical student – at the height of covid no less – I was able to finesse myself an elective with a humanitarian group in the Panamanian Jungle doing point of care mobile medicine. Acting as the medical lead due to unprecedented staffing shortages, my first day thrust me right into the thick of it as I ran a trauma in the field for a 13 year old boy kicked unconscious by a horse. One broken pulse oximeter, a makeshift stretcher, and two blistered hands from extricating our patient through kilometres of dirt path later, I confirmed what I already knew: that I had found my calling. This was the beginning of a career that continues to take many twists and turns, and a journey that I hope to share with anybody who will care to listen.
I started this blog to provide a window into the world of humanitarian medicine in hopes to inspire others to embark on a life of humanitarian service. You will find archived the notes from all my missions, many of them different in their own way: refugee camps, NGOs, government field hospitals, academic centres, and some things in between. I hope that you will find something of value in them; in particular to my colleagues in medicine, I

want you to see yourselves practicing in these non-traditional settings. Our help is needed in these places more than anywhere else.
Most recently, I spent a week working in Western Uganda providing point of care ultrasound training for medical staff at Kyangwali Refugee Settlement, home to over 130 000 asylum seekers living in extreme poverty. Read about my time there at the link below
https://humanitarianmedicjournals.com/a-new-start/
31 SPRING 2024 : Philadelphia Medicine philamedsoc.org
FEATURE

































Meet Our Healthcare Banking Expert Andre Jones, Senior Relationship Manager Healthcare Banking 484.947.6309 | CitadelBanking.com/Healthcare WELCOME TO BETTER Built for Your Practice BUSINESS BANKING We understand that starting, running, and expanding a practice is no small feat. Our team of Relationship Managers offers years of experience partnering with healthcare professionals to develop custom strategies that address your distinct needs and challenges. Citadel is recognized as a Forbes 2022 Best-in-State Credit Union. Federally Insured by NCUA
