
Marzia Chowdhury
Ph.D. Candidate
Department of Architecture
The University of Kansas
PORTFOLIO
sample
Academic and Research work

Marzia Chowdhury
Ph.D. Candidate
Department of Architecture
The University of Kansas
Beyond the Darkness Socio-Cultural Center Education Center for Visually Impaired Children
Learning the Past and Developing the Future London Housing Design Competition
Emergency Department Design in Response to the Pandemics:
A Systematic Literature Review of Emergency Department Responses to Previous Pandemic and Epidemic
Emergency Department (ED) Design for Pandemic Conditions: Lessons Learned from the COVID-19 Pandemic
Understanding the Relation between Healthcare Accessibility and Population Health Outcome by Implementing ArcGIS
Impacts of the Cohort Isolation Design Strategy in Emergency Department on the Patients’ Operational Outcome
A Nationwide Survey on Emergency Departments (EDs) Pandemic Responses
Undergraduate Academic Level
Graduate Academic Level
Poster Presentation in Conference
Presentation in Conference
Unpublished
Unpublished
Unpublished
Socio-Cultural Center Education Center for Visually Impaired Children
Learning
London Housing Design Competition

Project type Socio-Cultural Center
Location Dhaka, Bangladesh
Setting Historical
Despite the efforts of public and private organizations, the education and overall development of visually impaired and blind children in Bangladesh is still an underdeveloped sector. This has resulted in a significant gap that needs to be addressed urgently. To address this issue, a comprehensive research study was conducted to explore the different ways in which visually impaired and blind people interact with the built environment and its elements. The study included a) a literature review, b) interviews with visually impaired individuals and their associates, and c) an in-depth



Regular Vision Visually Impaired People Vision
analysis of the built environments (e.g., schools) in Bangladesh and other countries to gain a better understanding of how the built environment can create an inclusive environment and promote mobility.
The objective of this undergraduate project was to establish definitive design criteria that can facilitate the creation of a multi-faceted environment that promotes integration for both visually impaired and normally sighted individuals. The aim is to create a more comprehensive and inclusive learning and integrating environ-



ment that can help visually impaired and blind children overcome the challenges they face and achieve their full potential.
The study aims to provide visually impaired and blind children with the necessary tools to succeed in their academic and personal lives. It also seeks to raise awareness about the importance of creating inclusive and accessible environments that can help promote the integration of individuals with disabilities into society.





The sensory responses of a built form are defined by its architectural features such as edge, transition, threshold, path, landmark, and space. For designers, it is crucial to consider these features as design principles to establish a strong connection with memories and feelings. Inclusive design requires a deep understanding of visual impairment, which is essential to create an architectural character that is accessible to everyone.
The incorporation of the layering concept in the design has brought about a remarkable diversity that plays a crucial role in sustaining the built form as a center for integration. When dealing with a site that has roads on three sides, designers are often met with the challenge of providing access from both sides. To overcome this challenge, two entrances are created using




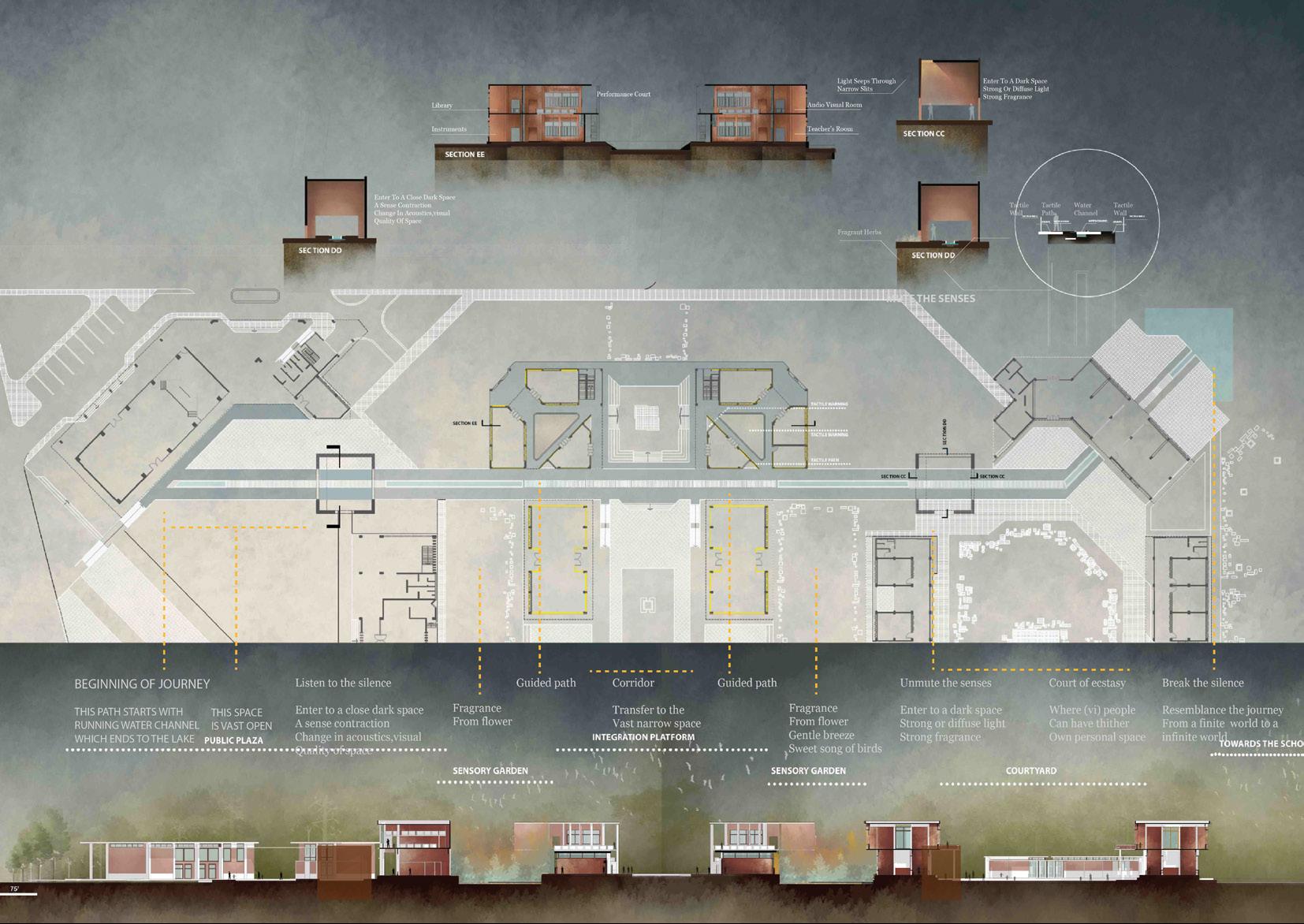
Path
The path of sensuous journey runs along the water channel and leads to the lake. The acoustics of water and associated other sensory clues like visual and olfactory sensory.
There is visual, acoustics landmark help user to orient.
and enclosed built-environment with wall grooves make the navigation more easier.
two different approaches – one for pedestrians and the other for vehicles. Transverse and lateral layering have been implemented to ensure maximum adaptability and flexibility in the design. These layers have been strategically placed to not only enhance the aesthetic value of the design but also to optimize functionality and ensure the smooth flow of traffic.
There is visual, acoustics landmark help user to orient.

The path of sensuous journey runs along the water channel and leads to the lake. The acoustics of water and associated other sensory clues like visual and olfactory sensory.
Trees Trees and enclosed built-environment with wall grooves make the navigation more easier.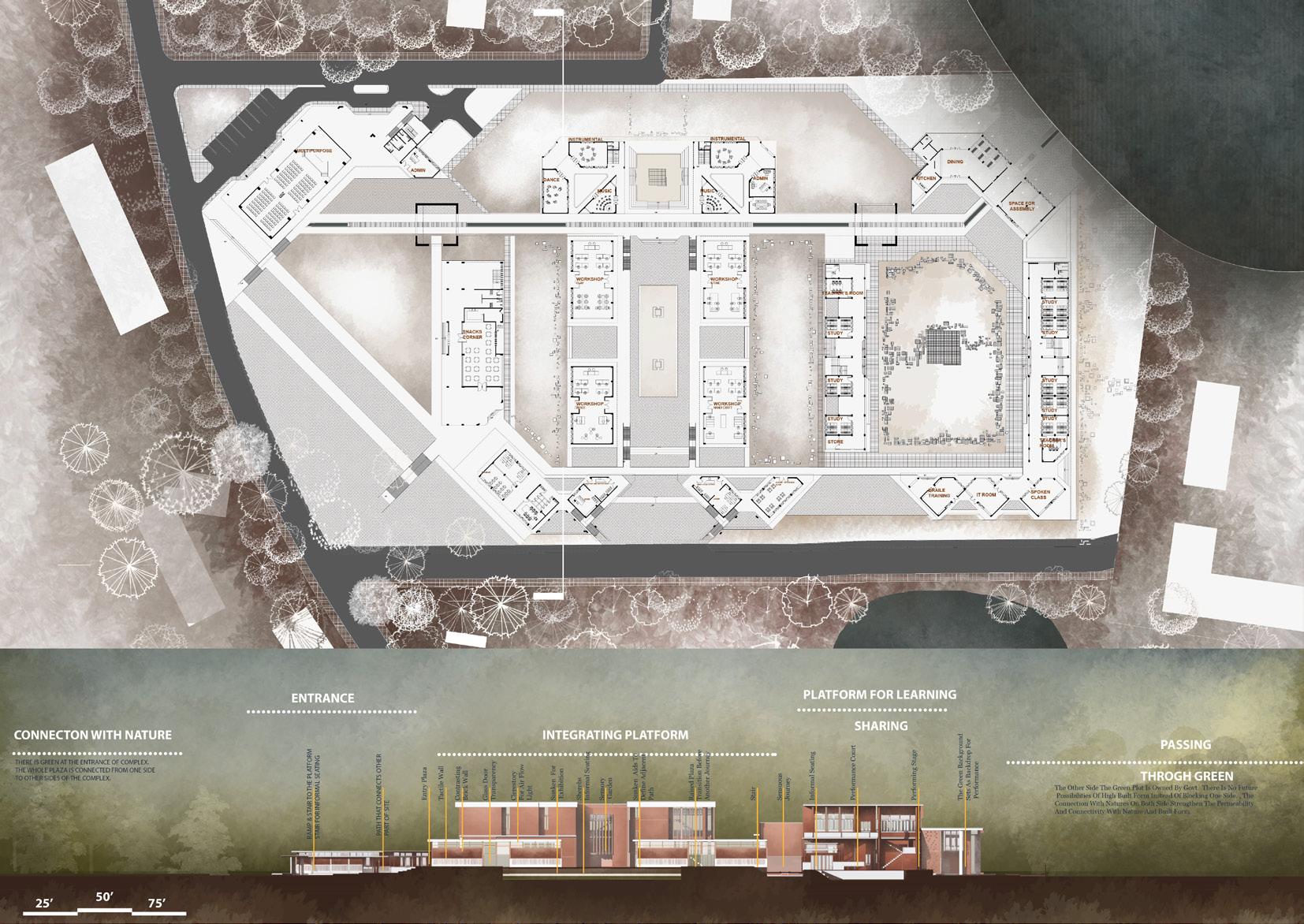
Prof. Micheal Grogan (Lead), Mahruf Kabir, Nazmun Akter, Marzia
Chowdhury
Project type Competition Project
Area Area
Location London, United Kingdom
Setting Residential
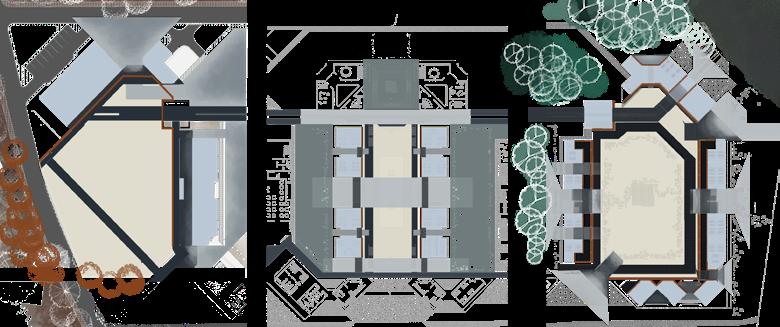
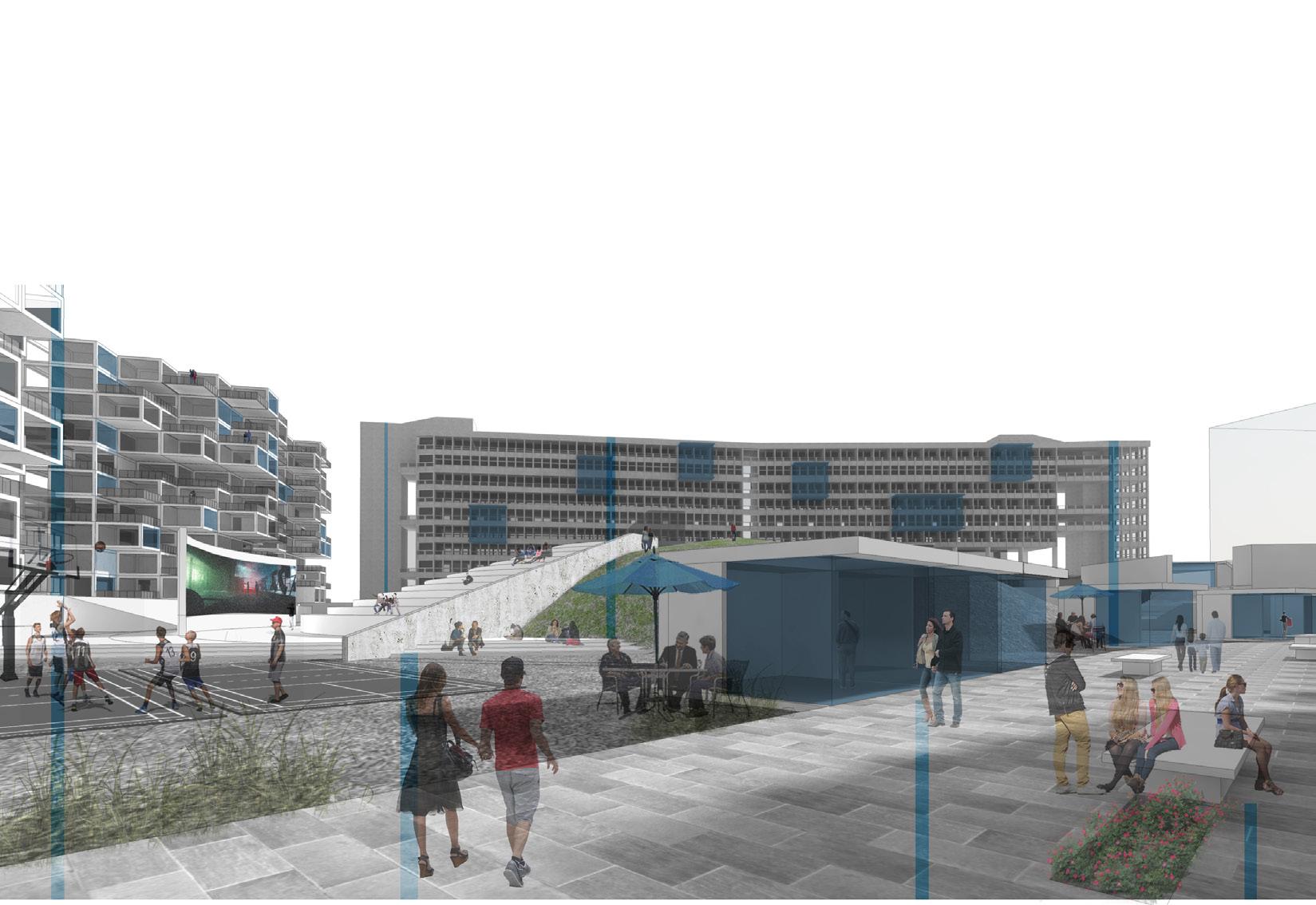
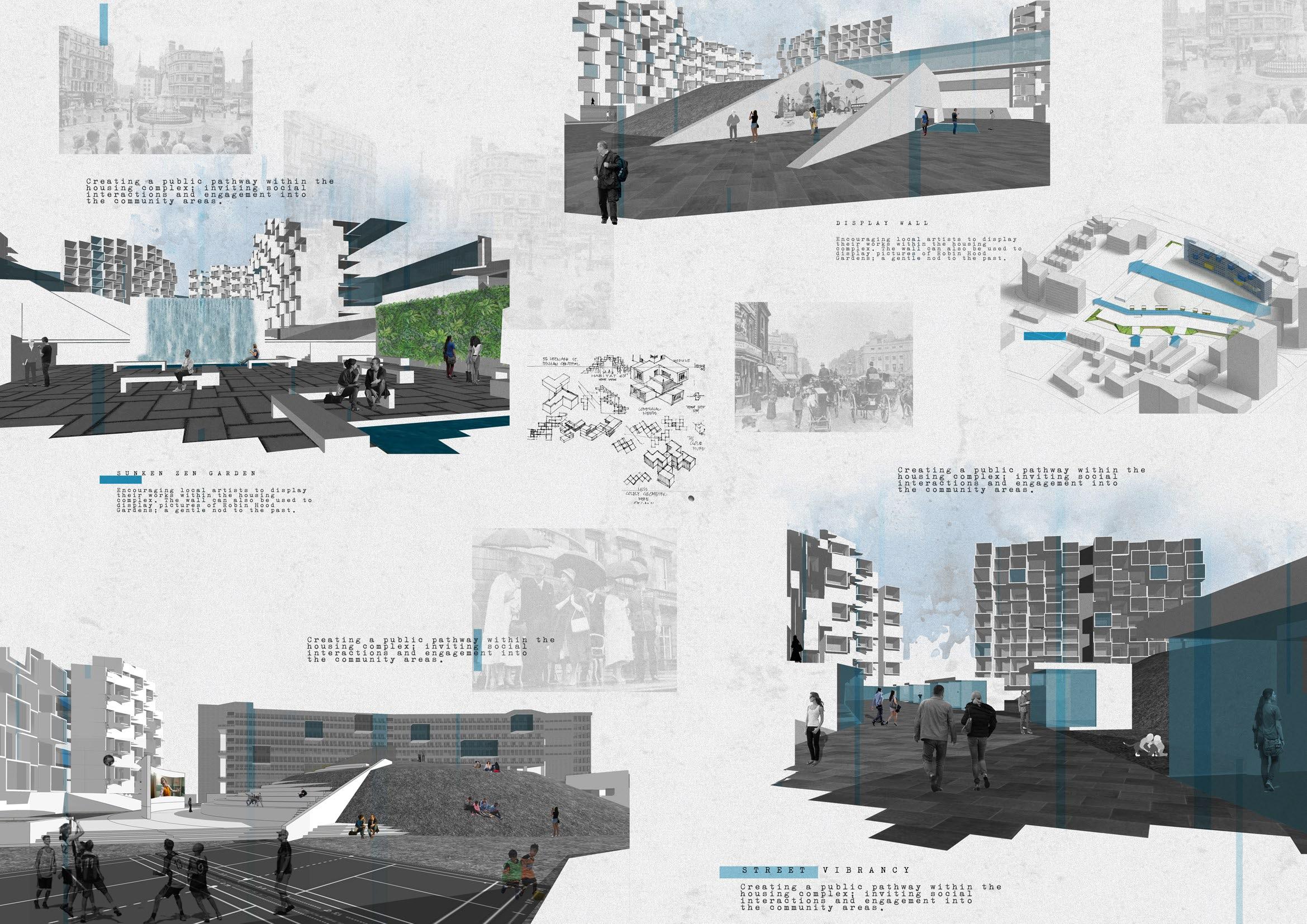
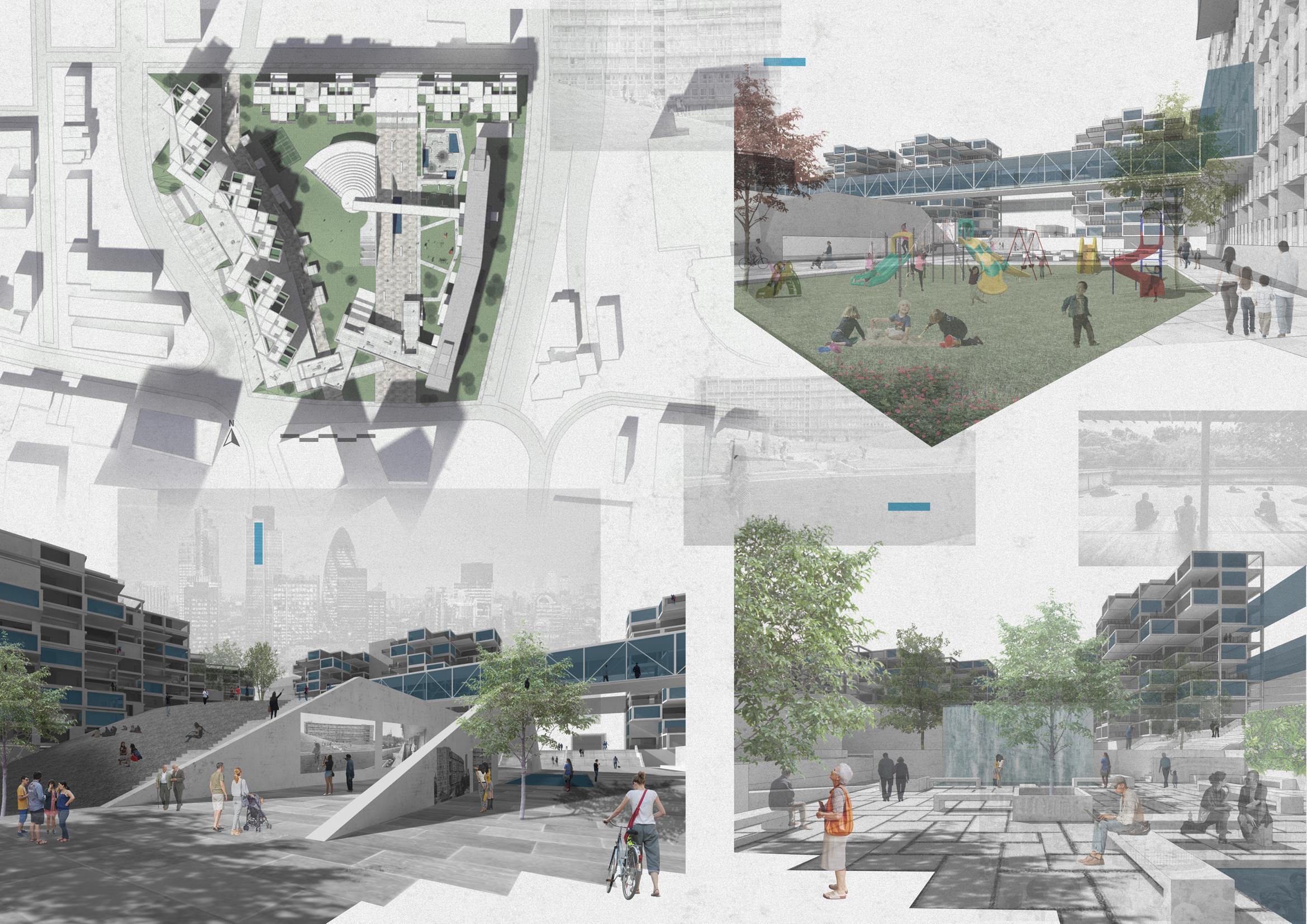
This proposal seeks to retain and celebrate the architectural history, often maligned, of the Alison and Peter Smithson-designed Robin Hood Gardens. What remains of this original
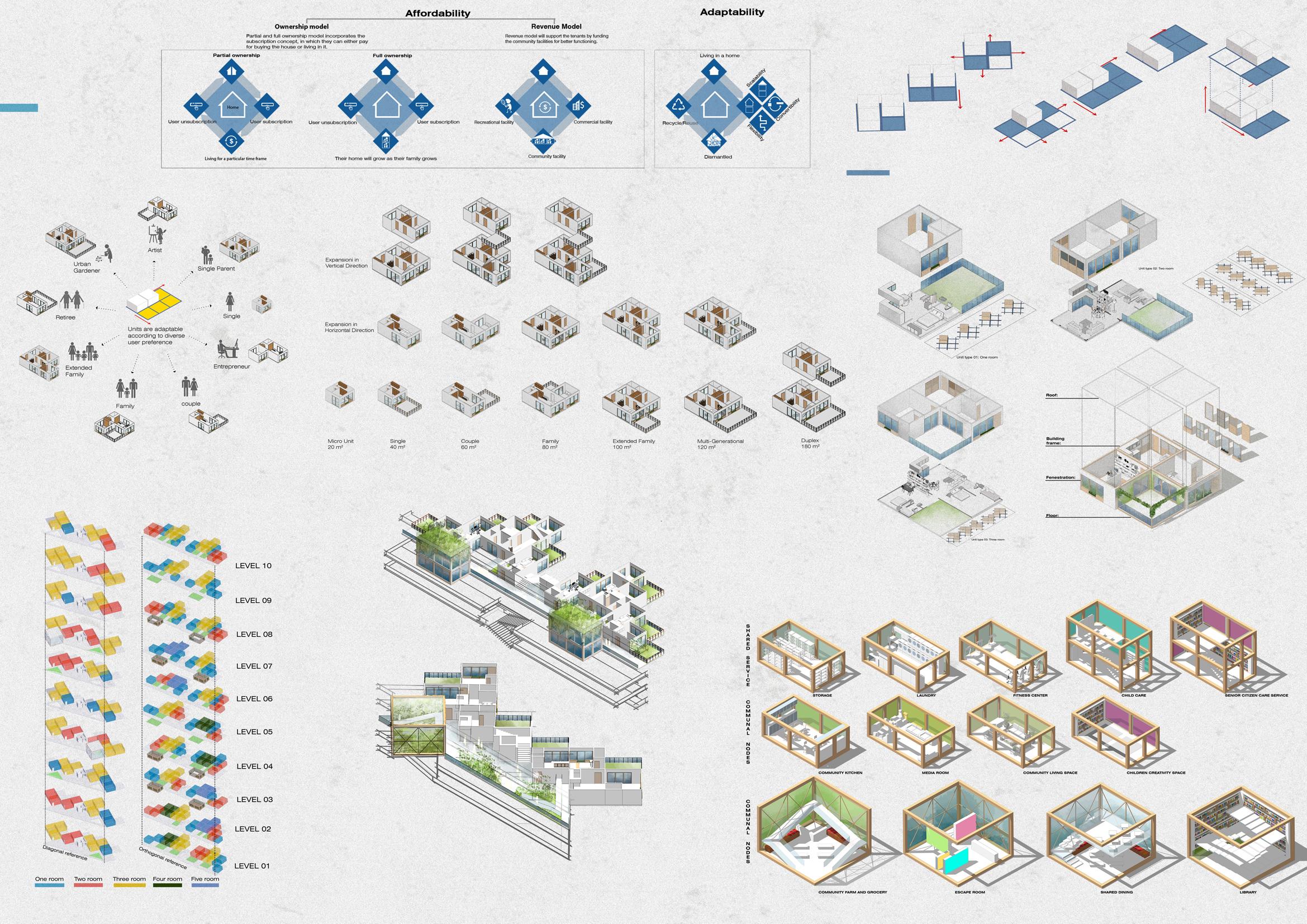
Contribution― the west housing block and conical berm― will be retained with new additions that re imagine an approach towards mass housing while also opens the site to the public realm though publicly-oriented uses, and new throughsite pedestrianized connections a series of activated open spaces. This proposal is predicated on reversing the severing― channeling OMA’s CRONONCAOS― of the connection between architecture and idealism; the much needed social project of contending with the housing crisis after the fall of Council Housing. Though retaining and replicating aspects of the former design, permeability and connectivity of the complex, rather than autonomy, is the objective with an eye towards an urban and socioeconomic intertwining. The proposed aggregations of housing are both prototypical, potentially realized throughout London and the region, and situational, grounded in the logics of the
Poplar site and context. Here distributed in connected clusters, two forms of housing are proposed based on modules connected to a circulatory and services armature. One form is composed of fixed and stackable units, that may be slightly modified to increase unit size and amenities. More flexible is a system of framed modules that can incorporate different panel types and be easily extended for both interior and exterior expansion.
Linking the housing aggregations, we revisit the previously-questioned concept of “streets-in the-air,” first proposed in the Smithsons’ Golden Lane Housing proposal. Pushing this archetype beyond the simple concerns with smooth circulation (two women with prams not “blocking the flow”) we push further the idea of “intervals” as socially-activating nodes. These nodes― interior and exterior― may accommodate spaces for social gathering, meetings, small performances, child care, an so forth. With a strategic dispersion of these communal nodes, the re-envisioned “streets” will prove more inviting, complex, and purposeful-yet-flexible, finally becoming the “social entities” previously
conceived.
All of this, on the Robin Hood Gardens site, transitions to the ground through a gradient of semi-public-to-public uses in a base that transforms from berm to plinth to bridge to ultimately connect to the existing block’s second story “street” which has been partially transformed. The berming and plinth, mainly along the north and east streets, accommodate retail and public access points. The bridge portion along the south provides community functions, here conceived as small library and galleries, though typologically this may accommodate other programs. As importantly, this forms a portal into the site. Two pedestrian paths run north-south to connect a school and religious complex at the north to new developments south of the parcel. Other connections occur along the east, the west remaining edged by the remaining building that also forms a barrier to the noisy A 102 highway. Continue on about elements in the open spaces


Emergency Department Design in Response to the Pandemics: A Systematic Literature Review of Emergency Department Responses to Previous Pandemic and Epidemic
Emergency Department (ED) Design for Pandemic Conditions: Lessons Learned from the COVID-19 Pandemic
Impacts of the Cohort Isolation Design Strategy in Emergency Department on the Patients’ Operational Outcome
A Nationwide Survey on Emergency Departments (EDs) Pandemic Responses
Understanding the Relation between Healthcare Accessibility and Population Health Outcome by Implementing ArcGIS
The COVID-19 pandemic has presented serious challenges to emergency departments (EDs). EDs play an important role in responding to pandemics, as they made the first substantial strides to recuperate patients and protect them from infectious diseases, as shown in experiences of earlier infectious disease surge events (e.g., SARS-CoV, H1N1, and Ebola, etc.). However, there is limited evidence on how facility design can support EDs’ response to pandemics.
This article aims to provide a systematic literature review (SLR) of EDs’ challenges and responses to pandemics, with a primary focus on facility design strategies. The authors followed the “Preferred Reporting Items for Systematic Reviews and Meta-Analysis” (PRISMA) guideline and searched the databases; PubMed, Web of Science, Science Direct, PubMed central database, covering the literature from March 2000 to March 2021. 2489 studies were identified by the initial database keyword search and additional hand search based on literature search. Finally, 20 articles met the inclusion criteria.
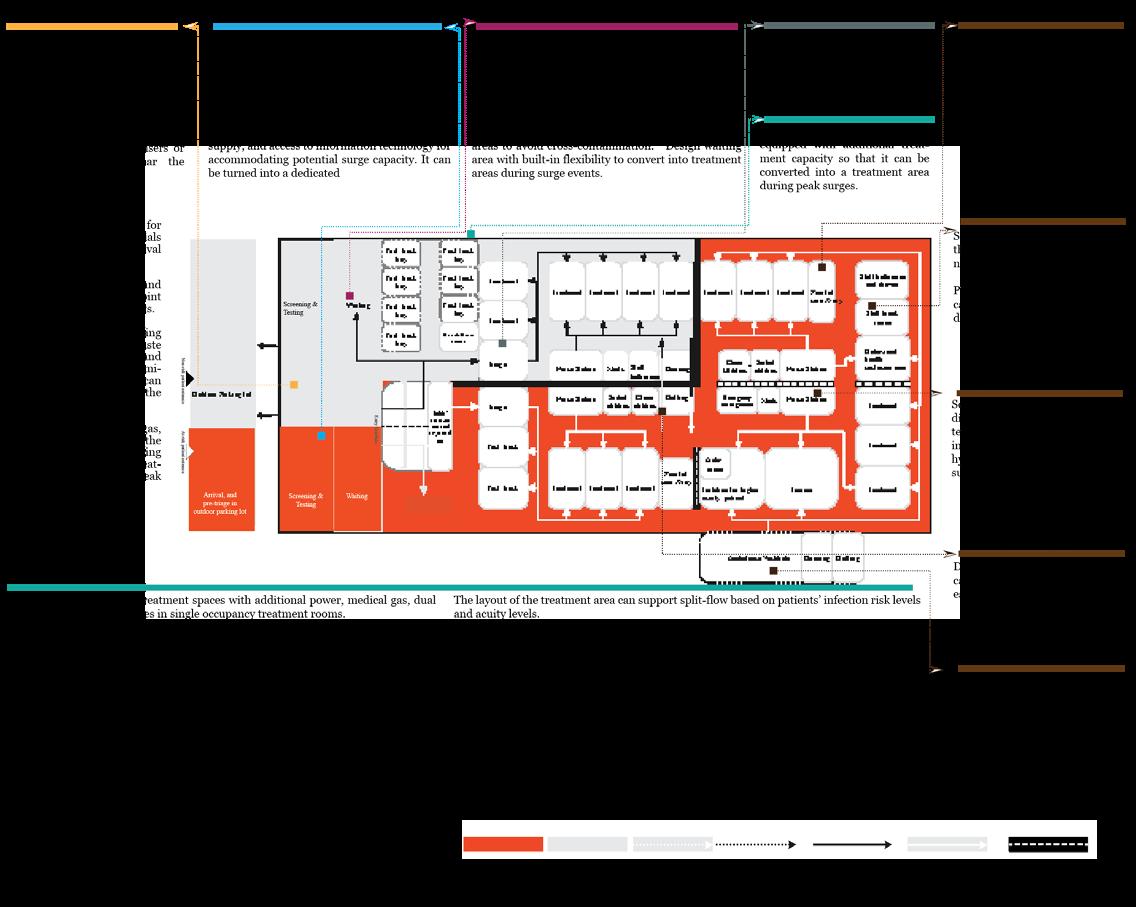
Key findings include a) negative pressure rooms b) split flow and cohort isolation that can create various zones for patients with different risk and acuity levels are the most addressed approaches for infection control and accommodating surge capacity. Convertibility and flexibility concept (e.g., reconfiguration of spaces, temporary separation within spaces, reversible air pressure, flexible use of treatment and non-treatment spaces within and adjacent to ED) is key to address unique challenges of evolving nature of pandemic outbreaks.
This study provides a summary of existing design strategies for EDs to respond to pandemics. Multiple design strategies need to be combined to minimize the disease transmission in EDs during pandemics and providing surge capacity for overflow of patients. Detailed design principles were synthesized based on the SLR and translated to a design prototype that can respond to evolving stages of pandemics.
This article can be helpful to front-line staff in clinical settings, hospital administrators, public or government officials, architects, and the like. It also identifies opportunities for further research on EDs design to better respond to pandemics.
Keywords:
Emergency department, surge capacity, design strategies, pandemics, infection control strategy
Current Knowledge on Surge Capacity Infection Control Strategy

The aim is to develop a comprehensive review of the literature and summarize the current knowledge of the spatial strategies that EDs in respond to pandemic-related surge events.
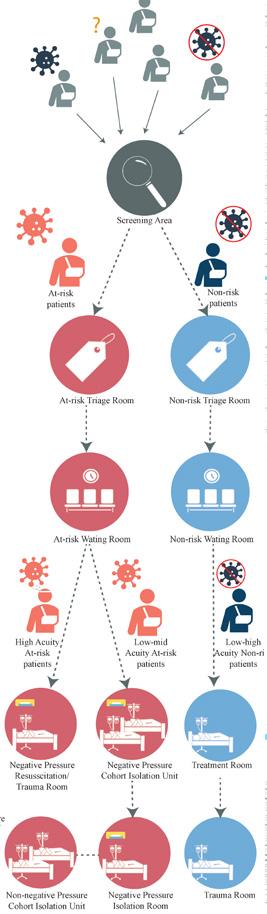
Screening Area
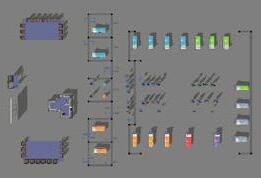
Waiting Area Surge Capacity
(Regular-Full Pandemic Mode)
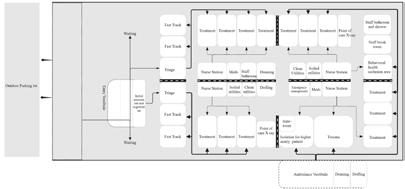
Regular Operational Hour
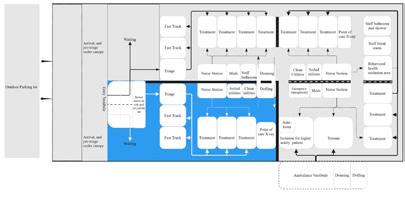
Pandemic Mode: Initial Surge

Pandemic Mode: Mid Surge
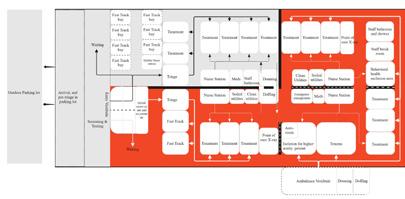
Pandemic Mode: Full Surge
Does ED design make a difference in responding to the pandemic at different phases?
What are the pandemic resilient design features?
How did that ED design affect the ED operational metrics, First wait time (door to provider time), and treatment time (provider to disposition time) for different cohort patient groups?
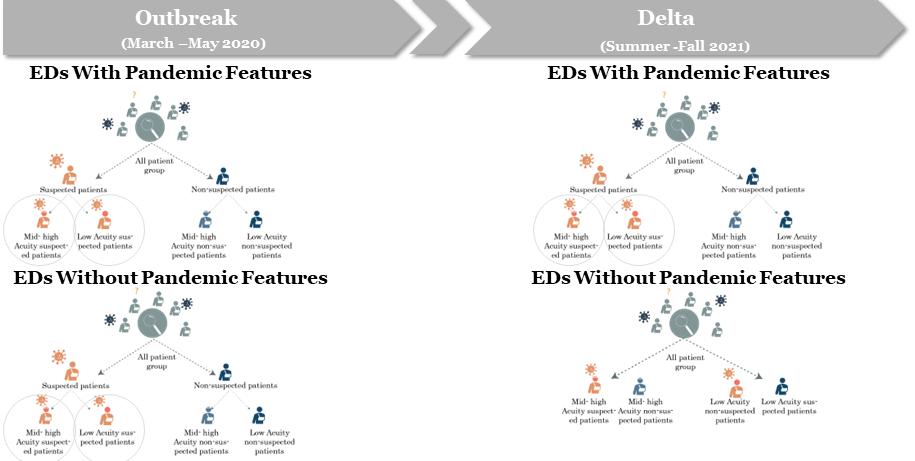


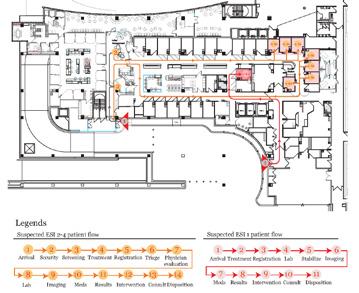
Some key strategies for EDs’ to address pandemics have been identified: a)the split flow of suspected and non-suspected patients; b)the provision of separate screening, triaging, waiting, and cohort isolation zones for suspected patients; and c) adaptive use of treatment and non-treatment areas within and adjacent to ED spaces and conversion of non-treatment areas to accommodate surge capacity.




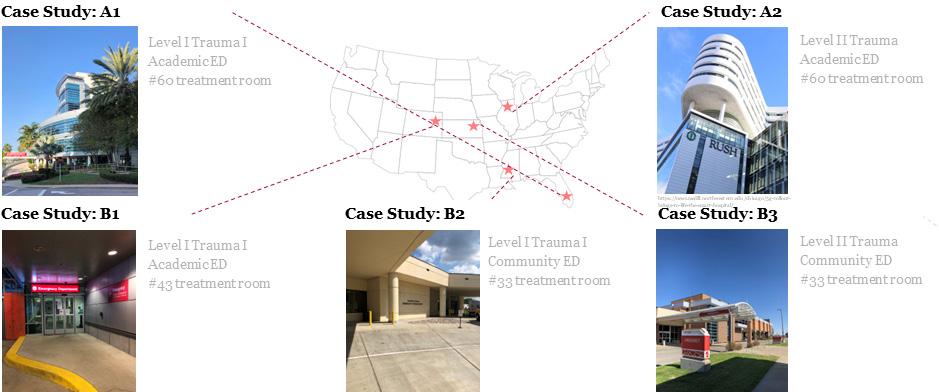
Case Study A1

Case Study A2

Case Study B1
Case Study A1

Case Study A2
Case Study B1
Infection Control Strategies





Mass Decontamination Area/ Decon Area
Modular/ Pod Design in Treatment Area
Negative Pressure Isolation Room
Negative Pressure Isolation Unit
Separate Toilet in Negative Pressure Isolation Room/ Unit
Separate Patient Route from Arrival to Negative Pressure Isolation Room/ Unit
Surge Capacity Strategies



Built-In Flexibility In Non treatment Area
(Medical Gas, Power Outlet in non-treatment area, Also Consider access to support and services)
Double Occupancy in Treatment Room
(Dual Headwall and dual power column)
Acuity-adaptable Treatment Room
(Access to necessary power column, medical gas outlet)
Modular/ Pod Design in Treatment Area
During the initial phase of the pandemic, utilizing cohort isolation units proved to be highly effective in reducing the infection risk. However, many Emergency Departments (EDs) discontinued this strategy due to the low utilization of these units.
This study investigates how the treatment room numbers in the cohort isolation unit affect the ED operational metrics, such as first-wait time (door-to-provider time) and treatment time (provider-to-disposition time) for different cohort patient groups by the status of COVID-19 virus, and then ESI level.
This study is based on predictive analytics using DES. It will use the actual ED operational data to build a baseline simulation model and propose a series of “what-if” scenarios to test the effectiveness of various cohort isolation strategies using hypothetical layouts during two time periods: the first phase of the pandemic when cohort isolation strategy was implemented and later period when it was not implemented.
Time-stamped patient-level EMR (Electronic Medical Record) data spanning from March 2020-March 2021 has been collected from an academic tertiary hospital ED to develop and validate the baseline DES model using FlexSim 2021.
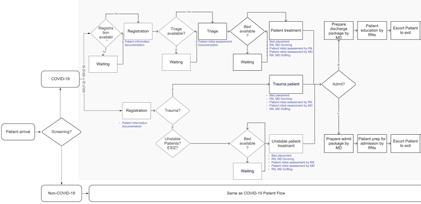
A stochastic profile of patients and their activities was constructed. The process maps were created to describe various types of patient flow and the related resource utilization (e.g., staff, equipment, space) from patient arrival to patient disposition. Then, the simulated and actual ED patient outcome data of interest will be compared for model validation.
Utilization rate comparison between two spatial strategies across diff. resources
COVID-19 patients’ first wait time comparison between two spatial strategies across diff. risk level and acuities
COVID-19 patients’ LOS comparison between two spatial strategies across diff. acuities
Average of Waiting time during "cohort isolation" period
Average of Waiting Time during "without cohort isolation" period
Average of
during "cohort Iisolation"
Average of LOS during "without cohort isolation" period
The chart displays the variations and effects of different design strategies on the LOS, waiting time, treatment room utilization rate, capacity, and staff requirements of different patient cohorts. The purpose is to assess the effectiveness of different design models. The chart demonstrates that cohort isolation units have enhanced bed utilization rates as beds were exclusively allocated to them during the initial phase of the pandemic. Furthermore, it has improved the overall LOS for the COVID-19 patient group.
The prolonged COVID-19 pandemic created multiple surge demands at various phases of the pandemic. Pandemic responses vary across different EDs. However, there is little research on the connection of the built environment in response to adopted strategies.
Value df Asymptotic Significance (2-sided)
Separate pre-triage/screening area
Urban-rural 0.49 1 0.484
Hospital Size 4.236 1 0.04*
Objective Method

This study aims to evaluate pandemic preparedness approaches from a facility design perspective for different periods and identify their relationship to EDs’ characteristics.
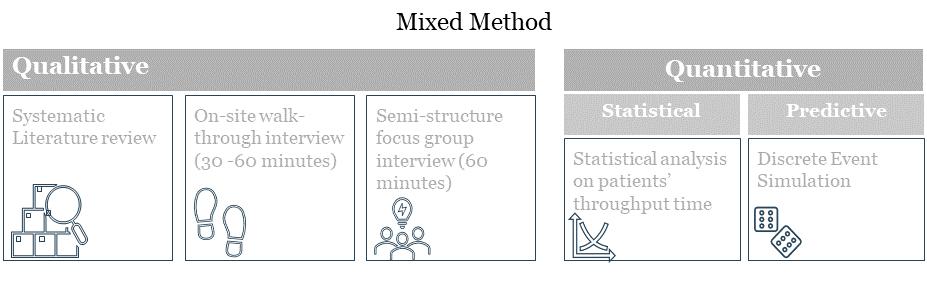
A qualitative research method has been conducted, including a systematic literature review (SLR) to understand ED design strategies and a nationwide survey to evaluate the strategies during different periods of the pandemic. The survey was distributed through the EDBA (Emergency Department Benchmark Alliance) from September 2022 to October 2022. The survey asked for information on strategies to address pandemic needs in their EDs. A descriptive statistic and Chi-squared test of independence were conducted to evaluate what design strategies various EDs in the United States have implemented to respond to the COVID-19 pandemic.
Results

The participants in this study showcased an array of diversity in their respective geographical locations. Among the five regions, the Midwest emerged as the frontrunner with a staggering 37% representation (n=19/57), while the Southwest exhibited the smallest proportion (n=02/57, 4%). It was also observed a relatively higher number of Level I trauma centers among the sample (n=27/57, 47%).

Academic status 1.403 1 0.236
Trauma level 1.467 1 0.226
Separate triage area for suspected infectious patients
Urban-rural 1.96 1 0.162
Hospital Size 0.01 1 0.920
Academic status 8.077 1 0.004*
Trauma level 0.271 1 0.602
Separate patient flow for infected and non-infected patients
Urban-rural 1.544 1 0.214
Hospital Size 0.078 1 0.78
Academic 5.53 1 0.019*
Trauma 0.759 1 0.384
Dedicated donning and doffing area
Urban-rural 0.188 1 0.665
Hospital Size 0.008 1 0.931
Academic 3.989 1 0.046*
Trauma 0.97 1 0.325
Out of the 130 respondents for the EDBA survey, 57 completed all sections and were included in the analysis. The most adopted strategies are —a) negative pressure room (95%, n=54/57), b) cohort isolation (84%, n=48/57), and c) separate pre-triage or screening area (84%, n=47/57). Almost half (48%) of the strategies were implemented at the onset, whereas only 17% were before the outbreak.
The statistical analysis revealed significant differences between types of EDs and the design strategies they have adopted in response to the pandemic. For example, academic EDs are associated with a higher chance of adopting separate triage at twice the rate (1, N = 57) = 7.75, p = 0.004; separate patient flow X2 (1, N = 57) = 5.53, p = 0.019; and separate dedicated donning and doffing areas X2 (1, N = 57) = 3.989, p = 0.046. Hospital size is also significantly associated with the likelihood of adopting separate screening areas, X2 (1, N = 57) = 4.236, p = 0.04.
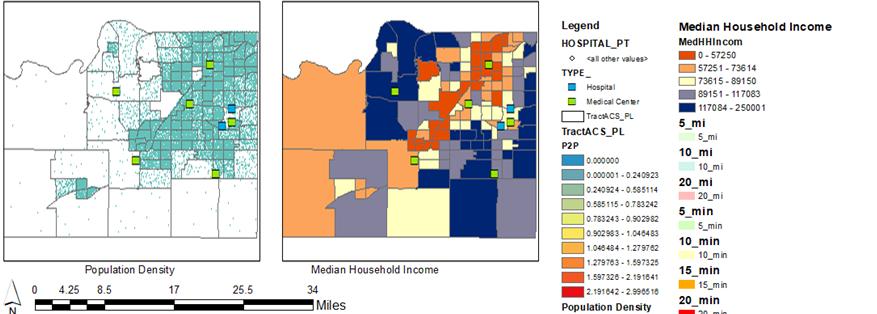
Assessing accessibility involves understanding the five dimensions of a healthcare facility: availability, accessibility, affordability, acceptability, and accommodation. Availability and accessibility are particularly related to spatial factors and geographical location. In order to ensure population health, healthcare accessibility is considered a critical factor (Guagliardo, 2004).
By identifying underserved areas, this article aims to draw a connection between primary care physician access and the health outcome of the overall population.


Connection between primary care physician access

Health outcome of the overall population.
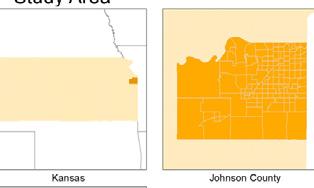
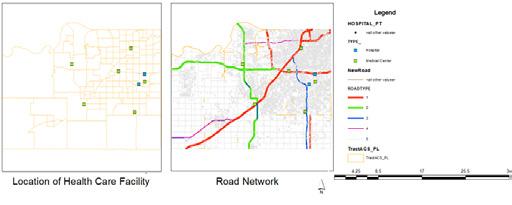
As a case study, this article focuses on potential healthcare accessibility and identifying potentially underserved areas in Johnson County, Kansas, which have the highest health outcomes in population health.
The two-step floating catchment area method is implemented by incorporating the ‘Network Analyst’ extension of the ArcGIS 10.7.1 software. The extension incorporates several functions, among them the OD cost distance matrix and service area functions that are specifically helpful for this project.
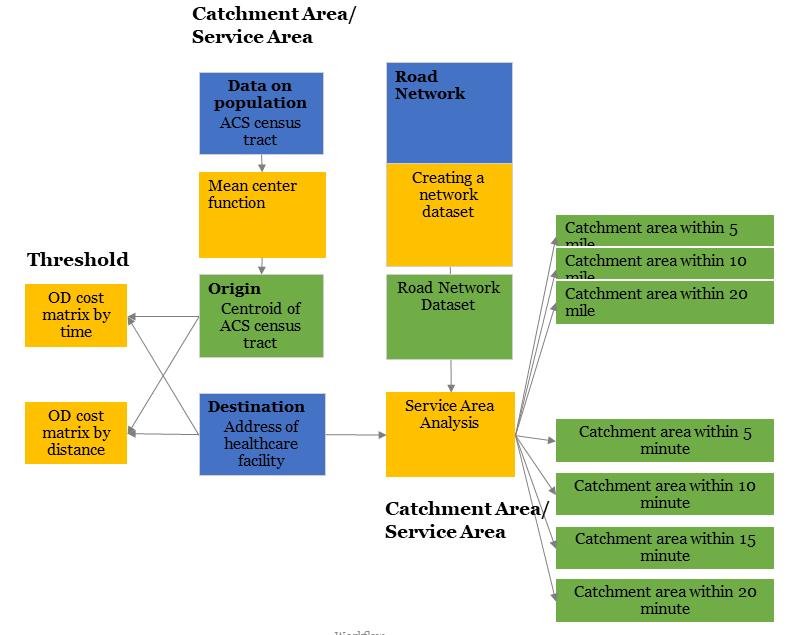
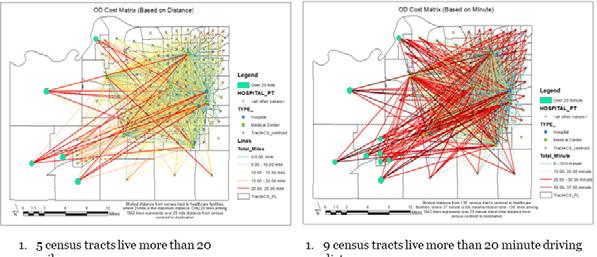
How many people/ census tracts live inside or outside of “healthcare facility zones”? The racial and socio-economic characteristics of the population inside and outside the catchment of healthcare facility zones that offers physical and mental health services.
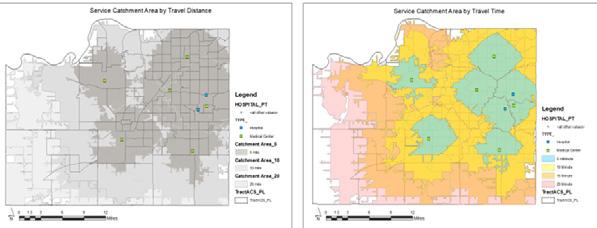
How much area of Johnson County is covered by “healthcare facility service zones”?
Healthcare Accessibility
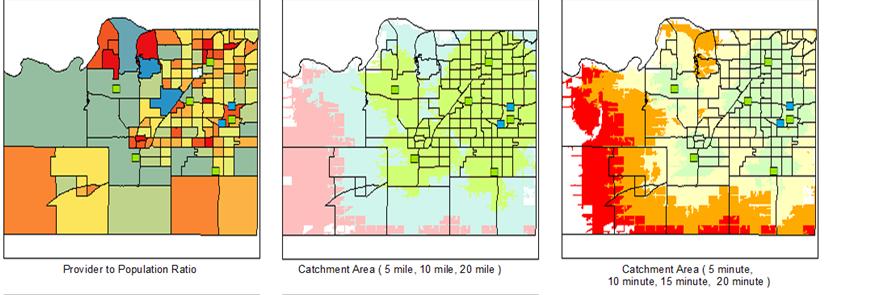
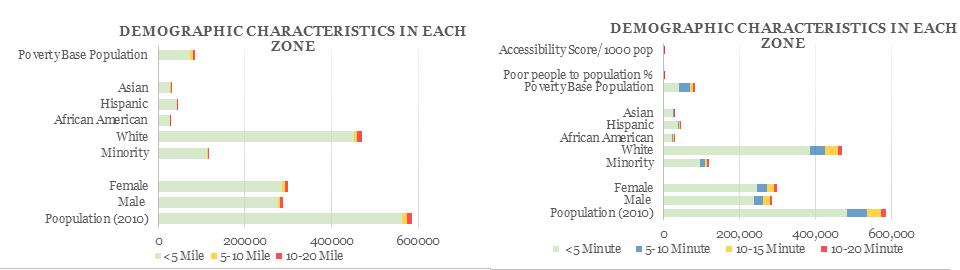





The objective behind analyzing based on both travel time and travel distance was to understand if there is any significant difference in the accessibility. But, the second analysis which is based on the travel time has similar kind results in the output. Most of the minority groups and most of the people below poverty level live within the proximity zone. Where most of the people live within 5 minutes travel distance. 98% of total population live within 20-minute drive and 10-mile travel distance. One of the explanations of equitable access in Johnson County, KS could be that it is already saturated with the healthcare facility. In the last six years, there is an expansion of the healthcare facility in that county. ¹
1 (https://www.kansascity.com/news/business/health-care/article230523004.html)
Guagliardo, M. F. (2004). “Spatial accessibility of primary care: concepts, methods and challenges.” International journal of health geographic 3(1): 3.