The ERS Vice President discusses AI in lung cancer care and the importance of patient education
Personalising Potentially Surgically Resectable Stage IIIA Lung Cancer Treatment Feature:
04 Editorial Board
07 Welcome
09 Foreword
Congress Review
10 Review of the European Respiratory Society (ERS) Congress 2024, 7th–11th September 2024
Congress Features
21 Overcoming the Challenges of Increasing Urbanisation in Respiratory Health
Helena Bradbury
25 The Future of Lung Transplantation in Cystic Fibrosis
Aleksandra Zurowska
Symposium Reviews
30 Emerging Concepts in Bronchiectasis: Diagnosis, Pathophysiology, and Relevance in Lung Disease
41 Transforming Care in SEA: Evidence and Considerations for Evolution of the Current Treatment Paradigm
51 Prioritising Patients and Planet: Advocating for Change in Respiratory Care
63 Heterogeneity of Inflammatory Processes and Pathways Driving Chronic Obstructive Pulmonary Disease Pathology
73 Bronchiectasis Exacerbations: Are We Doing Everything We Can?
Abstract Reviews
82 Antifibrotic Treatment Efficacy in Progressive Pulmonary Fibrosis: Single Centre Experience
Okumus et al.
84 Inhalation Innovation: Phase IIb Study Design of Inhaled Pirfenidone in the Treatment of Progressive Pulmonary Fibrosis
Kolb et al.
Congress Interview
97 Joanna Chorostowska-Wynimko
Interviews
101 Patricia Silveyra
104 Antonio Anzueto Infographics
108 Don’t Hold Your Breath: Adapt and Become More Resilient Against Air Pollution
110 Understanding COPD: Current Treatments and Emerging Breakthroughs
Features
112 Precision Strikes: Personalising Potentially Surgically Resectable Stage IIIA Lung Cancer Treatment with Targeted and Immune Therapies
Bertolaccini et al.
119 Advancing Respiratory Care: The Role of Simulation in Clinical Education
J. Brady Scott
Article
123 Unveiling the Rarity: Pleural Metastasis of Papillary Thyroid Cancer – A Case Report and Clinical Implications
"We
care for patients from birth to old age, from prevention to palliative care, based on respiratory physiology"
Editorial Board
Editor-in-Chief
Antonio Rossi
Senior Medical Director, Oncology Center of Excellence, Therapeutic Science & Strategy Unit, IQVIA, Milan, Italy
He has been a medical oncologist at the Division of Medical Oncology of the S.G. Moscati Hospital of Avellino, Italy, since 2002. A graduate of the “Federico II” University of Naples, where he earned his medical degree and board certification in medical oncology with highest honours, Rossi is an expert in lung cancer and a member of numerous prestigious oncology societies, including AIOM, AIOT, ASCO, ESMO, and IASLC.
Catharina Belge
University Hospitals Leuven, Belgium
Jacques Bouchard
Université Laval, Canada
Andrew Bush
Imperial College London, UK
Nicholas Hill
Tufts University School of Medicine, USA
Martin Balzan
University of Malta, Malta
Giorgio Walter Canonica
Humanitas Research Hospital, Italy
Enrico Clini
University of Modena, Italy
Oliver Eickelberg
University of Pittsburgh, USA
Atul Gupta King's College London, UK
Dario Olivieri
University of Parma, Italy
Neil Holden
University of Lincoln, UK
Mohammad Azizur Rahman
Dhaka University, Bangladesh
Islam Ibrahim
University of California, USA
Paraschiva Postolache
Peter Barnes
Imperial College London, UK
Grigore T. Popa University of Medicine and Pharmacy, Romania
Aims and Scope
EMJ Respiratory is an open access, peer-reviewed ejournal committed to helping elevate the quality of practices in interventional cardiology globally by informing healthcare professionals on the latest research in the field.
The journal is published annually, six weeks after the European Respiratory Society (ERS) Congress, and features highlights from this event, alongside interviews with experts in the field, reviews of abstracts presented at ERS, as well as in-depth features on sessions from this event. The journal also covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
EMJ Respiratory also publishes peer-reviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field and broaden readers’ professional interests. The journal is managed by a dedicated editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copy editing, and ensures timely publication.
EMJ Respiratory endeavours to increase knowledge, stimulate discussion, and contribute to a better understanding of practices in the field. Our focus is on research that is relevant to all healthcare professionals in this area. We do not publish veterinary science papers or laboratory studies not linked to patient outcomes. We have a particular interest in topical studies that advance knowledge and inform of coming trends affecting clinical practice in the respiratory filed.
Further details on coverage can be found here: www.emjreviews.com
Editorial Expertise
EMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors who are recognised authorities in their respective fields.
• Peer review, which is conducted by expert reviewers who are invited by the Editorial team and appointed based on their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area.
All peer review is double blind. Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected.
Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects. We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial.assistant@emjreviews.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in EMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
EMJ is distributed through controlled circulation to healthcare professionals in the relevant fields across Europe.
Indexing and Availability
EMJ is indexed on DOAJ, the Royal Society of Medicine, and Google Scholar®; selected articles are indexed in PubMed Central®.
EMJ is available through the websites of our leading partners and collaborating societies. EMJ journals are all available via our website: www.emjreviews.com
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
All information obtained by EMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, EMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. EMJ is completely independent of the review event (ERS 2024) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever. The cover photo is of Vienna, Austria, the location of ERS 2024.
KARL STORZ SE & Co. KG, Dr.-Karl-Storz-Straße 34, 78532 Tuttlingen/Germany www.karlstorz.com In an Emergency, Selecting the Right Bronchoscope Should Not be a Matter of Chance
Editor
Evgenia Koutsouki
Editorial Manager
Darcy Richards
Copy Editors
Noémie Fouarge, Katheeja Imani, Jenna Lorge
Editorial Co-ordinators
Victoria Antoniou
Abigail Craig
Editorial Assistants
Helena Bradbury, Ada Enesco, Katrina Thornber, Katie Wright, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey Rivers
Senior Designer
Steven Paul
Designers
Owen Silcox, Fabio van Paris
Junior Designers
Dillon Benn Grove, Shanjok Gurung
Senior Performance & Insight Lead
Darren Brace
Project Manager
James Murphy
Marketing Director
Kristina Mestsaninova
Chief Content Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and Chief
Executive Officer
Spencer Gore
Welcome
Dear Readers,
Welcome to the 2024 issue of EMJ Respiratory, bringing you all the latest advancements from the European Respiratory Society (ERS) Congress 2024. Prevailing themes in this year’s Congress revolved around lifelong lung health, chronic obstructive pulmonary disease, and the promising prospects of technology solutions, including AI, in respiratory medicine.
Be sure not to miss our congress features that dive into key topics discussed at the Congress, including the challenges of urbanisation on respiratory health and the role of machine learning in cystic fibrosis. Our expert interviewees for this year’s issue explore topics such as sex differences in lung diseases and chronic obstructive pulmonary disease treatments and their impact on patient outcomes.
Among the highlights of this issue is a feature exploring the high value of simulation in respiratory care education alongside the challenges that come with implementing simulation-based learning. Despite simulation-based education being a widely used tool in medical education, there is still a relative lack of data on its effectiveness and impact, and this article helps unravel the key areas of focus for the future.
I would like to close by thanking our peer reviewers, Editorial Board members, and all of the contributors for helping this great issue materialise by offering their valuable insights on the review and creation of the content. We welcome your submissions and feedback over the next 12 months, and until then, I hope you enjoy reading this issue.
Editorial enquiries: editor@emjreviews.com
Sales opportunities: salesadmin@emjreviews.com
Permissions and copyright: accountsreceivable@emjreviews.com
Evgenia Koutsouki Editor
Reprints: info@emjreviews.com Media enquiries: marketing@emjreviews.com
Foreword
It is my pleasure to introduce the latest issue of EMJ Respiratory. In this edition, you will find peer-reviewed articles alongside a review of the European Respiratory Society (ERS) Congress 2024, which took place in Vienna, Austria, between 7ᵗʰ–11ᵗʰ September 2024. The hybrid event saw experts from around the globe come together to present research findings and key updates across a variety of disciplines within respiratory medicine.
The theme for this year’s Congress was ‘Humans and Machines: Getting the Balance Right’, with the programme including several sessions on this topic. In addition to this, other key topics highlighted by ERS’s leadership included the current and future role of humans in AI-supported medical care, thoracic oncology, interstitial lung diseases, and airway diseases.
In theme with the Congress, this issue covers a variety of topics, including a feature article by Bertolaccini et al. that reviewed the treatment landscape for potentially resectable Stage IIIA non-small cell lung cancer and how adenocarcinoma and squamous carcinoma have evolved over the years. Additionally, an article by Salak et al. covers an interesting case of pleural metastasis of papillary thyroid cancer and its clinical implications.
You can also find an insightful interview with key opinion leaders in the field of respiratory medicine, covering topics such as new advancements and developments in the treatment of chronic obstructive pulmonary disease, and sex differences in lung diseases.
I would like to take this opportunity to thank all of those who have contributed to this issue, including all the authors, peer reviewers, interviewees, and Editorial Board.
I hope you enjoy reading this journal.
The theme for this year’s Congress was ‘Humans and Machines: Getting the Balance Right’, with the programme including several sessions on this topic
Antonio Rossi Senior Medical Director, Oncology Center of Excellence, Therapeutic Science & Strategy Unit, IQVIA,
Milan, Italy
ERS 2024
We care for patients from birth to old age, from prevention to palliative care, based on respiratory physiology
Review of the European Respiratory Society (ERS) Congress 2024 Congress Review
WITH an impressive 34,000 members, attendees from more than 160 countries worldwide, and a record number of early career members, the European Respiratory Society (ERS) Congress 2024 was one to be remembered. Taking place in the vibrant and historical Vienna, Austria, from 7th–11th September, the Congress featured dozens of symposia, lectures, abstract presentations, and scientific posters from experts in the field, discussing all of the hottest topics in respiratory medicine, as well as the latest breaking research into chronic obstructive pulmonary disease (COPD), bronchiectasis, and much more.
The bustling event kicked off with a welcome from the ERS President, Monika Gappa, Children’s Hospital, EVK Düsseldorf, Germany, who expressed her gratitude at the vast number of healthcare professionals and key opinion leaders who came together from around the globe, both in person and online, to make this year’s ERS Congress the best one yet. “We care for patients from birth to old age, from prevention to palliative care, based on respiratory physiology to basic research into new molecules,” she highlighted to an engrossed crowd, emphasising just how vital organisations such as ERS and everyone who works with them are.
Gappa went on to discuss the theme that has continued in the society throughout her career, lifelong lung health. With a wealth of research having come out in recent years about the effects of early life events on lung health in adult life and the new initiative from the ERS, ‘Healthy Lungs for Life’, this has become and continues to be a priority for
the organisation and the clinicians involved in it. With this comes the responsibility of leading by example, she went on to explain, urging her colleagues to not only advocate for healthier lifestyles amongst their patients but to embrace it themselves, avoiding tobacco, living more sustainably to reduce pollution, and encouraging vaccination against respiratory diseases. Gappa closed her rousing welcome speech by encouraging healthy lifestyles amongst patients and clinicians alike, collaboration between departments, and education for younger individuals in the field, something which ERS is continually improving.
Following the President was none other than medical futurist, Bertalan Mesko, Semmelweis Medical School, Budapest, Hungary, who took to the stage to discuss the transformative impact of science fiction on the medical field. What if technology could save millions of lives? What if a new technological advancement could transform medicine for the worse?
Technology and the role of AI in healthcare have been a topic on the minds of physicians and researchers in every field, and Mesko’s speech aimed to open their eyes to the possibilities these developments hold. He highlighted that in previous centuries, we could spend decades developing one invention, perfecting one piece of equipment; now, thousands of innovative ideas and technologies are coming out every day. These developments have the potential to let healthcare professionals access patient data, insights, information, and diagnostic help faster and easier than ever before; they have been shown to have the ability to predict exacerbations in COPD and analyse spots of lung cancer and signs of primary biliary cholangitis or pneumonia. Mesko’s message was not that AI and technology will one day dominate healthcare, but that they have the ability to make systems more efficient, improve patient relationships, and improve education. He urges everyone to embrace the changes facing respiratory medicine today, balancing human relationships and technology with the goal of improving patient care worldwide. Medical professionals should be leading the way in developing technologies to improve disease prevention and patient outcomes, he pointed out and encouraged his fellow healthcare professionals to look forward to the future of digital health.
Medical professionals should be leading the way in developing technologies to improve disease prevention
The opening ceremony proceeded with these messages in mind, presenting awards to researchers and clinicians who have made a significant impact in the field, as well as welcoming new members of ERS. New webinar series, new educational resources, and exciting new hybrid programmes were announced, highlighting ERS’ commitment to improving education and working with early-career healthcare professionals. The themes of sustainability, technology, and
the dangers of smoking were addressed throughout the session, as well as for the entirety of the Congress, with many lectures and posters emphasising the importance of these issues in respiratory disease.
This year’s Congress was a truly international and collaborative event, in which it was made abundantly clear how important societies such as ERS are when it comes to beating respiratory diseases and educating the population on how to live a healthier lifestyle.
Read on for more key insights into ERS 2024, and make sure to join us next year for ERS 2025, which will take place in the picturesque Amsterdam, the Netherlands.
329
The study involved infants, including both full-term and premature babies, assessed for BPD.
AI Shows Promise in Detecting Lung Disease in Premature Babies
AI has shown promising results in detecting lung disease in premature babies, according to a study presented at the ERS Congress by Edgar Delgado-Eckert from the University of Basel, Switzerland.
The study demonstrated that artificial neural networks (ANN) can effectively identify bronchopulmonary dysplasia (BPD), a serious lung condition affecting premature infants. BPD is challenging to diagnose in newborns, as traditional lung function tests are unsuitable for infants. Currently, BPD is often identified based on prematurity and the need for respiratory support rather than direct lung assessments. Delgado-Eckert’s team developed a novel approach using a soft face mask with a sensor to capture airflow and volume while the newborn is asleep, providing sequential tidal breathing data that the ANN can analyse.
The study involved 329 infants, including both full-term and premature babies, assessed for BPD. The team measured 100 consecutive breaths per baby to train, validate, and test a Long Short-Term Memory (LSTM) model, a type of ANN suited for sequential data. The LSTM model achieved a 96% accuracy rate in identifying BPD from unseen test data, marking a significant advancement in non-invasive diagnostics for infants.
The LSTM model achieved a 96% accuracy rate in identifying BPD from unseen test data
Delagado-Eckert emphasised that this method allows for early BPD detection as soon as 1 month of age, enabling quicker access to treatment and potentially improving long-term outcomes for affected infants. The non-invasive nature of the test also reduced distress for both babies and their parents.
The study team aims to expand their work by testing the ANN’s applicability shortly after birth, assessing lung function in older children, and exploring its potential in diagnosing other conditions, such as asthma.
Epileptic Drug Reduces Symptoms of Sleep Apnoea
SULTHIAME,
a drug currently in use for epilepsy, has been shown to reduce symptoms of obstructive sleep apnoea (OSA), according to results of a clinical trial presented at the ERS Congress.
A primary symptom of OSA is tiredness, but it is also associated with an increased risk of high blood pressure, stroke, heart disease, and Type 2 diabetes. The standard treatment for obstructive sleep apnoea is sleeping with a machine that blows air to keep the airways open, called continuous positive airway pressure machines or mouthpieces. Unfortunately, many people find these machines hard to use over the long term, so there is a need to find alternative treatments.
Researchers conducted a double-blind, randomised, placebo-controlled trial involving 298 people with OSA from 28 different centres in Spain, France, Belgium, Germany, and the Czech Republic. The participants previously reported intolerance to continuous positive airway pressure machines, highlighting the need for alternative treatments. Sulthiame works by targeting the respiratory system, inhibiting an enzyme called carbonic anhydrase, and stimulating the muscles in the upper airway; therefore, the research team investigated the potential benefit of sulthiame in these patients.
The frequency of respiratory pauses during sleep, measured by AHI3a, decreased by 17.8% in patients taking the lowest dose
At the start of the trial, and again at 4 and 12 weeks, patients underwent polysomnography assessments, a diagnostic test that monitors breathing, blood oxygen levels, heart rhythm, eye movements, and brain and muscle activity during sleep. Participants were divided into four groups: 74 received 100 mg of sulthiame daily, 74 received 200 mg, 75 received 300 mg, and 75 were given a placebo.
The frequency of respiratory pauses during sleep, measured by AHI3a, decreased by 17.8% in patients taking the lowest dose, 34.8% in those on the medium dose, and 39.9% in those receiving the highest dose. Using another measure, AHI4, the treatment led to nearly a 50% reduction in respiratory pauses, particularly when oxygen levels dropped significantly. Patients with OSA who experienced daytime sleepiness also reported feeling less sleepy while taking sulthiame. Side effects, such as pins and needles, headaches, fatigue, and nausea, were generally mild to moderate.
In conclusion, the results showed that patients treated with sulthiame experienced fewer breathing pauses and higher blood oxygen levels during sleep. These findings suggest that sulthiame could be an effective treatment for OSA, especially for patients who cannot tolerate CPAP machines.
Medical Clowns Shorten Hospital Admissions for Children with Pneumonia
A RECENT study, presented at ERS 2024, has revealed that medical clowns (MC) can significantly reduce the length of hospitalisation for children with communityacquired pneumonia (CAP), one of the leading causes of paediatric hospitalisation.
Children in the medical clown group had a significantly shorter hospital stay, 43.5 hours on average.
The study, conducted as a prospective randomised controlled trial, included 52 children aged 2–18 years, hospitalised for CAP. The children were split into two groups, one receiving standard care, and the other receiving standard care plus twice daily 15-minute visits from medical clowns during the first 48 hours of hospitalisation. The results showed that children in the medical clown group had a significantly shorter hospital stay, 43.5 hours on average, compared to 70 hours in the control group. Moreover, children treated with the assistance of MCs also needed fewer days of intravenous antibiotic therapy (2.3 versus 5 days) highlighting the clinical benefits of this intervention.
The study supports the view that MCs, trained professionals who use humour, music, and imagination to alleviate stress and anxiety, help children adapt better to the hospital environment. These interactions not only improved psychological wellbeing but also aided children in adhering
to treatments such as oral antibiotics and fluids, contributing to faster recovery.
Furthermore, the research indicates that humour and laughter may have direct physiological benefits, including lowering heart and respiratory rates and enhancing immune function. Karin Yaacoby-Bianu, Carmel Medical Centre, Haifa, Israel, one of the study’s authors, suggested that incorporating MCs into paediatric care could significantly ease the emotional and physical stress on children and their families. The potential cost reduction for healthcare systems is another benefit, as shorter hospital stays reduce overall treatment expenses.
These findings underscore the importance of exploring non-pharmacological interventions, like humour therapy, in paediatric care, opening doors for further studies on the broader impact of medical clowns on other illnesses.
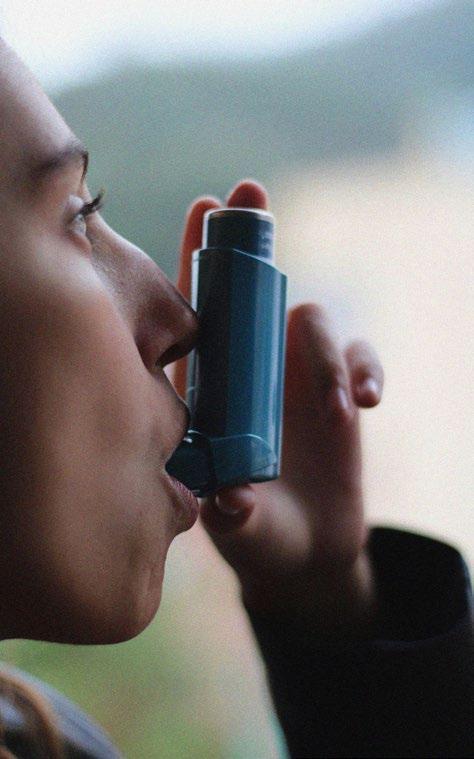
Asthma Linked to Miscarriage and Fertility Treatment in Women
A RECENT study presented at the ERS Congress in Vienna, Austria, has revealed that women with asthma are more likely to experience miscarriages and require fertility treatment. However, asthma does not seem to affect the overall number of live births.
The research, led by Anne Vejen Hansen, Copenhagen University Hospital, Denmark, analysed the reproductive outcomes of 769,880 Danish women born between 1976–1999. The study followed these women from 1994–2017 and classified those regularly using asthma medication as asthmatic.
Findings showed that women with asthma had a higher rate of fetal loss (17.0% compared to 15.7% in non-asthmatic women) and were more likely to use fertility treatments (5.6% versus 5.0%). However, the proportion of live births was the same for both asthmatic and non-asthmatic women, standing at 77%.
Women with asthma had a higher rate of fetal loss and were more likely to use fertility treatments
Hansen explained: “The more severe the asthma and the more flare-ups, the greater the likelihood of needing fertility treatment. While the cause is unclear, it could be linked to systemic inflammation affecting reproductive organs.”
Lena Uller, Head of the Respiratory Immunopharmacology research group at Lund University, Sweden, who was not involved in the study, commented: “It’s reassuring that asthma doesn’t affect live birth rates, but women should be aware of potential fertility challenges. Effective asthma management is essential for reproductive health.”
“The fact that the more severe the asthma, the more the problems with fertility, suggests that uncontrolled asthma is the problem and we should be helping women to get their asthma under control,” she added.
This research highlights the importance of addressing asthma control in women of reproductive age. Further investigations into the impact of asthma on fertility in both women and men are planned.
Saline Nasal Drops Shorten Cold Duration in Young Children
A NEW STUDY presented at the ERS Congress 2024 found that using hypertonic saline nasal drops can reduce the length of the common cold in children by 2 days.
The study led and presented by Steve Cunningham from the University of Edinburgh, UK, showed results from the ELVIS-Kids randomised controlled trial.
A total of 407 children under 6 years of age were included and divided into two groups based on the development of cold symptoms. Group 1 received hypertonic saline ~2.6% (salt-water) nasal drops, and Group 2 received the usual care. Among the 301 children who developed a cold, those treated with saline drops experienced symptoms for an average of 6 days, compared to 8 days for the usual care group. Additionally, children receiving saline drops required fewer medications during their illness.
The saline drops, made of sodium and chloride, work by enhancing the body’s natural defences against viral infections. Cunningham explained that the chloride component helps cells in the nose and airways produce hypochlorous acid, which is used by the body to combat viruses. This mechanism is believed to suppress viral replication, thus shortening the duration of the infection.
The results also showed that fewer households reported family members
catching a cold when children used saline drops (46% compared to 61% with usual care). A significant majority of parents (82%) reported that the drops helped their children recover faster, and 81% said they would use the drops again in the future.
said they would use the drops again in the future % %
reported that the drops helped their children recover faster
The research team led by Cunningham now plans to explore the potential benefits of saline drops on wheezing during colds, as initial results indicated that children who used the drops experienced significantly fewer episodes of wheezing (5% versus 19%).
In conclusion, the findings indicate that using saline drops could be a practical solution for reducing the duration and burden of colds in young children and their families, and potentially easing the health and economic impact of colds worldwide.
Impact of Early Smoking and Packyears on Young Adult Respiratory Health
THE EFFECTS of age at smoking initiation and the number of packyears on the development of respiratory symptoms, such as asthma, have been investigated by researchers from the Obstructive Lung Disease in Northern Sweden (OLIN) project and presented at the ERS Congress 2024.
The study followed a cohort of 3,430 8-yearold participants from 1996 until they turned 19 years old. Data were collected annually from participants through questionnaire surveys on asthma, respiratory symptoms, and once they had reached 13 years old, smoking habits. At 28 years old, a follow-up questionnaire was completed by 2,291 of these individuals, 71% of the original cohort, to assess long-term respiratory health and symptoms.
The study found that 22% of participants had reported smoking at least once daily, with more women (25%) than men (19%) being identified as daily smokers. Of these smokers, 29% had started at or before the age of 15 years, accumulating an average of 2.3 packyears. Another 35% started between the ages of 16 and 17, with 1.8 packyears on average, and 35% began smoking after turning 18, with 1.2 packyears on average.
By age 28, 23% of the participants reported asthma, and 53% experienced at least one respiratory symptom, such as wheezing (36%), or sputum production (30%). The study concluded that both early smoking initiation, before 18 years old, and the total number of packyears were strongly associated with these symptoms. Starting to smoke at the age of 15 years or younger was linked to a significantly higher risk of respiratory issues.
While asthma was also associated with early smoking and packyears, this link weakened after adjusting for factors such as family history of asthma and childhood exposure to smoke. The findings emphasise the need for early intervention to prevent smoking initiation in children and teenagers, given the potential rapid onset of respiratory issues in young adulthood.
The study found...
22%
of participants had reported smoking at least once
35%
began smoking after turning 18, with 1.2 packyears on average
By age 28
23% of the participants reported asthma
53%
experienced at least one respiratory symptom, such as wheezing, or sputum production
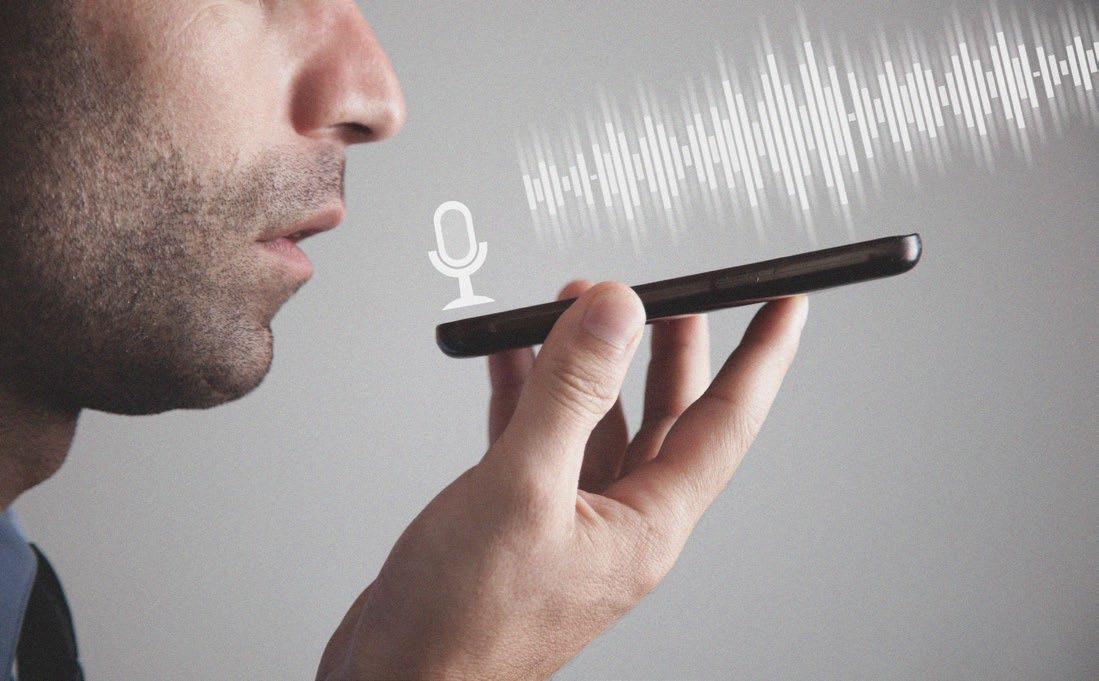
Smartphone Voice Recordings Aid Early Detection of Lung Flare-Ups
A PILOT STUDY presented at the 2024 ERS Congress highlighted how changes in voice recordings on a smartphone can signal the onset of chronic obstructive pulmonary disease (COPD) exacerbations.
COPD, encompassing emphysema and chronic bronchitis, is the third leading cause of death globally, according to the WHO. A flare-up in symptoms like breathing difficulties and coughing (exacerbation) significantly increases the risk of hospitalisation, cardiovascular events, and even death. Early detection is crucial, yet challenging, as these symptoms typically start at home.
This study, led by Loes van Bemmel from Maastricht University Medical Centre, the Netherlands, explored whether voice analysis could predict exacerbations early. She explained that patients had
reported changes in their voice before and during flare-ups, and the study aimed to assess whether these changes could be objectively recorded and analysed to detect early signs.
Twenty-eight patients with COPD participated in the 12-week study, recording their voices daily via a smartphone app. They were asked to say “aah” for as long as possible in one breath, and either read a short story or answer a question after. They also completed daily symptom questionnaires. During the study, there were 16 occasions where exacerbations were recorded.
Twenty-eight patients with COPD participated in the 12-week study, recording their voices daily. During the study, there were 16 occasions where exacerbations were recorded.
Voice recordings were analysed, revealing that the patients’ voices became highpitched when an exacerbation was imminent, and identified more jitter in patients when exacerbation was beginning. These changes support the hypothesis that voice alterations could indicate the onset of an exacerbation. Van Bemmel stressed that these preliminary findings need validation in a larger cohort. If successful, this could enable patients to detect and manage exacerbations at home, improving outcomes and reducing hospitalisations.
Van Bemmel and colleagues in the future plan on developing the SPEAK app, in collaboration with Radboud University Medical Centre, the Netherlands, to detect exacerbations through voice analysis and offer home-based support. Researchers are also focusing on ensuring the secure collection and storage of speech data to protect patients’ privacy.
Frits Franssen, the Secretary of the ERS assembly on respiratory clinical care, commented on the potential of voice analysis for early detection of COPD exacerbations, suggesting that if further validated, this approach could offer an efficient, accessible method of alerting patients and doctors to the need for early intervention, potentially saving lives.
Overcoming the Challenges of Increasing Urbanisation in Respiratory Health
IN THIS year’s European Respiratory Society (ERS) Congress, a session focused on the current challenges related to the impact of urbanisation on respiratory health. This discussion among experts highlighted the role of environmental factors, including air quality, green spaces, and indoor microbiomes, in shaping longterm health outcomes.
SUSCEPTIBILITY IN URBAN ADOLESCENCE
Vivi Schlünssen, Aarhus University, Denmark, opened her talk by referencing the Forsdahl-Barker hypothesis, the theory that inadequate nutrition in early life increases susceptibility to ischaemic heart disease later in life. Now expanded to the ‘Developmental Origins of Health and Disease’, this concept highlights the effects of maternal nutrition on disease risk in adulthood.
A compelling 2022 study comprising 929 offspring aged 18–54, 54% of which were daughters of 308 fathers and 388 mothers (aged 40–66), concluded that fathers’ overweight status in puberty was associated with asthma in adult offspring.1 Additionally, the impact of male smoking in puberty on offspring respiratory health has been widely documented.2
Looking to the future, Schlünssen highlighted several initiatives set out to minimise the effect of urbanisation on adolescent health. First, the societal attitude towards smoking has shifted in recent decades, as this habit is no longer glamorised. The price and unavailability of tobacco products have increased, thus deterring the general public from purchasing such products, and many cities worldwide have adopted a ‘smoke-free’ approach, banning the purchasing and possession of e-cigarettes and creating smoke-free public spaces. Communal, public spaces have also been purposely designed to promote more physical exercise.
A compelling 2022 study concluded that fathers’ overweight status in puberty was associated with asthma in adult offspring
INNOVATIVE STRATEGIES FOR THE ADVANCEMENT OF URBAN RESPIRATORY HEALTH
Alessandro Marcon, University of Alberta, Canada, then took the stage, spotlighting various innovative strategies for improving urban respiratory health and the health benefits of green spaces. Benefits are seen in cardiovascular, mental, respiratory, and metabolic health, as well as pregnancy outcomes.3
An example of this is the ‘Green Corridors’ in Medellin, Colombia, a project set up in 2016 to reduce the city’s heat island effect and improve air quality through the creation of a network of green spaces.4 Costing 16.3 million USD, 30 green corridors, including 20 km of shaded cycle and pedestrian paths, were created. Remarkably, temperatures reportedly fell by 2 °C in the first 3 years following construction.
Marcon then cited several staggering statistics from a 2023 study, namely that across 93 cities in Europe from the summer of 2015, there were 6,700 deaths attributable to urban heat islands (UHI).5 This phenomenon of UHIs occurs when a city experiences significantly warmer temperatures than rural areas in proximity. A key contributor to this is the abundance of human-made materials, such as concrete, that reflect less sunlight than vegetation, causing the neighbouring spaces to warm.
As noted by Marcon, green spaces not only combat UHIs but also remove air pollution. Interestingly, a 2019 study quantified the percentage of different air pollutant types removed by vegetation.6 For instance, restoring land cover in the USA to countylevel average canopy was estimated to remove the pollutants SO2, PM10, PM2.5, and NO2 by 30%, 10%, 11%, and 14%, respectively.
Restoring land cover in the USA to county-level average canopy was estimated to remove the pollutants
SO2, PM10, PM2.5, and NO2 by 30%, 10%, 11%, and 14%, respectively
But are green spaces cost-effective? “In short, yes,” explained Marcon. Displaying a graph from Gopalakrishnan et al.,6 Marcon explained that, for the majority of counties in the USA, tree restoration was more costeffective compared to introducing the best available air pollution removal technologies. As noted by Marcon, the specific species of trees also matter. According to a recent study, it is estimated that around half of the 11,000 trees found on Royal Botanic Gardens Kew’s 320-acre London site in the UK could die by the end of 2090.7 Furthermore, a 2024 study from the University of Vienna, Austria, projected that the number of climatically suitable species per km2 in the EU will fall from 14 in 2020 to nine in 2090.8 These statistics highlight that tree restoration should take into account plant species that will be suitable for future climate scenarios.
Finally, he touched on the future potential of pollen forecasting, which will help significantly with those susceptible to pollen allergies.
URBAN INDOOR MICROBIOME AND RESISTOME EXPOSURE
Following on, Randi J. Bertelsen, University of Bergen, Norway, took the stage to raise awareness of indoor biological exposures and combative efforts to ensure a healthy indoor environment in a future with increasing urbanisation and climate change. In one particular study from Denmark, a team investigated the differences in the microbiome between suburban homes, stables, and the associated farmers’ homes, looking specifically at the bacterial transfer between the livestock and the homes.9 Results found that the bacterial load was highest in the samples from the stables and lowest in the suburban homes. Looking at the bacterial diversity and composition, they concluded that more beneficial bacteria were present in the farmers’ homes than in suburban homes and stables.
In another study, indoor airborne bacteria were collected 10 years apart (2012 and 2022) from the same 27 households for each city: Uppsala, Reykjavik, Bergen, and Aarhus (unpublished data). Using shotgun sequencing, data on the microbiome and resistome were collected. Bergen had consistently high precipitation, whilst Aarhus had the highest wind speed and temperature over the 10-year period. Overall, statistical models revealed that temperature and humidity influence the changes in microbiome composition, likely by affecting growth conditions, moisture availability, stress tolerance, and nutrient access.
Finally, Bertelsen touched on ways to secure a healthy indoor environment, such as using user-friendly, affordable ventilation systems, cleaning regularly, and opting out of certain materials (e.g., wood, carpets, textiles) as they foster the growth of allergens and microorganisms. Within the wider public, she urged for the construction of climate-resistant infrastructure, implementation of stricter air quality standards and regulations for indoor/outdoor environments, and public awareness campaigns on the importance of air quality.
CONCLUSION
Overall, these presentations from the 2024 ERS Congress collectively emphasised the significant impact of environmental and developmental factors on urban health, particularly in adolescence. They highlighted the growing concern over how urbanisation, climate change, and lifestyle choices affect long-term health outcomes, especially respiratory health. Urban planning strategies, such as the introduction of green spaces, were shown to play a crucial role in improving air quality, reducing heat, and promoting overall well-being. Additionally, the importance of addressing both outdoor and indoor environmental factors, including pollution, temperature, and microbiome composition, was stressed as key to creating healthier living spaces.
References
1. Lønnebotn M et al. Parental prepuberty overweight and offspring lung function. Nutrients. 2022;14(7):1506.
2. Accordini S et al. A three-generation study on the association of tobacco smoking with asthma. Int J Epidemiol. 2024;1;47(4):1106-17.
3. Johannessen et al. Greenness exposure: beneficial but multidimensional. Breathe. 2023;(19):220221.
4. Yeung P. How a colombian city
cooled dramatically in just three years. 2024. Available at: https:// reasonstobecheerful.world/greencorridors-medellin-colombia-urbanheat/. Last accessed: 30 September 2024.
5. Lungman et al. Cooling cities through urban green infrastructure: a health impact assessment of European cities. Lancet. 2023; 401(10376):577-89.
6. Gopalakrishnan et al. Naturebased solutions can compete with technology for mitigating air emissions across the United States. Environ Sci Technol. 2019;53(22):13228-37
7. Royal Botanic Gardens Kew. Planting for the future: How Kew is protecting its plants to 2090. 2024. Available at: https://www.kew.org/read-and-watch/ landscape-succession-plan. Last accessed: 30 September 2024.
8. Wessely et al. A climate-induced tree species bottleneck for forest management in Europe. Nature Ecol & Evol. 2024;8(6):1109-17.
9. Amin H et al. Cow farmers’ homes host more diverse airborne bacterial communities than pig farmers’ homes and suburban homes. Frontiers. 2022;13:883991.
The Future of Lung Transplantation in Cystic Fibrosis
AN INSIGHTFUL session on the future of lung transplantation presented at this year’s European Respiratory Society (ERS) Congress explored the insights shared by experts during sessions on lung transplantation, the role of machine learning in cystic fibrosis care, and the future challenges ahead.
IS CYSTIC FIBROSIS STILL AN INDICATION FOR LUNG TRANSPLANTATION?
Clemence Martin from Chochin Hospital, Paris, France, delivered a talk on cystic fibrosis and lung transplantation. Martin presented the results of a 6 month trial conducted in 2019,1 which used a highly effective triple combination of cystic fibrosis (CF) transmembrane conductance regulator (CFTR) modulators in a population of patients with a single Phe508del allele variant, a frequent deletion in patients with CF. The patients with a pulmonary function between 40–50% and aged ≥12 years old were selected. Results demonstrated, for the first time, a rapid and stable increase in forced expiratory volume (FEV1) in these patients. This was also associated with a drop in pulmonary exacerbations, hospitalisations, intravenous antibiotic courses, an increase in body weight, and an improvement in quality of life. However, as the patients were selected based on their pulmonary functions, very few would have been considered for lung transplantation.
Martin described an early access programme in France, which began in January 2020. This programme was designed to provide early access to CFTR modulators for patients with advanced CF, prior to full regulatory approval therapy.
It was specifically aimed at patients with severe lung disease who had limited treatment options.
The introduction of CFTR modulators drastically reduced the number of lung transplantations for CF in France
The eligibility criteria for the programme were carefully assessed, including the presence of the Phe508del allele variant and FEV1 pulmonary function below 40%, indicating significant pulmonary impairment. The goal of the programme was to treat these patients early, offering them a chance to improve lung function and overall health by accessing treatment early. Over the course of the programme, patients demonstrated significant improvements in lung function, reduced oxygen needs, fewer hospitalisations, and better quality of life.
These benefits were maintained over the long term, and some patients no longer required lung transplantation at the end of 1 year of treatment.
Martin also described how the introduction of CFTR modulators drastically reduced the number of lung transplantations for CF in France, from 80–100 per year before the COVID-19 pandemic to around eight per year after. Martin emphasised that this drop is largely attributed to the effectiveness
of modulators in stabilising pulmonary function. However, approximately 8–10% of patients, particularly those with rare or non-responsive CF variants, still require transplantation.
Martin continued by describing the French compassionate programme, which expanded access to CFTR modulators for patients with advanced lung disease, regardless of genotype. Although the need for lung transplantation has decreased, patients with CF with impaired lung function may still require transplants in the future. Martin emphasised that this population requires follow-up, and proper early referral for lung transplantation if necessary.
In her concluding remarks, Martin explained that CF may still be an indication for lung transplantation in two groups of patients: those who cannot access elexacaftor/ tezacaftor/ivacaftor (ETI) therapy, which is the newest CFTR modulator drug approved for the treatment of patients with CF aged ≥6 years with at least one copy of the F508del mutation (F) in the CFTR gene; and those with rare or non-responsive variants, who, despite being initiated on ETI, have advanced lung disease and may still require lung transplantation in the future.
However, approximately of patients, particularly those with rare or non-responsive CF variants, still require transplantation 8–10 %
CAN MACHINE LEARNING HELP US IN PHENOTYPING CYSTIC FIBROSIS AND PREDICT PROGNOSIS?
The second talk was delivered by Tamara Vagg, Cystic Fibrosis Centre, Cork, Ireland. Vagg began by introducing machine learning in the context of phenotyping as an emerging tool in CF research, particularly
in phenotyping, prognosis, and lung transplantation. Machine learning can be used to identify patterns in data, and cluster patients based on factors such as disease severity and response to treatments while improving its predictions over time based on the information it gathers. However, its success depends on the availability of high-quality data.
Vagg described three key studies in this area that demonstrate its potential. Firstly, a 2021 UK-Canadian study2 identified four CF phenotypes independent of lung function, linking them to factors like weight, height, hospitalisations, and pathogen growth, with two clusters showing milder disease and two showing more severe cases. The data demonstrated how ML can be used to refine CF phenotyping beyond traditional markers, offering a more comprehensive view of the disease severity.
The second study, a one French from 20223 predicted patient responses to lumacafor/ ivacaftor after 1 year by analysing CT scans and identified three clusters based on lung abnormalities, age, and MRSA colonisation, as well as other factors. Interestingly, the youngest group in this study has the best treatment response.
This shows how ML can help predict patientspecific responses to CFTR modulators, allowing clinicians to personalise treatment based on predicted outcomes.
Lastly, a 2020 US study,4 used microbiome data to predict lung function decline and demonstrated that analysing the whole microbiome provided better insights than just focusing on pathogens. This suggests that ML can deepen our understanding of how the microbiome influences disease progression, potentially leading to new therapeutic approaches in the treatment of CF.
Vagg went on to describe a study that suggested ML could aid in diagnosing post-transplant complications and refine immunosuppressive regimens. ML also has the potential to improve waiting list optimisation, and organ allocation, and predict patient graft survival. However, most current research is limited and does not really explore these applications in CF lung transplantation. “This gap presents a challenge but also a huge opportunity,” concluded Vagg.
Much like the advanced CFTR modulators described earlier, ML can be a useful tool in reshaping CF care, especially in areas like prognosis and lung transplantation. Expanding research and improving data quality will be key to unlocking its full potential.
CURRENT STATUS AND FUTURE CHALLENGES
Alberto Benazzo, Department of Thoracic Surgery, Medical University of Vienna, Austria, began with a brief history of CF, as it is important to understand the history of the disease to develop better treatments. The first lung transplantation in patients with CF occurred in the late 1980s marking lung transplantation as the standard of care for patients with an advanced stage of lung disease. The steep rise in CF transplantation rates was then stabilised by the introduction of a multidisciplinary approach, which improved the management of this disease in patients.
Early challenges in managing this disease included managing infections, malnutrition, and severe respiratory conditions. The development of extracorporeal membrane oxygenation devices and CO2 removal devices allowed patients to receive transplants safely, even when critically ill. As a result of all these efforts, patients with CF now experience some of the best transplant outcomes, in all underlying conditions, as shown by the data from international registries and single centres like the Toronto Transplant Group.
The introduction of CFTR modulators in 2019 changed the landscape for the disease. Two studies1,5 investigated the efficacy of triple therapy CFTR modulators in people with cystic fibrosis, with a F508del mutation, and demonstrated excellent results, this led to a dramatic decrease in the number of lung transplants and mortality.
These developments pose some questions for the future, one of them being whether lung transplantation will simply be postponed in patients with CF. Benazzo mentioned that further postponement of lung transplantation will come with a higher burden of concomitant diseases like complications of diabetes mellitus, cardiovascular disease, osteoporosis, and cancer. Another question is whether lung transplant patients will be eligible for ETI, specifically patients with mutations that are not approved for CFTR modulators. Benazzo described a case from his centre, a 17-yearold patient with an N1303k mutation and a heterozygous carrier for alveolar microlithiasis, and CF-related comorbidities. The patient was initially on antibiotic therapy every 10 weeks. A healing attempt was initiated with ETI, whereby her weight and lung function improved, and she was never listed for a lung transplant.
According to Benazzo, the case of this patient and descriptions in several studies like the Burgel et al.6 demonstrate that patients with mutations that are not FDAapproved for CFTR can still benefit from this specific treatment. However, some cases that present severe haemoptysis or with rare mutations may still necessitate transplants.
In conclusion, CF lung transplantation has achieved excellent outcomes throughout years of multidisciplinary work, but the advent of CFTR modulators poses a new challenge in determining which patients will require transplants in the future.
CONCLUSION
The evolution of care, marked by novel therapies and technology, is transforming the landscape of lung transplantation.
While the need for transplants has decreased significantly due to improved patient outcomes, ongoing research and innovations will be essential in identifying which patients with CF still require lung transplantation. As CF care continues to evolve, maintaining expertise in highvolume transplant centres and leveraging emerging tools like machine learning will be key to improving care and ensuring successful outcomes for all patients.
The advent of CFTR modulators poses a new challenge in determining which patients will require transplants in the future
References
1. Middleton PG et al. ElexacaftorTezacaftor-Ivacaftor for Cystic Fibrosis with a Single Phe508del Allele. N Engl J Med. 2019;381(19):1809-19.
2. Filipow N et al. Unsupervised phenotypic clustering for determining clinical status in children with cystic fibrosis. Eur Respir J. 2021;58:2002881.
3. Campredon A et al. Using chest computed tomography and
unsupervised machine learning for predicting and evaluating response to lumacaftor–ivacaftor in people with cystic fibrosis. Eur Respir J. 2022;59:2101344.
4. Zhao et al. Microbiome data enhances predictive models of lung function in people with cystic fibrosis. J Infect Dis. 2020;233(12 Suppl 2):S246-56.
5. Heijerman et al. Efficacy and safety of the elexacaftor plus tezacaftor plus ivacaftor combination regimen in people with cystic fibrosis
homozygous for the F508del mutation: a double-blind, randomised, phase 3 trial. The Lancet. 2019;384(10212):1940-8.
6. Burgel PR et al. The expanded French compassionate programme for elexacaftor-tezacaftor-ivacaftor use in people with cystic fibrosis without a F508del CFTR variant: a real-world study. Lancet Respir Med. 2024;DOI:10.1016/S22132600(24)00208-X.
Emerging Concepts in Bronchiectasis: Diagnosis, Pathophysiology, and Relevance in Lung Disease
This industry symposium took place during the European Respiratory Society (ERS) Congress held in Vienna, Austria on 7th–11th September 2024.
Chairperson:
Georg-Christian Funk,1,2 Eva Polverino3
Speakers: Marc Miravitlles,3 Luca Richeldi,4 Franziska Trudzinski,5 Alice Turner,6 Eva Polverino1,2
1. Karl Landsteiner Institute for Lung Research and Pulmonary Oncology, Vienna, Austria
2. Medical Pneumology Department, Klinik Ottakring, Vienna, Austria
4. A. Gemelli Hospital and Catholic University of the Sacred Heart, Rome, Italy
5. Thoraxklinik, University Hospital Heidelberg, Germany
6. School of Health Sciences, University of Birmingham, UK
Disclosure: Funk has received scientific grants, congress invitations, or speaker/ consultant fees from Amgen, Astra Zeneca, Bristol Myers Squibb, Boehringer Ingelheim, Chiesi, CSL Behring, Daiichi Sankyo, Draeger, Eli Lilly, Fresenius Kabi, Getinge, Gruenenthal, GSK, Insmed, Janssen-Cilag, Linde, MedAhead, MedMedia, Menarini, MSD, Novartis, Orion Pharma, Pfizer, Roche, Sanofi Genzyme, Takeda, Vifor, and Vivisol. Polverino has received a research grant from Grifols; speaker/consultancy fees from Chiesi, CSL Behring, GSK, Grifols, TEVA, Insmed, Pfizer, Vertex, Medscape, Moderna, AN2 Therapeutics, Gilead, Electromed, and Zambon; and travel to ERS International Congress 2024 was provided by CSL Behring. Miravitlles has received speaker fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GSK, Glenmark Pharmaceuticals, Menarini, Kamada, Takeda, Zambon, CSL Behring, Specialty Therapeutics, Janssen, Grifols, and Novartis, consulting fees from AstraZeneca, Atriva Therapeutics, Boehringer Ingelheim, Beam Therapeutics, BridgeBio, Chiesi, GSK, CSL Behring, Ferrer, Inhbrix, Menarini, Mereo Biopharma, Spin Therapeutics, Specialty Therapeutics, Palobiofarma SL, Takeda, Novartis, Novo Nordisk, Sanofi/Regeneron, Zambon, Zentiva, and Grifols; and research grants from Grifols. Richeldi is affiliated with, has a financial interest in, or has received grants or research support from Biogen, Boehringer Ingelheim, Celgene, DevPro Biopharma, FibroGen, Galapagos, Gilead, Novartis, Promedior, Respivant Sciences, Roche, Takeda, and UCB; has received honoraria or consultation fees from Boehringer Ingelheim, Cipla, Roche, and Zambon; has participated in a company-sponsored bureau for Acceleron, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Chiesi, CSL Behring, DevPro Biopharma, FibroGen, Forsee Pharmaceuticals, Liminal BioSciences, Nitto BioPharma, Pliant Therapeutics, Promedior, Respivant Sciences, Roche, Sanofi-Aventis, Veracyte, and Zambon; and travel to ERS International Congress 2024 was provided by CSL Behring.
Trudzinski is affiliated with, has a financial interest in, or has received grants or research support from AstraZeneca, Berlin-Chemie, Boehringer Ingelheim, Chiesi, CSL Behring, GSK, Grifols, Novartis, Pfizer, and STREAMED UP; has received honoraria or consultation fees from Boehringer Ingelheim, Chiesi, CSL Behring, and Grifols; and travel to ERS International Congress 2024 was provided by CSL Behring. Turner is affiliated with, has a financial interest in, or has received grants or research support from AstraZeneca, Chiesi, CSL Behring, Grifols, GSK, Takeda, and Vertex Pharmaceuticals; has received honoraria or consultation fees from AstraZeneca, Beam Therapeutics, Boehringer Ingelheim, CSL Behring, Grifols, GSK, Inhibrx, and Takeda; and has received sponsorship for conference attendance within the last 3 years from CSL Behring, AstraZeneca, and Grifols.
Acknowledgements: Writing assistance was provided by Nicola Humphry, Nottingham, UK.
Support: The publication of this article was funded by CSL Behring. The views and opinions expressed are exclusively those of the speakers.
Meeting Summary
This symposium took place during the 2024 European Respiratory Society (ERS) Congress held in Vienna, Austria. The main objective was to discuss the clinical aspects, diagnosis, and pathophysiology of bronchiectasis, a chronic, abnormal dilation of the bronchi, and its association with other lung diseases. The current understanding of the characteristics and prevalence of bronchiectasis in patients with chronic obstructive pulmonary disease (COPD) and alpha 1 antitrypsin (AAT) deficiency was discussed, as well as the relationship between the extent of traction bronchiectasis and exacerbations in idiopathic pulmonary fibrosis (IPF). The overarching message from the symposium was that advances are being made in elucidating the pathophysiology of bronchiectasis, and this is helping clinicians to understand why it occurs in patients with COPD and AAT deficiency. Increased characterisation of bronchiectasis is needed, including the understanding of its aetiology, disease development and progression, and the role of biomarkers in clinical management. This may help to identify treatable traits leading to personalised therapy with anti-inflammatory and antimicrobial drugs in the future.
Clinical Aspects and Diagnosis of Bronchiectasis
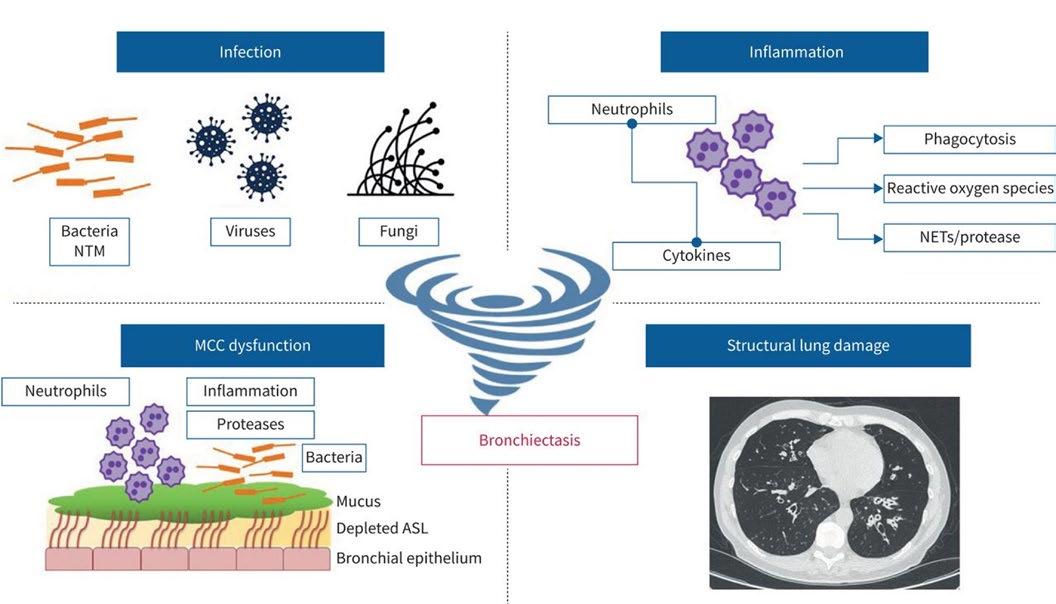
Bronchiectasis is a clinical condition defined as a chronic, abnormal dilation of the bronchi accompanied by classical symptoms.1,2 While the disease typically develops from chronic airway inflammation and/or infection, it has multiple aetiologies (excluding cystic fibrosis, which is considered a separate clinical entity) that
can be associated with several different conditions (Figure 1).1,3
International consensus recommendations indicate that the diagnosis of clinically significant bronchiectasis as a disease requires both radiological and clinical criteria, such as a persistent cough and sputum production, and a history of exacerbations.3 On CT, bronchiectasis appears as a dilation of the bronchus
PHARMA
relative to the accompanying pulmonary artery, with a lack of tapering, bronchial wall thickening, and the presence of visible bronchi within 1 cm of the pleural surface.2
Franziska Trudzinski, a Senior Clinical Consultant at Heidelberg University, Germany, stressed that all patients with bronchiectasis should undergo an aetiological workup, which includes a review of their medical history, clinical findings, and radiological findings, and a “minimum bundle” of laboratory tests. The minimum bundle of aetiological tests recommended by the ERS for adults with a new diagnosis of bronchiectasis includes differential blood count to detect primary or secondary immunodeficiency, serum immunoglobins (total IgG, IgA, and IgM), and testing for allergic bronchopulmonary aspergillosis (ABPA).5 Trudzinski uses these three inexpensive tests, along with a test for AAT levels, to detect those causes of bronchiectasis that require a specific treatment in her patients, such as humoral immunodeficiencies or ABPA.
Patients also benefit from further examinations at a specialised centre if they are younger or have severe or rapidly progressing disease.5 For example:5,6
• sequential daily sputum cultures or a bronchoalveolar lavage should be considered if non-tuberculous mycobacteria are suspected;
• sweat chloride, other biomarkers, or genetic testing should be considered if cystic fibrosis is suspected;
• nasal nitric oxide, high-speed video analysis, transmission electron microscopy, immunofluorescence, and/or genetic testing should be considered if primary ciliary dyskinesia is suspected; and
• AAT serum levels, phenotyping, and/or genotyping should be considered if AAT deficiency is suspected.
Trudzinski emphasised that following the ERS recommendations can help to understand the aetiology of bronchiectasis,
and can lead to relevant changes in treatment and prognosis.5 However, she explained that once bronchiectasis has been accurately diagnosed, additional CT scans are rarely useful unless the clinical manifestations of the disease have changed considerably; in patients with relatively stable disease, Trudzinski tends to perform a CT scan every five years (Trudzinski, personal communication).
She also stressed that a better understanding of the underlying pathology of bronchiectasis in different conditions is needed to enable clinicians to better tailor treatments to each patient’s disease rather than focussing purely on symptoms.
Bronchiectasis: State-of-the-Art
Eva Polverino, a Pulmonologist Expert in Respiratory Infections at the University Hospital Vall d’Hebron and VHIR, Barcelona, Spain, emphasised the heterogeneity of bronchiectasis. There are over 15 known causes of the disease (Figure 1); and bronchiectasis can be associated with other conditions such as COPD, rheumatoid arthritis, and severe asthma.7 In addition to cough and sputum production, clinical manifestations can include respiratory infections, lung function decline, and signs and symptoms of comorbidities.7 Accordingly, potential therapeutic options for the management of bronchiectasis vary and may include macrolides, pulmonary rehabilitation, long-acting bronchodilators, or inhaled corticosteroids (in patients with comorbid asthma).7
Bronchiectasis has long been understood to involve a ‘vicious cycle’ of host-mediated, inflammatory tissue damage and infection.8 However, Polverino explained that an infection of the respiratory tract is no longer considered to be the only trigger that can precipitate this cycle.
A more current view of the pathophysiology of bronchiectasis includes drivers such as airway inflammation, systemic inflammation, or genetic factors (Figure 2).7,9,10 Because the pathogenesis is more complex than was
previously thought, Polverino stressed the need for a more personalised approach to treatment.
Over a single year, half of patients with bronchiectasis in Europe experience two or more exacerbations, with approximately 25% of patients requiring at least one hospitalisation.11 Chronic infection in bronchiectasis involves immune dysregulation and is associated with a higher risk of exacerbations and hospitalisations, and reduced quality of life.12
The innate immune defence system carefully balances tissue repair, infection clearance, and injury resolution with the tissue damage that inflammation can cause. This balance requires the careful regulation of proteases (e.g., neutrophil elastase) and antiproteases (e.g., AAT).13 In bronchiectasis, dysregulation of this system tips the balance in favour of progressive tissue damage.13
In most cases of bronchiectasis, the disease is driven by neutrophilic inflammation,10,14 and a Phase II trial of an inhibitor of dipeptidyl peptidase 1, an enzyme that activates neutrophil proteases, resulted in fewer exacerbations and less sputum neutrophil elastase.15 Nevertheless, in about 20% of bronchiectasis patients eosinophil inflammation has been detected in the airways and has to be further addressed by future research to identify specific therapies.16
In addition to local inflammation, chronic respiratory disease can be associated with varying levels of systemic inflammation. Polverino explained that increasing evidence suggests systemic inflammation can be involved in bronchiectasis, and in some rare cases, this could be the driving factor in patients with rheumatoid arthritis or inflammatory bowel disease.7
Polverino stressed that real-world studies of bronchiectasis are incredibly important, particularly because of the diversity in patient demographics and healthcare systems. The European Multicentre Bronchiectasis Audit and Research Collaboration (EMBARC) registry has generated considerable real-world data on the aetiological distribution of bronchiectasis. Huge differences have also been described in terms of local microbiology, for instance, in Southern Europe (Spain, etc.), there is a preponderance of Pseudomonas aeruginosa among patients with bronchiectasis, whereas Haemophilus influenzae is more common in Northern and Western Europe.11
AIRWAY INFLAMMATION
• Neutrophilic
• Eosinophilic
• Other
SYSTEMIC INFLAMMATION
• Auto-immunity
• Auto-inflammatory
• Immune deficiency
EMBARC data has also estimated the prevalence of COPD and asthma among patients with bronchiectasis.17,18 Polverino emphasised that real-world data are invaluable for understanding the aetiology of the disease and determining how best to manage it in different geographical regions.
Polverino described a promising future for bronchiectasis management, with increased characterisation of the disease, through aetiology and biomarkers; personalised therapy with anti-inflammatory and antimicrobial drugs; and improved prevention through monitoring and immunisation, particularly in children at risk (Polverino, personal communication).
Bronchiectasis and Exacerbations in Chronic Obstructive Pulmonary Disease
There is a high prevalence of bronchiectasis among patients with COPD, although figures vary considerably between studies
(4–72%).1 Marc Miravitlles, a Pulmonologist and Senior Researcher at the University Hospital Vall d’Hebron and Vall d’Hebron Research Institute (VHIR), Barcelona, Spain, explained that his own experience suggests the true prevalence of bronchiectasis is likely to be between 30–50% of patients
Figure 2: Pathophysiology of bronchiectasis.7,9,10
COPD severity
with COPD. The presence of both conditions can be defined as the clinical COPD phenotype: COPD-bronchiectasis.1 However, he stressed the importance of differentiating the co-occurrence of bronchiectasis and COPD from bronchiectasis with airflow obstruction, which represents a purely bronchiectasis-based disease (Miravitlles, personal communication).
The European consensus definition of COPD-bronchiectasis, developed through a Delphi process by the EMBARC Airways Working Group, is the coexistence of four criteria, represented by the acronym, ‘ROSE’:19
• Radiology: abnormal bronchial dilatation, airways visible within 1 cm of pleura and/ or lack of tapering sign in one or more pulmonary segment and in more than one lobe.
• Obstruction: a spirometry pattern of forced expiratory volume in 1 second/ forced expiratory volume <0.7.
• Symptoms: at least two characteristic symptoms from cough, expectoration, dyspnoea, fatigue, and frequent infections.
• Exposure: current or past exposure to smoke (≥10 pack-years) or other toxic agents (e.g., biomass).
Bronchiectasis in patients with COPD is usually cylindrical, bilateral, and basal, with moderate severity scores in radiological analysis.1 Patients with severe COPD are consistently more likely to have bronchiectasis than those with moderate COPD,1 and the probability is also higher in patients with potentially pathogenic microorganisms (PPM) isolated from sputum, and those with a greater number of hospital admissions in the previous year (Figure 3).20
Isolation of PPM in sputum
Adapted from Martínez-García et al. 2011.20
COPD: chronic obstructive
Figure 3: Probability of the presence of bronchiectasis by patient characteristics.
Miravitlles explained that it is biologically plausible that COPD itself could cause bronchiectasis.1 Impaired immunity in COPD facilitates the survival and proliferation of PPMs in the lower airways, which can result in persistent bronchial inflammation. Together, chronic infection and inflammation can damage the bronchial wall and impair mucociliary clearance, leading to the vicious cycle of bronchiectasis.1 This evolution of COPD into a COPDbronchiectasis phenotype could be driven by genetic predisposition, environmental factors, response to antibiotic treatment, and/or immune response.1 In Miravitlles’ opinion, bronchiectasis can develop as a consequence of COPD in those patients who experience frequent exacerbations, bacterial infection, and increased inflammation over the course of their COPD, due to the bronchial damage they sustain. On the other hand, Trudzinski explained that in patients who develop bronchiectasis in childhood and are then exposed to environmental triggers, COPD may develop as a secondary disease. (Trudzinski, personal communication).
The presence of bacteria in the lungs is associated with inflammation in a doseresponse relationship; higher bacterial loads are associated with a higher intensity of inflammation and more frequent exacerbations.21 Miravitlles considers chronic bronchial infection to be the primary factor associated with both symptoms and poor outcomes in bronchiectasis, but he pointed out that frequent and severe exacerbations are also associated with a poor prognosis in COPD in general. He concluded that bacteria are likely be a foundation for the pathogenesis of bronchiectasis in COPD.
The best way to understand the natural history of bronchiectasis in COPD is by building large, international registries to collect information from a large population of patients. Miravitlles stressed that observational studies have helped to identify several factors associated with the development of bronchiectasis in COPD including: the frequency of severe exacerbations; the presence of bacteria in the lower airways, both during
exacerbations and in the stable state; and the presence of purulent sputum.22-24 He explained that patients with these factors are at increased risk of developing bronchiectasis or of worsening existing bronchiectasis.
A prospective, observational, cohort study in Spain followed patients with moderateto-severe COPD for around 8.5 years (102 months).22 Of the 77 patients who had at least two high-resolution CT scans for comparison, 16.9% had bronchiectasis that worsened, and 19.5% developed new bronchiectasis.22 Predictive factors for the progression or emergence of bronchiectasis in COPD included chronic mucopurulent/ purulent sputum (adjusted hazard ratio [aHR]: 2.8; p=0.023), the number of PPM isolations (aHR: 1.1; p=0.011), and number of hospitalisations (aHR: 1.2; p=0.2).22 The presence of bronchiectasis in patients with COPD has also been associated with inflammatory cytokines in the sputum, poor lung function, exacerbations, and isolation of P. aeruginosa. 23,24
Another prospective, observational study in patients with moderate-to-severe COPD found that bronchiectasis was associated with an increased risk of mortality in this population (HR: 2.54; p=0.02).25 The isolation of P. aeruginosa in patients with COPD is also linked with increased mortality (aHR: 1.95), and multiple isolates of P. aeruginosa have been associated with the presence of bronchiectasis and severe exacerbations.26,27
The sputum microbiome and protein profile in patients with COPD-bronchiectasis largely overlap with those in patients with bronchiectasis alone.28 However, compared with patients with COPD alone, those with COPD-bronchiectasis exhibit a greater abundance of proteobacteria, higher expression of mucin-5AC and proteins from the neutrophil degranulation pathway, lower expression of mucin-5B and peptidase inhibitors, and greater microbiome diversity.28
Understanding disease phenotypes in bronchiectasis is important because treatment strategies are based on the
patient’s symptoms and risk factors.28 For example, Miravitlles considers frequent exacerbations to be the most important aspect of the disease due to the association with poor quality of life and reduced survival. In patients with frequent exacerbations, treatment strategies should be implemented to reduce their frequency and severity. Alternatively, if a patient is not a frequent exacerbator but has a chronic cough and sputum, or is short of breath, then treatment should aim to alleviate these symptoms.
Miravitlles summarised the hallmarks of bronchiectasis in patients with COPD as increased sputum production, recurrent infections, and frequent exacerbations. He stressed that a chest CT scan is recommended in these cases.29 The identification of treatable traits of COPD, such as AAT deficiency, chronic bronchial infection, and bronchiectasis, allows specific treatment to be tailored to individual patient needs.30
Same But Different? Bronchiectasis in AAT Deficiency
AAT deficiency is associated with unopposed protease activity, which drives an inflammatory cascade, resulting in enhanced airway inflammation. This represents a potential risk factor for the development of bronchiectasis.31-33
Despite this potential, Alice Turner, a Senior Clinical Lecturer in Respiratory Medicine at the University of Birmingham, UK, emphasised that the literature is unclear about whether an association exists between these two diseases.
Some studies have shown an increased prevalence of bronchiectasis in patients with AAT deficiency (9–27%) compared with the general population,31,33 and the prevalence of AAT deficiency among patients with bronchiectasis is similar to that observed for other genetic causes of bronchiectasis.33
However, prevalence estimates vary widely,34-36 bronchiectasis occurs at a
similar frequency to usual COPD, suggesting that bronchiectasis is a secondary development,20,37 and there is no evidence of an allelic association.38
One reason for the lack of clarity regarding bronchiectasis in AAT deficiency is that several studies were of low quality, with heterogenous reporting, making it difficult to perform a meta-analysis.39
A recent analysis was conducted on data from the first 564 patients recruited to the European Alpha 1 Research Collaboration (EARCO) International Registry for whom a CT scan was performed.32 The data showed that bronchiectasis (with or without emphysema) was identified in 189 patients (34%), and 55 (9.8%) had bronchiectasis alone. However, it was also noted that forced expiratory volume in 1 second appeared to be impaired more by emphysema and smoking history than by bronchiectasis.32
Turner reported data from a recent study in 1,232 patients with AAT deficiency in Birmingham, UK.40 Among these patients, 235 (19.1%) had a diagnosis of bronchiectasis and 30 (2.4%) had a diagnosis of bronchiectasis without COPD. The prevalence of bronchiectasis was greater among patients with the severe deficiency PiZZ genotype of AAT deficiency than those with the milder PiSZ genotype (patients with PiZZ had significantly higher numbers of affected lobes; p=0.009).40 Even among those patients without COPD, bronchiectasis was still found to be associated with the PiZZ genotype (p=0.016), as well as with reduced serum AAT levels and poorer dyspnoea scores (Turner, personal communication).
However, no association was found between bronchiectasis and lung function decline measures or exacerbation rate,40 and Turner speculated that this may be because bronchiectasis is such a heterogeneous disease. Heterogeneity of bronchiectasis in AAT deficiency was shown by the broad range of individual patient scores in the Birmingham cohort using the validated Bronchiectasis Severity Index (BSI) scoring system.40
Mild bronchiectasis was predominant among those patients with AAT deficiency who were diagnosed with the disease, and bronchiectasis was even detected in CT scans from several of the patients in the control group who had not been diagnosed with bronchiectasis.40 Turner recommended that clinicians consider reviewing CT scans for patients with AAT deficiency to look for evidence of bronchiectasis.
In the Birmingham cohort, the majority (approximately 45%) of patients had cylindrical bronchiectasis morphology. Fifteen patients had the generally more severe cystic morphology, which was associated with a greater decline in the carbon monoxide transfer coefficient, and an increase in exacerbation rate compared with other morphologies.40
Of 994 sputum samples from patients with AAT deficiency, 61% showed evidence of bacterial colonisation, which is more common in patients with bronchiectasis (73%) than in those without (56%; Spittle, et al. Submitted for publication). The presence of colonising bacteria also appears to be associated with the rate of exacerbations.41 Studies to characterise the microbiome in AAT deficiency are ongoing, and it is expected that new data will help to define new phenotypes to explain the diversity of clinical presentations of lung disease in AAT deficiency.41,42
Turner concluded that, in some ways, bronchiectasis patients with AAT deficiency have similar characteristics to those in patients with COPD. However, the prognosis of patients with AAT deficiency with bronchiectasis is less clear, and there seems to be a greater heterogeneity of disease among these patients than is observed in patients with bronchiectasis alone.40
In terms of pathophysiology, early data suggest an association between AAT levels and bronchiectasis, and Turner explained that since bronchiectasis is also seen in patients without COPD, it is possible that reduced levels of AAT could be driving this pathology.43 In addition, polymers of AAT, often found in the circulation of patients with PiZZ AAT deficiency, can be
considered pro-inflammatory and potentially chemotactic for neutrophils,44 and Turner speculated that these polymers could contribute to the vicious cycle of pathology in bronchiectasis.
Further radiological studies are needed to determine whether the morphological and microbiome data reported from the Birmingham AAT deficiency cohort can be replicated in other groups, and Turner stressed that we also know little about the drivers of exacerbations in AAT deficiency.
Bronchiectasis and Exacerbations in Idiopathic Pulmonary Fibrosis
On a CT scan, bronchiectasis with evidence of thickened, irregular bronchial walls (‘traction’ bronchiectasis) is an indicative feature of the usual interstitial pneumonia (UIP) pattern, which is typical of IPF, a progressive, life-threatening, interstitial lung disease of unknown aetiology.2,45,46 The rate of decline in patients with IPF can take different forms, including a slow physiologic deterioration, periods of relative stability interposed with periods of acute respiratory decline (exacerbations), or rapid deterioration.46 The occurrence of acute exacerbations in IPF is associated with a substantially increased risk of mortality.47
Luca Richeldi, Professor of Respiratory Medicine at the Catholic University of the Sacred Heart and Head of Pulmonology at the Gemelli Hospital in Rome, Italy, explained that the extent of traction bronchiectasis and/or honeycombing in CT may be a prognostic biomarker in fibrotic interstitial lung diseases (ILD) such as IPF.48 Among 209 patients with ILD, the risk of disease progression at 1 year was associated with both traction bronchiectasis and/or honeycombing (odds ratio: 8.54; p=0.19), and with raised levels of monocytes (odds ratio: 3.16; p=0.014).48 These three key variables commonly cooccurred in patients and were used to develop a validated scoring system for risk of progression in ILD: the honeycombing, traction bronchiectasis, and monocyte (HTM) score.48
In traction bronchiectasis, Richeldi stressed that inflammation is less relevant to disease compared to bronchiectasis in COPD. He explained that the role of inflammation remains controversial in IPF, and the main factor contributing to disease is fibrosis. For this reason, Richeldi feels that using purely inflammatory markers to monitor disease progression in IPF is unlikely to be clinically helpful.
Richeldi stressed that the treatment of acute exacerbations in IPF remains largely empirical and is not based on evidence.49 Currently, the best treatment for acute exacerbations is to avoid them by reducing disease progression.
Summary
The key messages among the emerging diagnostic and therapeutic concepts for inflammation in rare lung diseases discussed at this symposium were:
• The diagnosis of clinically significant bronchiectasis requires both clinical and radiological criteria, with further examinations at a specialised centre for younger patients, or those with severe or rapidly progressing disease.
References
1. Martínez-García MÁ, Miravitlles M. Bronchiectasis in COPD patients: more than a comorbidity? Int J Chron Obstruct Pulmon Dis. 2019;18;14:245. Corrected and republished from: Int J Chron Obstruct Pulmon Dis. 2017;12:1401-11.
2. Bankier AA et al. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2024;310(2):232558.
3. Aliberti S et al. Criteria and definitions for the radiological and clinical diagnosis of bronchiectasis in adults for use in clinical trials: international consensus recommendations. Lancet Respir Med. 2022;10(3):298-306.
4. Chan ED et al. Diagnostic evaluation of bronchiectasis. Respir Med X. 2019;1:100006.
• Many different underlying diseases are associated with bronchiectasis. The future is characterisation, personalised therapy, and addressing inflammation, infection, and prevention.
• Greater severity of COPD is associated with a higher prevalence of bronchiectasis, and the presence of bronchiectasis is associated with poorer prognosis.
• Bronchiectasis is not always reported on a CT scan for a patient with AAT deficiency. However, there is some evidence of an association between these two diseases, and a high rate of bacterial colonisation in the lung is associated with exacerbation risk.
• The risk of acute exacerbations in IPF correlates with the severity of the disease, i.e., the extension of honeycombing and traction bronchiectasis. The best treatment is currently to avoid acute exacerbations by reducing disease progression.
Trudzinski stressed that, currently, bronchiectasis is sometimes improperly reported, and that artificial intelligence is likely to be important in the future to better establish diagnostic criteria and markers of disease progression.
5. Polverino E et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur Respir J. 2017;50(3):1700629.
6. Miravitlles M et al. European Respiratory Society statement: diagnosis and treatment of pulmonary disease in α1-antitrypsin deficiency. Eur Respir J. 2017;50(5):1700610.
7. O’Donnell AE. Bronchiectasis - a clinical review. N Engl Med J. 2022;387(6):533-45.
8. Cole PJ. Inflammation: a two-edged sword--the model of bronchiectasis. Eur J Respir Dis Suppl. 1986;147:6-15.
9. Keir HR, Chalmers JD. Pathophysiology of bronchiectasis. Semin Respir Crit Care Med. 2021;42(4):499-512.
11. Chalmers JD et al. Bronchiectasis in Europe: data on disease characteristics from the European Bronchiectasis registry (EMBARC). Lancet Respir Med. 2023;11(7):637-49.
12. Mac Aogáin M et al. Infection and the microbiome in bronchiectasis. Eur Respir Rev. 2024;33(173):240038.
13. Polverino E et al. The role of neutrophil elastase inhibitors in lung diseases. Chest. 2017;152(2):249-62.
14. Chalmers JD et al. Neutrophil elastase activity is associated with exacerbations and lung function decline in bronchiectasis. Am J Respir Crit Care Med. 2017;195(10):1384-93.
10. Chalmers JD et al. Basic, translational and clinical aspects of bronchiectasis in adults. Eur Respir Rev. 2023;32:230015.
15. Chalmers JD et al. Phase 2 trial of the DPP-1 inhibitor brensocatib in bronchiectasis. N Engl J Med. 2020;383(22):2127-37.
16. Shoemark A et al. Characterization of eosinophilic bronchiectasis: a European multicohort study. Am J Respir Crit Care Med. 2022;205(8):894-902.
17. Polverino E et al. Bronchiectasis and asthma: data from the European Bronchiectasis Registry (EMBARC). J Allergy Clin Immunol. 2024;153(6):1553-62.
18. Polverino E et al. The association between bronchiectasis and chronic obstructive pulmonary disease: data from the European Bronchiectasis Registry (EMBARC). Am J Respir Crit Care Med. 2024;210(1):119-27.
19. Traversi L et al. ROSE: radiology, obstruction, symptoms and exposure – a Delphi consensus definition of the association of COPD and bronchiectasis by the EMBARC Airways Working Group. ERJ Open Res. 2021;7(4):00399-2021.
20. Martínez-García MÁ et al. Factors associated with bronchiectasis in patients with COPD. Chest. 2011;140(5):1130-7.
21. Miravitlles M. Exacerbations of chronic obstructive pulmonary disease: when are bacteria important? Eur Respir J Suppl. 2002;36:9s-19s.
22. Martínez-García MÁ et al. Bronchial infection and temporal evolution of bronchiectasis in patients with chronic obstructive pulmonary disease. Clin Infect Dis. 2021;72(3):403-10.
23. Patel IS et al. Bronchiectasis, exacerbation indices, and inflammation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2004;170(4):400-7.
24. Ni Y et al. Clinical characteristics of patients with chronic obstructive pulmonary disease with comorbid bronchiectasis: a systemic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2015;10:1465-75.
25. Martínez-García MÁ et al. Prognostic value of bronchiectasis in patients with moderate-to-severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187(8):823-31.
26. Martínez-García MÁ et al. Long-term risk of mortality associated with isolation of pseudomonas aeruginosa in COPD: a systematic review and meta-analysis. Int J Chron Obstruct
Pulmon Dis. 2022;17:371-82.
27. Martínez-García MÁ et al. Risk factors and relation with mortality of a new acquisition and persistence of pseudomonas aeruginosa in COPD patients. COPD. 2021;18(3):333-40.
28. Huang JT et al. Endotyping chronic obstructive pulmonary disease, bronchiectasis, and the “chronic obstructive pulmonary disease–bronchiectasis association”. Am J Respir Crit Care Med. 2022;206(4):417-26.
29. Agustí et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Eur Respir J. 2023;61(4):2300239.
30. Miravitlles M et al. Actualización 2021 de la Guía Española de la EPOC (GesEPOC). Tratamiento farmacológico de la EPOC estable. Arch Bronconeumol. 2022;58(1):69-81.
31. Parr DG. Prevalence and impact of bronchiectasis in a1-antitrypsin deficiency. Am J Respir Crit Care Med. 2007;176:1215-21.
32. Stockley RA et al. The prevalence of bronchiectasis in patients with alpha-1 antitrypsin deficiency: initial report of EARCO. Orphanet J Rare Dis. 2023;18(1):243.
33. Eden E et al. The clinical features of bronchiectasis associated with alpha-1 antitrypsin deficiency, common variable immunodeficiency and primary ciliary dyskinesia-results from the U.S. Bronchiectasis Research Registry. Chronic Obstr Pulm Dis. 2019;6(2): 145-53.
34. Aliberti S et al. Clinical phenotypes in adult patients with bronchiectasis. Eur Respir J. 2016;47(4):1113-22.
35. Pasteur MC et al. An investigation into causative factors in patients with bronchiectasis. Am J Respir Crit Care Med. 2000;162(4 Pt 1):1277-84.
36. Carreto L et al. Utility of routine screening for alpha-1 antitrypsin deficiency in patients with bronchiectasis. Thorax. 2020;75(7):592-93.
37. Agusti A et al. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res. 2010;11(1):122.
38. Cuvelier A et al. Distribution of alpha(1)-antitrypsin alleles in patients with bronchiectasis. Chest. 2000;117(2): 415-9.
39. De Soyza J et al. What are the radiological, microbiological and biochemical characteristics of bronchiectasis in alpha-1 antitrypsin deficiency? A systematic review. Abstract PA394. ERS International Congress. 9-13 September, 2023.
40. De Soyza J, et al. Bronchiectasis occurs independently of chronic obstructive pulmonary disease in alpha-1 antitrypsin deficiency. Chronic Obstr Pulm Dis. 2024;11(5):507-14.
41. Spittle D et al. Bacterial colonisation doubles the risk of exacerbation in subjects with alpha-1 antitrypsin deficiency (AATD)-related COPD. Abstract A2925. ATS International Conference. 17-22 May, 2024.
42. Strange C et al. Rationale and design of the genomic research in alpha-1 antitrypsin deficiency and sarcoidosis study. Alpha-1 protocol. Ann Am Thora Soc. 2015;12(10):1511-60.
43. Sanduzzi A et al. Alpha-1-antitrypsin deficiency and bronchiectasis: a concomitance or a real association? Int J Environ Res Public Health. 2020;17(7):2294.
44. Núñez A et al. Association between circulating alpha-1 antitrypsin polymers and lung and liver disease. Respir Res. 2021;22(1):283. Corrected and republished from: Respir Res. 2021;22(1):244.
45. Raghu G et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults an official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2022;205(9):e18-47.
46. Ley B et al. Clinical course and prediction of survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;183(4):431-40.
47. Paterniti MO et al. Acute exacerbation and decline in forced vital capacity are associated with increased mortality in idiopathic pulmonary fibrosis. Ann Am Thorac Soc. 2017;14(9):1395-402.
48. Shao G et al. Clinical, imaging, and blood biomarkers to assess 1-year progression risk in fibrotic interstitial lung diseases-Development and validation of the honeycombing, traction bronchiectasis, and monocyte (HTM)-score. Front Med (Lausanne). 2022;9:1043720.
49. Luppi E et al. Acute exacerbation of idiopathic pulmonary fibrosis: a clinical review. Intern Emerg Med. 2015;10(4):401-11.
Transforming Care in SEA: Evidence and Considerations for Evolution of the Current Treatment Paradigm
This symposium review article is based on an AstraZeneca-sponsored non-promotional symposium session that took place at the European Respiratory Society (ERS) Congress held in Vienna, Austria, between 7th–11th September 2024.
Chairperson: Stefano Del Giacco1
Speakers: Katrin Milger-Kneidinger,2,3 Felix Herth,4 Stephanie Korn,4,5 Stefano Del Giacco1
1. University of Cagliari, Sardinia, Italy
2. University Hospital at the Ludwig-Maximilian University (LMU), Munich, Germany
3. MedUni Graz, Austria
4. Thoraxklinik and Translational Lung Research Center Heidelberg, University of Heidelberg, Germany
5. Institute für klinische Forschung (IKP) Pneumologie, Mainz, Germany
Disclosure: Del Giacco declared no conflicts of interest. Milger-Kneidinger has been a speaker and/or served on the advisory board for AOP Orphan Pharmaceuticals, AstraZeneca, Chiesi Farmaceutici, GlaxoSmithKline (GSK), Insmed, Janssen, Novartis, and Sanofi. Herth has received research support from BMG Pharma, Broncus Medical, the European Union, the German Federal Ministry of Education and Research (BMBF), the German Research Foundation (DFG), Hardenberg-Stiftung Foundation, Klaus-Tschira Stiftung Foundation, Octapharma, Olympus Medical, Pulmonx, Roche Diagnostics, and Uptake Medical; has received speaker honoraria from AstraZeneca, Berlin Chemie, Boehringer Ingelheim, Chiesi Farmaceutici, Erbe Elektromedizin, GSK, Medupdate Europe, Novartis, Pulmonx, Roche Diagnostics, Streamed Up, and Uptake Medical; and has served as a consultant for AstraZeneca, Boston Scientific, Broncus Medical, Dinova, Eolo Pharma, Erbe Elektromedizin, Free Flow Medical, Johnson & Johnson, Karger Publishers, LÄK, Nanovation Therapeutics, Olympus Medical, Pulmonx, Roche Diagnostics, and Uptake Medical. Korn has received research support from AstraZeneca, Boehringer Ingelheim, Chiesi Farmaceutici, GSK, Novartis, Roche Diagnostics, and Sanofi; has received speaker honoraria and/or served as a consultant for AstraZeneca, Boehringer Ingelheim, Chiesi Farmaceutici, GSK, Novartis, Roche Diagnostics, and Sanofi.
Acknowledgements: Medical writing assistance was provided by Bjørn Hanger, EMJ, London, UK.
Disclaimer The non-promotional symposium was organised and funded by AstraZeneca. The information displayed during the meeting is exclusively for healthcare professionals. The purpose of the non-promotional symposium was for disease state awareness and is not meant to imply the efficacy or safety of any AstraZeneca products or other medications which are discussed. The Summary of Product Characteristics and prescribing information for benralizumab are available from: https://www. ema.europa.eu/en/documents/product-information/fasenra-epar-product-information_en.pdf.
Support: The symposium and publication of this article were organised and funded by AstraZeneca.
Meeting Summary
This article reviews an industry symposium held on 8 September 2024 as part of the European Respiratory Society (ERS) Congress 2024 in Vienna, Austria, which brought together four experts to discuss the current treatment paradigm for severe eosinophilic asthma (SEA), including the role of biologics and background medication tapering. Katrin Milger-Kneidinger, Professor of Respiratory Medicine at the University Hospital of the Ludwig Maximilian University Munich (LMU), in Germany, and the MedUni Graz, in Austria, explored the critical role eosinophils play in SEA pathology and how biologic therapies targeting eosinophils can address key disease features, including airway remodelling, airway hyperresponsiveness (AHR), and mucus production. Felix Herth, Professor of Pulmonary and Critical Care Medicine at Thoraxklinik Heidelberg, Heidelberg University Hospital, in Germany, discussed persistent airflow obstruction (PAO) in patients with SEA, focusing on a typical patient profile to understand the clinical manifestation and opportunities for management. Stephanie Korn, Professor of Pulmonary and Respiratory Medicine at Thoraxklinik Heidelberg, Heidelberg University Hospital, in Germany, and Head of the Clinical Research Centre, Institute für Klinische Forschung (IKP) Pneumologie in Mainz, Germany, presented on remission as a clinical target in SEA, focusing on how biologics can help achieve remission in some patients. Lastly, in a discussion led by symposium chair Stefano Del Giacco, Professor of Medicine, Allergy, and Clinical Immunology, at the University of Cagliari, Sardinia, in Italy, the experts agreed that a positive practice change would be to get more patients with relevant clinical manifestations on biologics, and that background medication tapering, when appropriate, could lead to improved patient outcomes and quality of life (QoL) in SEA.
Introduction
Asthma affects approximately 262 million people globally,1 with the number of asthma incidents having increased by around 15% over the last 29 years.2 Up to 10% of this population has severe asthma,3 which accounts for an estimated 50% of all asthma-related annual healthcare costs in Europe, accounted for by an increased hospitalisation rate.4,5 Of those with severe asthma, 84% of patients are likely to have an eosinophilic phenotype, termed SEA.6 Greater patient hospital costs are associated with patients with eosinophilic asthma versus other types of asthma.7
Clinically, eosinophilic asthma is associated with more frequent and severe exacerbations (two or more exacerbations annually), poor asthma control,8 with an increased risk of asthma-related hospitalisations, and poor QoL,7 reduced lung function (evidenced by low forced expiratory volume in 1 second [FEV1] and persistent airflow limitation),9–11 a higher likelihood of nasal polyps, asthma being adult-onset,6 steroid dependence,10 and death.10,12
Historically, the use of oral corticosteroids (OCS) has been common practice in treating severe asthma,13 but long-term use of
PHARMA
OCS carries significant health risks for patients with severe asthma.14 With these challenges in mind, the overarching aim of this symposium was to advance clinical practice in SEA and reduce the global burden of long-term background medications in partnership with healthcare professionals (HCP).
Latest Advances in Understanding the Critical Role of Eosinophils in Severe Asthma: A Key Driver of the Hallmarks of Disease
Katrin Milger-Kneidinger
Milger-Kneidinger shared the up-to-date evidence demonstrating the critical role of eosinophils in driving the key features of SEA, including remodelling, mucus plugging, and AHR.
Notably, the airway pathology of SEA is characterised by Type 2 eosinophilrich airway inflammation which causes epithelial damage and drives airway remodelling.15,16 Processes involved include goblet cell hyperplasia, mucus production, and smooth muscle contractility and hypertrophy.15,16 Clinically, this manifests in bringing about exacerbations, airway obstruction, clinical symptoms, and AHR.15,16 As such, elevated eosinophils remain one of the most important targets for SEA.
Targeting the IL-5 Pathway
Mitigating the cytotoxic effects of eosinophils by reducing systemic levels is a key treatment strategy in SEA.17–20 MilgerKneidinger highlighted that monoclonal antibodies targeting the IL-5 pathway are key to reducing eosinophil levels in those with asthma, through either binding with IL-5, such as mepolizumab and reslizumab, or interacting with the IL-5 receptor, such as with benralizumab.18,21 Milger-Kneidinger summarised data which indicate that benralizumab achieves a substantial eosinophil reduction, with ≥95% reduction in blood and sputum eosinophils, and 80–94% in the airway.18 Mepolizumab has demonstrated an 80–94% reduction
in blood eosinophils but <50% in sputum, and reslizumab demonstrated an 80–94% reduction in blood eosinophils and 50–79% in sputum.18 According to Milger-Kneidinger, the importance of reducing eosinophils in the airway with IL-5 antibodies, stating “improvement in clinical symptoms has been observed; however, some patients may have an incomplete response, with exacerbations.” She highlighted findings from the MEX study, a UK-based multicentre, prospective observational study that investigated why exacerbations still occur in those treated with mepolizumab.19 The study found that ~50% of exacerbations on mepolizumab occur in the context of ongoing airway eosinophilia, as seen by the sputum eosinophilia and fractional exhaled nitric oxide (FeNO) levels at the time of exacerbation.19
There is a complex interplay between airway inflammation, airway remodelling, and structural changes in SEA.22–24 In the context of airway inflammation, the severity of AHR correlates with eosinophil and mast cell numbers, though AHR can also occur independently of airway inflammation.25,26 On AHR association with airway remodelling and structural changes, Milger-Kneidinger said that it is an area of evolving research, noting “especially smooth muscle hypertrophy” as a contributor, and that “bronchoconstriction itself may lead to epithelial damage and inflammation, providing another important link in this complex interplay.”
Mucus production and mucus plugs, which likely contribute to persistent or fixed airway obstruction, are also potential features in SEA.27,28 Milger-Kneidinger reported that eosinophil peroxidase degranulation by eosinophils leads to mucin crosslinking, increasing its viscosity and forming mucus plugs.27,28 Higher levels of sputum eosinophils are associated with higher mucus scores, and higher levels of mucus plugs are associated with airway obstruction, as demonstrated by lower FEV1 over time,28 emphasising the role of eosinophils in this process.
Managing Mucus Plugging in Severe Asthma
When considering the treatment options for AHR, Milger-Kneidinger discussed the use of biologics and shared her experience from the German asthma network study.29,30,31
Treatment with biologics has been demonstrated to significantly attenuate airway challenge-induced AHR.30,31 Reducing eosinophil levels in the airways using biologics may also inhibit airway remodelling, reducing airway thickening.32,33 For example, mepolizumab reduces airway wall thickening by inhibiting airway remodelling markers, tenascin, lumican, and procollagen III,32 and benralizumab reduces airway smooth muscle mass by targeting IL-5 receptor-α.33
Treatment with biologics such as tezepelumab, mepolizumab, dupilumab, and benralizumab, has been linked to reductions or near-elimination of mucus plugs.34–37 Reductions in mucus plug scores are positively correlated with improved FEV1 percentage.38
Positive bronchodilator (BD) reversibility is a diagnostic criterion for asthma.31 However, as seen in the German asthma network study, two-thirds of patients exhibited a negative BD reversibility response.31 Positive BD reversibility was associated with low baseline predicted FEV1 percentage and chest tightness.31 Milger-Kneidinger shared that with regards to negative BD reversibility, rather than it being associated with chronic obstructive pulmonary disease (COPD) or smoking history, it was associated with lower FeNO and the presence of gastro-oesophageal reflux disease.31 Milger-Kneidinger then reported that treatment with anti-IL-5 or anti-IL-5R biologics can reduce OCS dependence, annualised exacerbation rates, and improve symptoms (reported with a positive change in asthma control test score) and lung function (reported by an increased FEV1) in patients with severe asthma, regardless of positive or negative BD reversibility.39 Milger-Kneidinger also reported that it may be possible to predict improvements in lung function, dependent on patient characteristics when considering the use
of biologics, as a higher initial mucus plug score increased the likelihood of having improvement in FEV1 following treatment.40
Milger-Kneidinger concluded that 1) eosinophils drive asthma pathology through airway inflammation, remodelling, and structural changes; 2) thorough eosinophil depletion is key to reducing the risk of eosinophilic-associated exacerbations; and 3) reducing eosinophils in SEA reduces AHR, airway wall thickening, and mucus plug formation.
A Focus on Persistent Airflow Obstruction in Severe Eosinophilic Asthma
Felix Herth
Herth identified that the understanding of the clinical traits and pathological mechanisms for asthma is still emerging,41-44 and therefore explored the latest evidence for the role of eosinophils in individuals with SEA with PAO and reviewed typical patient profiles to understand the clinical manifestation and opportunities for management.
PAO, a clinical phenotype seen in individuals with SEA, is defined as a postBD FEV1/FVC ratio of <0.7 and is thought to be due to airway wall remodelling.3 It may develop later in the asthma course, with Herth emphasising that some patients initially present with variable airflow obstruction.3 This phenotype is often confused with COPD.3,45
Key Risk Factors and Clinical Presentation in Developing Persistent Airflow Obstruction
Herth called for a need for improved awareness around the challenge of misdiagnosis of COPD for those that should have a diagnosis of SEA with PAO, presenting a case study of a 65-yearold female, ex-smoker with a previous diagnosis of COPD, who presented with increasing shortness of breath, cough, and exacerbations. Diagnostics demonstrated
poor lung function, specifically a pre-FEV1 of 0.72 L (29.6% predicted), post-FEV1 of 0.85 L (37.1% predicted), and residual volume of 190%. However, Herth highlighted the diffusion capacity testing with transfer factor of the lung for carbon monoxide was 76.3%, suggesting that further investigation was required and indicated SEA with PAO. These diagnostic challenges are problematic as PAO in asthma can, in some cases, be reversible with appropriate treatment, as observed in the case presented by Herth.3,45
Up to 23% of those with asthma have PAO, with it being most common in those with severe disease.46 Risk factors for developing PAO include older age, male sex,47 preterm birth and low birth weight, greater infant weight gain, chronic mucus hypersecretion, longer asthma duration, lack of inhaled corticosteroid (ICS) treatment, low initial FEV1, exposure to tobacco smoke, and environmental pollutants.3
Herth noted that those with asthma and PAO tend to have more severe symptoms48 and poorer outcomes49 such as reduced lung function,50,51 increased airway inflammation,50 risk of exacerbation,50,51 and mortality,52 compared to those with asthma without PAO.3,48-52 Contributing to the differences in clinical outcomes in patients with asthma and PAO compared to those without PAO is an association with increased sputum and blood eosinophils, higher monocyte counts in the blood, fewer macrophages in sputum, and a greater decline in lung function (FEV1).50,51 As such, remodelling of the airway epithelium, likely influenced by eosinophil-driven mucus production and plugging, as eluded by Milger-Kneidinger, also contributes to the pathophysiology of PAO.53-56
Management Options for Severe Eosinophilic Asthma with/without Persistent Airflow Obstruction
Biologics have shown to be of benefit to those with SEA, regardless of PAO status. Benralizumab significantly reduced annualised exacerbation rates (AER) (44% reduction in those with PAO status, and 42%
in those without PAO status) and improved pre-BD FEV1 (0.159 L increase in those with PAO status, and 0.103 L increase in those without PAO status) compared to placebo.57 Dupilumab similarly demonstrated improved AER and pre-BD FEV1 in patients with PAO and eosinophil levels of ≥150 cells/μL or FeNO at ≥25 parts per billion at baseline, and in patients with PAO and eosinophil levels of ≥300 cells/μL and FeNO at ≥25 parts per billion at baseline when compared to placebo.49 Tezepelumab and omalizumab also reduced annualised AER over 52 weeks compared to placebo in patients with and without PAO, although, as reported by Herth, a study on omalizumab has highlighted a potentially difficult-to-treat group in patients with or without PAO but low BD responsiveness.58,59
Herth emphasised that as PAO is a distinct clinical phenotype characterised by irreversible airflow obstruction, there is a need to be aware of the misdiagnosis of COPD. Herth summarised that patients with asthma and PAO generally experience worsening outcomes compared to those without PAO, and that airway remodelling plays a critical role in the development of PAO, with biologics demonstrating improved symptom control and reduced exacerbations in patients with asthma and PAO.
Remission as a Clinical Target for Severe Eosinophilic Asthma
Stephanie Korn
Stephanie Korn shifted the focus to remission as a clinical target in SEA, focusing on the value of targeting clinical remission for patients compared with traditional treatment goals.
To define remission in asthma, several components must be met. These have been adopted by other conditions with chronic inflammation, and include key components for improvements in clinical outcomes, QoL, and productivity, as well as a composite of signs, symptoms, and biomarkers of disease.60-65 Although international asthma guidelines vary slightly, they all agree that
the absence of exacerbations, along with no systemic steroids for treatment, are essential for defining remission.3,66,67 Korn mentioned a need to establish consensus for defining minimal or no symptoms and lung function. Key variances across guidelines include symptoms, stable lung function, and the number of missed school/ work days.3,66,67
In clinical trials, remission is typically defined using four key criteria: 1) Daily symptoms (e.g., Asthma Control Questionnaire-6 [ACQ-6] score <1.5 or ≤0.75); 2) zero asthma exacerbations 3) zero OCS use; and 4) stabilisation or improvement in lung function as indicated by pre-BD FEV1 68,69 Korn presented posthoc analysis data from the SHAMAL trial, a trial on biologic benralizumab where patients with SEA were allowed to reduce their background medication.70,71 The majority of patients enrolled in SHAMAL achieved three- or four-components of the response endpoints with clinical remission at Week 32, with the three-component criteria excluding stable lung function.70 Four-component clinical remission was achieved less frequently than threecomponent clinical remission, particularly in participants with inhaled corticosteroid/ formoterol (ICS/FORM) stepdown.70 As such, for patients with SEA controlled on benralizumab, achieving clinical remission after ICS/FORM reduction is feasible, although Korn highlighted that there is a need for monitoring for worsening/ exacerbations during ICS/FORM dose reduction.
Real-world data from XALOC-1 and XALOC-2 also demonstrated remission rates in patients with uncontrolled SEA.72,73 In XALOC-1, 60% (n=745) and 43% (n=307) achieved two- and three-component remission at 12 months, respectively.72 The missing component for both datasets was improved or stabilised lung function, with the two-component dataset also not including asthma symptom control.72 In XALOC-2, which included analysis of the impact of BMI, the proportion of participants meeting three-component remission criteria, missing improvement or stabilisation of lung function, was 51.3% (n=76) for
participants with normal BMI (<25 kg.m2) and 30.4% (n=79) for participants with obesity (BMI ≥30 kg/m2 ).73 The lower rate of clinical remission in XALOC-2 participants with obesity was largely attributed to inadequately improved symptom control, and as such, Korn highlighted a need to pay particular attention to these patients.73
Korn also discussed data from the REDES clinical trial on the impact of mepolizumab in patients with SEA, where 63% (n=260) of patients on mepolizumab achieved three-component remission, excluding lung function stabilisation or improvement from remission criteria, compared to 37% (n=260) on placebo after 1 year.74 Korn also highlighted longer-term data from the QUEST and TRAVERSE trials with dupilumab, which showed increasing rates of clinical remission over time, with 35.04% of patients with uncontrolled, moderateto-severe, Type 2 inflammatory asthma achieving four-component remission after 1 year, which was sustained at years 1.5 (38.36%) and 2 (36.10%) (N=1,584).75
The percentage of participants who did not meet any clinical remission criteria at baseline reduced from 68.76% to 9.86%, 5.11%, and 7.84% at years 1, 1.5, and 2, respectively (N=1,584).75 At baseline, the remaining 30.88% of participants met one criterion, with this number reducing to 10.10%, 14.13%, and 12.35% at years 1, 1.5, and 2, respectively (N=1,584).75
Data from the NAVIGATOR trial on tezepelumab indicated that clinical remission could be achieved in patients with severe uncontrolled asthma, regardless of blood eosinophil levels.76 To define clinical remission, NAVIGATOR utilised strict criteria, using an ACQ-6 score of ≤0.75 and a requirement of pre-BD FEV1 of >80% or improvement in pre-BD FEV1 of >20%, as well as two additional assessments.76 One was for healthcare professional assessment of change using the Clinical Global Impression of Change (CGI-C) score, and the other was for patient assessment of severity using the Patient Global Impression of Severity (PGI-S) score.76 At Week 52, 12% of patients on tezepelumab (n=53) achieved remission, compared to 4% on placebo (n=17).76 Changing symptom
control and lung function criteria to ACQ-6 score ≤1.5 and pre-BD FEV1 and/or pre-BD FEV1 baseline of ≥0.95, resulted in clinical remission for 21% and 11% of participants on tezepelumab (n=97) and placebo (n=48), respectively.76 Patients with missing data were excluded from the analysis.76
Findings from a longitudinal cohort study on severe asthma using data from 23 countries from the International Severe Asthma Registry suggested that regardless of biologic choice, patients with fewer asthmarelated symptoms and lower long-term OCS use before biologic initiation, have a greater chance of achieving clinical remission.77 In the study, after 1 year of treatment, 20.3% of patients (n=1,059) with data on all four components reached four-component remission when lung function criteria were set to percent predicted FEV1 ≥80%.77 Additionally, 50.2% of patients (n=2,142) with data available reached two-component remission with no exacerbations and no longterm OCS use.77 Patients with fewer asthmarelated symptoms and lower long-term OCS use before biologic initiation have a greater chance of achieving clinical remission.77
To help more patients with SEA reach remission, Korn suggested that the status quo around treatment of severe asthma should be redefined. As part of this, Korn highlighted how uncontrolled asthma negatively impacts patient QoL, with asthma symptoms limiting daily activities.78,79 Korn advocated for improving disease control with earlier intervention and suggested that a treat-to-target approach could not only slow disease progression but also prevent irreversible damage.80-82 Key takeaways from Korn were that 1) clinical remission using biologics is an achievable goal for certain patients, with Korn highlighting that this should be the treatment goal in severe asthma due to the positive impact on patient QoL,3,83 2) patients in remission are those more likely to remain in remission, indicating durability,84 and that 3) remission has a positive impact on patient outcomes and should be the clinical goal in severe asthma.83 Korn did, however, highlight the need to continue refining the definition of remission with optimised tools and patient identification.
Beyond Asthma Control and Remission: Tackling the Treatment Escalator
Stefano Del Giacco
In the final session, Del Giacco led a panel discussion focused on the potential benefits of tapering background medications in SEA. The overarching goal of the discussion was to drive positive practice change and, as such, focused on reducing the burden of background medications, particularly corticosteroids, while maintaining effective asthma control.
The panel agreed that the potential treatment goal in appropriate patients should be tapering background medication while maintaining asthma control. They highlighted key benefits, including lessening treatment burden, including reduction of corticosteroidassociated treatment side effects, reducing healthcare utilisation, and overall reducing associated costs, if implemented effectively.85 To help with this, it was noted that guidelines need to be updated with the latest clinical trial data on the use of biologics in SEA. Milger-Kneidinger and Del Giacco highlighted that while some guidelines consider this, several key guidelines are behind. Herth agreed, suggesting that reports by the Global Initiative for Asthma (GINA) are the most useful resource,3 as they are a frequently updated source of practical recommendations that can support the management of SEA and the use of biologics.
GINA shared advice regarding reduction in background therapy in those patients who have demonstrated a good asthma response to therapy that targets Type 2 inflammation, with the highest priority given on reducing and ceasing maintenance of OCS, if used.3 To guide adjustment of maintenance ICS, GINA advises regular evaluation of each severe asthma treatment, either through assessment of patient symptom control or using biomarkers such as sputum eosinophil count and FeNO.3 Addressing how this can be achieved, if not already, these practices should be incorporated into existing patient pathways. This will be important for successful implementation and adoption.
Del Giacco raised the idea of potential reservations and anxiety of patients in terms of the patient’s response to the idea of reducing background therapy. The panel agreed that patients are very receptive to this, with Milger-Kneidinger and Korn suggesting patient excitement is common. Herth added that, based on experience, those with severe asthma are usually more informed about their condition, which adds to their positive experience when suggesting the reduction of background therapy. Patients who are well-informed and understand what to expect from their asthma care have demonstrated improved outcomes and higher adherence to treatments versus those who are not.86
Herth mentioned SHAMAL71 , a randomised clinical trial where patients on benralizumab were able to reduce corticosteroid use and that it could be used as a reference for tapering. However, Herth stated that it is critical that one prioritises local prescribing, labelling, and indications when considering dose reduction of ICS. Herth also highlighted that in their experience, the dose reduction of corticosteroids is not necessarily the primary issue impacting patients with SEA; rather, the major difficulty currently faced is that a high number of patients are still not using biologics. As suggested by the panel, more data on the potential benefits of early intervention with biologics will be helpful to ensure practice change.
References
1. Global Asthma Network. The Global Asthma Report 2022: Global burden of disease due to asthma. Available at: https://globalasthmareport.org/ burden/burden.php. Last accessed: 16 September 2024.
2. Cao Y et al. Global trends in the incidence and mortality of asthma from 1990 to 2019: An age-periodcohort analysis using the global burden of disease study Front Public Health. 2022;10:1036674.
3. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention. 2024. Available at: https://ginasthma. org/2024-report/. Last accessed: 16 September 2024.
4. Nunes C et al.. Asthma costs and
The major takeaway from the panel was the need to focus on patients who still have uncontrolled symptoms, especially those who are currently not on biologics. Milger-Kneidinger emphasised that patients reducing background medication should continue seeing a specialist to ensure their condition is monitored in case of worsening symptoms so that the patient does not fully stop taking medications that may be required for disease control.
Conclusion
The symposium provided valuable insights into the management of SEA, particularly focusing on the roles of eosinophils, airway remodelling, and PAO. It highlighted the critical importance of reducing eosinophils to mitigate exacerbations, improve lung function, and manage airflow limitation, alongside how biologics are currently key to helping achieve clinical remission in responsive patients. The discussion also reinforced the potential for tapering background medications, including corticosteroids, in well-controlled SEA. With these advancements, the overarching goal is to improve patient outcomes, reduce healthcare costs, and enhance the QoL in patients with SEA by refining treatment approaches and promoting earlier intervention.
social impact. Asthma Res. Pract. 2017;3:1.
5. The European Lung White Book. ERS - European Respiratory Society. Available at: https://www.ersnet.org/ the-european-lung-white-book/. Last accessed: 16 September 2024.
6. Heaney LG et al. Eosinophilic and noneosinophilic asthma: an expert consensus framework to characterize phenotypes in a global real-life severe asthma cohort. Chest. 2021;160(3):814-30.
7. Casciano J et al. Burden of asthma with elevated blood eosinophil levels. BMC Pulm Med. 2016;1691):100.
8. Price DB et al. Blood eosinophil count and prospective annual asthma disease burden: a UK cohort study. Lancet Respir. Med. 2015;3(11):849-58.
9. Newby C et al. Lung function decline and variable airway inflammatory pattern: longitudinal analysis of severe asthma. J. Allergy Clin Immunol. 2014;134(2):287-94.
10. de Groot JC et al. Management of the patient with eosinophilic asthma: a new era begins. ERJ Open Res. 2015;1: 00024-–02015.
11. de Groot JC et al. Management of the patient with eosinophilic asthma: a new era begins. ERJ Open Res. 2016;2(3):00024-2015-ERR. Corrected and republished from: ERJ Open Res. 2015;1(1):00024-2015.
12. Carroll N et al. The distribution of eosinophils and lymphocytes in the large and small airways of asthmatics. Eur Respir J. 1997;10(2):292-300.
13. Hekking PPW et al. The prevalence of severe refractory asthma. J Allergy Clin Immunol. 2015;135(4):896-902.
14. Volmer T et al. Consequences of longterm oral corticosteroid therapy and its side-effects in severe asthma in adults: a focused review of the impact data in the literature. Eur Respir J. 2018;52(4):1800703.
15. Israel E et al. Severe and difficult-totreat asthma in adults. N Engl J Med. 2017;377(10):965-76.
16. McBrien CN et al. The Biology of Eosinophils and Their Role in Asthma. Front Med (Lausanne). 2017;4:93.
17. Lombardi C et al. The emerging roles of eosinophils: Implications for the targeted treatment of eosinophilicassociated inflammatory conditions. Curr Res Immunol. 2022;3:42-53.
18. Jackson DJ et al. Living without eosinophils: evidence from mouse and man. Eur Respir J. 2023;61(1):2201217.
19. McDowell PJ et al. The inflammatory profile of exacerbations in patients with severe refractory eosinophilic asthma receiving mepolizumab (the MEX study): a prospective observational study. Lancet Respir. Med. 2021;9(10):1174-84.
20. Constantine GM et al. Recent advances in understanding the role of eosinophils. Fac Rev. 2022;11:26.
21. Rogers L et al. Biologics in severe asthma: a pragmatic approach for choosing the right treatment for the right patient. Respir Med. 2023;218:107414.
22. Fixman ED et al. Basic mechanisms of development of airway structural changes in asthma. Eur Respir J. 2007;29(2):379-89.
23. Busse WW. The relationship of airway hyperresponsiveness and airway inflammation. Chest. 2010;138(2 Suppl):4S-10S.
24. AZ EpiCentral Global. Airway hyperresponsiveness in severe asthma. Available at: https://global. epicentralmed.com/epifundamentals/ airway-hyperresponsiveness-severeasthma. Last accessed: 16 September 2024.
25. Crimi E et al. Dissociation between airway inflammation and airway hyperresponsiveness in allergic asthma. Am J Respir Crit Care Med. 1998;157(1):4-9.
26. Chapman DG, Irvin CG.Mechanisms of airway hyper-responsiveness in asthma: the past, present and yet to come. Clin Exp Allergy. 2015;4594):706-19.
27. Dunican EM et al. Autopsy and imaging studies of mucus in asthma. lessons learned about disease mechanisms
and the role of mucus in airflow obstruction. Ann Am Thorac Soc. 2018;15:S184-91.
28. Dunican EM. et al. Mucus plugs in patients with asthma linked to eosinophilia and airflow obstruction. J Clin Invest. 2018;128(3):997-1009.
29. Chan R et al. Eosinophil depletion with benralizumab is associated with attenuated mannitol airway hyperresponsiveness in severe uncontrolled eosinophilic asthma. J Allergy Clin Immunol. 2023;151(3):7005.e10.
30. Chan R et al. Efficacy of biologic therapy on airway hyperresponsiveness in asthma. Ann Allergy Asthma Immunol. 2023;131(1):37-41.
31. Milger K. et al. Bronchodilator reversibility in the GAN severe asthma cohort. J Investig Allergol Clin Immunol. 2023;33(6):446-56.
32. Flood-Page P et al. Anti-IL-5 treatment reduces deposition of ECM proteins in the bronchial subepithelial basement membrane of mild atopic asthmatics. J Clin Invest. 2003;112(7):1029-36.
33. Tsubokawa F et al. Effects of benralizumab on three-dimensional computed tomography analysis in severe eosinophilic asthma. Int Arch Allergy Immunol. 2023;184(3):243-51.
34. Nordenmark LH et al. Tezepelumab and mucus plugs in patients with moderate-to-severe asthma. NEJM Evid. 2023;2(10):EVIDoa2300135.
35. Hamakawa M, Ishida T. Usefulness of mepolizumab for mucus plugs. Intern Med. 2024;DOI:10.2169/ internalmedicine.3531-24.
36. Anai M et al. Successful treatment with dupilumab for mucus plugs in severe asthma. Respirol Case Rep. 2022;11(1):e01074.
37. McIntosh MJ et al. CT Mucus Score and 129 Xe MRI Ventilation Defects After 2.5 Years’ Anti-IL5Rα in Eosinophilic Asthma. Chest. 2023;164(1):27-38.
38. Tang M et al. Mucus plugs persist in asthma, and changes in mucus plugs associate with changes in airflow over time. Am J Respir Crit Care Med. 2022; 205(9):1036-45.
39. Mümmler C et al. Overall response to anti-IL-5/Anti-IL5-Rα treatment in severe asthma does not depend on initial bronchodilator responsiveness. J Allergy Clin Immunol Pract. 2022;10(12):3174-83.
40. Götschke J. Einfluss von mucus plugging auf lungenfunktionelle und klinische parameter vor und unter biologikatherapie bei patienten mit schwerem asthma. pneumologie 2024;78(S01):S8.
41. Bonser LR. et al. Airway mucus and asthma: the role of MUC5AC and MUC5B. J Clin Med. 2017;6(12):112.
42. Heijink IH et al. Epithelial cell dysfunction, a major driver of asthma development. Allergy. 2020;75(8):1902-17.
43. Ballester B et al. The role of mucin 1 in respiratory diseases. Eur Respir Rev. 2021;30(159):200149.
44. Porsbjerg C et al. Asthma. Lancet Lond Engl. 2023;401(10379):858-73.
45. Rutting S et al. Fixed airflow obstruction in asthma: a problem of the whole lung not of just the airways. Front Physiol. 2022;13:898208.
46. Del Olmo Sansone RA. Stability and predictive value of persistent airflow limitation in patients with physiciandiagnosed COPD and/or asthma in the NOVELTY study. Abstract A1149. ATS International Conference. 19-24 May, 2023.
47. Bennett GH et al. Risk factors and clinical outcomes associated with fixed airflow obstruction in older adults with asthma. Ann Allergy Asthma Immunol. 2018;120(2):164-8.e1.
48. Lee JH et al. Risk factors associated with persistent airflow limitation in severe or difficult-to-treat asthma: insights from the TENOR study. Chest. 2007;132(6):1882-9.
49. Hanania NA et al. Efficacy of dupilumab in patients with moderateto-severe asthma and persistent airflow obstruction. Ann Allergy Asthma Immunol. 2023;130(2):206-14. e2.
50. Kole TM et al. Predictors and associations of the persistent airflow limitation phenotype in asthma: a posthoc analysis of the ATLANTIS study. Lancet Respir. Med. 2022;10(12):e116. Corrected and republished from: Lancet Respir. 2023;11(1):55-64.
51. Contoli M et al. Fixed airflow obstruction due to asthma or chronic obstructive pulmonary disease: 5-year follow-up. J Allergy Clin Immunol. 2010;125(4):830-7.
52. Huang S et al. Asthma, airflow limitation and mortality risk in the general population. Eur Respir J. 2015;45(2):338-46.
53. Cohen L et al. Epithelial cell proliferation contributes to airway remodeling in severe asthma. Am J Respir Crit Care Med. 2007;176(2):13845.
54. Holgate ST. The sentinel role of the airway epithelium in asthma pathogenesis. Immunol Rev. 2011;242(1):205-19.
55. Bartemes KR et al. Dynamic role of epithelium-derived cytokines
in asthma. Clin Immunol. 2012;143(3):222-35.
56. Heijink IH et al. Airway epithelial barrier function regulates the pathogenesis of allergic asthma. Clin Exp Allergy. 2014;44(5):620-30.
57. Chipps BE et al. Benralizumab efficacy for patients with fixed airflow obstruction and severe, uncontrolled eosinophilic asthma. Ann. Allergy Asthma Immunol. 2020;124(1):79-86.
58. Hanania NA et al. Omalizumab in asthma with fixed airway obstruction: post hoc analysis of EXTRA. J Allergy Clin Immunol Pract. 2022;10(1):222-8.
59. Israel E et al. Efficacy of tezepelumab in patients with asthma and persistent airflow obstruction: a pooled analysis of the PATHWAY and NAVIGATOR studies. Chest. 2023;164(4):A15-7.
60. Actis GC, Pellicano R. Inflammatory bowel disease: efficient remission maintenance is crucial for cost containment. World J Gastrointest Pharmacol Ther. 2017;8(2):114-9.
61. Pierre N et al. Defining biological remission in Crohn’s disease: interest, challenges and future directions. J Crohns Colitis. 2023;17(10):1698-702.
62. van Vollenhoven RF et al. 2021 DORIS definition of remission in SLE: final recommendations from an international task force. Lupus Sci Med. 2022;9(1):e000538corr1. Corrected and republished from: Lupus Sci Med. 2021;8(1):e000538.
63. Yu C et al. Remission rate and predictors of remission in patients with rheumatoid arthritis under treat-totarget strategy in real-world studies: a systematic review and meta-analysis. Clin Rheumatol. 2019;38(3):727-38.
64. Studenic P et al. American College of Rheumatology/EULAR Remission Criteria for Rheumatoid Arthritis: 2022 revision. Arthritis Rheumatol. 2023;75(1):15-22.
65. Ostor AJ et al. Value of remission in patients with rheumatoid arthritis: a targeted review. Adv Ther. 2022;39(1):75-93.
66. Lommatzsch M et al. Pioneering a paradigm shift in asthma management:
remission as a treatment goal. Lancet Respir Med. 2024;12(2):96-9.
67. Blaiss M et al. Consensus of an American College of Allergy, Asthma, and Immunology, American Academy of Allergy, Asthma, and Immunology, and American Thoracic Society workgroup on definition of clinical remission in asthma on treatment. Ann Allergy Asthma Immunol. 2023;131(6):782-5.
68. Menzies-Gow A et al. An expert consensus framework for asthma remission as a treatment goal. J Allergy Clin Immunol. 2020;145(3):757-65.
69. Menzies-Gow A et al. Clinical remission in severe asthma: a pooled post hoc analysis of the patient journey with benralizumab. Adv Ther. 2022;39(5):2065-84.
70. Devouassoux G. Clinical remission in patients with severe eosinophilic asthma treated with benralizumab who were randomised to reduce their inhaled corticosteroid/formoterol dose: SHAMAL post-hoc analysis. PA1194. ERS Congress, 7-11 September, 2024.
71. Jackson DJ et al. Reduction of daily maintenance inhaled corticosteroids in patients with severe eosinophilic asthma treated with benralizumab (SHAMAL): a randomised, multicentre, open-label, phase 4 study. Lancet Lond Engl. 2024;403(10432):1140. Corrected and republished from: Lancet. 2024;403(10423):271-81.
72. Jackson DJ et al. Benralizumab effectiveness in severe asthma is independent of previous biologic use. J Allergy Clin Immunol Pract. 2022;10(6):1534-44.e4.
73. Lommatzsch M et al. Clinical remission by BMI in patients with severe eosinophilic asthma (SEA) over 1 year post benralizumab: realworld XALOC-2 programme. PA3932. ERS Congress, 7-11 September, 2024.
74. Pavord I et al. Remission outcomes in severe eosinophilic asthma with mepolizumab therapy: analysis of the REDES study. Front Immunol. 2023;14:1150162.
75. Pavord ID et al. Dupilumab induces clinical remission in patients with uncontrolled, moderate-to-severe, type
2 inflammatory asthma. A5995. ATS International Conference, 19-24 May, 2023.
76. Castro M et al. On-treatment clinical remission with tezepelumab among patients with severe, uncontrolled asthma in the phase 3 NAVIGATOR study. Eur Respir J. 2022;60(suppl 66):2287.
77. Perez-de-Llano L et al. Exploring definitions and predictors of severe asthma clinical remission post-biologic in adults. Am J Respir Crit Care Med. 2024;DOI:10.1164/rccm.2023112192OC.
78. Correia de Sousa J et al. Asthma control, quality of life, and the role of patient enablement: a cross-sectional observational study. Prim Care Respir J. 2013;22(2):181-7.
79. Kharaba Z et al. An assessment of quality of life in patients with asthma through physical, emotional, social, and occupational aspects. a crosssectional study. Front Public Health. 2022;10:883784.
80. O’Byrne P et al. Asthma progression and mortality: the role of inhaled corticosteroids. Eur Respir J. 2019;54(1):1900491.
81. Nannini LJ. Treat to target approach for asthma. J Asthma. 2020;57(6):687-90.
82. Papi A et al. Treatment strategies for asthma: reshaping the concept of asthma management. Allergy Asthma Clin Immunol. 2020;16:75.
83. Thomas D et al. Asthma remission: what is it and how can it be achieved? Eur Respir J. 2022;60(5):2102583.
84. Lommatzsch M et al. Durability of benralizumab-induced remission in severe asthma: an analysis of the BORA study. OA1420. ERS International Congress, 9-13 September, 2023.
85. Louis R et al. Severe asthma standardof-care background medication reduction with benralizumab: ANDHI in Practice Substudy. J Allergy Clin Immunol Pract. 2023;11(6):1759-170.e7.
86. Winders T et al. Perspectives on decisions for treatment and care in severe asthma. World Allergy Organ J. 2021;14(1):100500.
Prioritising Patients and Planet: Advocating for Change in Respiratory Care
This review is based on an AstraZeneca-sponsored nonpromotional symposium that took place at the European Respiratory Society (ERS) Congress 2024, held between 7th–11th September 2024 in Vienna, Austria.
Chairpersons: John Hurst,1 Helen Reddel2
Speakers: Omar Usmani,3 Erika Penz4
1. Department of Respiratory Medicine, University College London (UCL), UK
2. Clinical Management Group, Woolcock Institute of Medical Research, Sydney, Australia
3. National Heart and Lung Institute (NHLI), Faculty of Medicine, Imperial College London, UK
4. College of Medicine, University of Saskatchewan, Canada
Disclosure:
Hurst has received grant support, has been a speaker, and/or received travel honoraria, and has served on the advisory boards of pharmaceutical companies that make medicines to treat asthma and COPD, including AstraZeneca. Reddel has received grant funding from AstraZeneca, Chiesi Farmaceutici, GlaxoSmithKline (GSK), and Sanofi; has served as a consultant for AstraZeneca, Chiesi, and Novartis; has served on the advisory board for AstraZeneca, Chiesi Farmaceutici, GSK, and Sanofi-Genzyme; and has received speaker honoraria from Alkem, AstraZeneca, Boehringer Ingelheim, Chiesi Farmaceutici, Getz Pharma, GSK, and Teva Pharmaceuticals. Usmani has received grant funding and/or personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi Farmaceutici, Cipla, Covis Pharma, DEVA, Edmond Pharma, GSK, Kamada, KYORIN Pharmaceutical, Menarini, Mereo BioPharma, Mundipharma, Napp Pharmaceuticals, Novartis, Orion Pharma, Sandoz, Takeda Pharmaceuticals, Trudell Medical, and UCB. Penz has grant funding from the Canadian Institute Health Research, Lung Saskatchewan, Saskatchewan Health Research Foundation, AstraZeneca, GSK, and Sanofi; has served as a consultant for AstraZeneca, GSK, Sanofi, and Saskatchewan Cancer Agency; and has received speaker honoraria from AstraZeneca, Boehringer Ingelheim, Canadian Thoracic Society, Covis Pharma, GSK, Lung Saskatchewan, Sanofi-Genzyme, and Valeo Pharma.
Acknowledgements: Medical writing assistance was provided by Hannah Moir, EMJ, London, UK.
Disclaimer: The purpose of the non-promotional symposium was for disease state awareness and is not meant to imply the efficacy or safety of any AstraZeneca products or other medications. The information is intended for healthcare professionals only.
The symposium and publication of this article were organised, developed, and funded by AstraZeneca.
PHARMA PARTNERSHIP
Meeting Summary
The global burden of respiratory diseases, particularly asthma and chronic obstructive pulmonary disease (COPD), continues unabated. Suboptimal management places a significant strain on both patients and urgent or emergency care services. With an ageing population in many countries, the demand for these services is set to increase further. At the same time, healthcare systems are striving to reduce their carbon footprint and achieve net zero emissions, as the healthcare sector is a significant contributor to carbon emissions worldwide. Although these two goals may appear contradictory, they need not be in conflict.
This article reviews an industry-sponsored symposium held at the European Respiratory Society (ERS) Congress 2024 in Vienna, Austria, in September 2024. The session addressed the urgent need to change the delivery model for respiratory healthcare in response to the increasing prevalence of respiratory diseases and the challenges posed by climate change.
Co-chair John Hurst, Professor of Respiratory Medicine at University College London (UCL), UK, underscored the importance of innovative solutions for managing respiratory diseases and highlighted the challenges faced by healthcare decision-makers. This was further elaborated on by Omar Usmani, Professor of Respiratory Medicine at Imperial College London, UK, who emphasised the importance of clinical choice. He stated that inhaled medicines, which form the cornerstone of treatment, should not be considered interchangeable. He also discussed ongoing efforts to maintain access to essential medicines by developing novel next-generation propellants (NGP) for pressurised metered-dose inhaler (pMDI) devices, which will reduce their carbon footprint to levels comparable with dry powder inhalers (DPI). Additionally, he described the European Chemicals Agency (ECHA) proposal to restrict a broad range of chemicals classed as per- and polyfluoroalkyl substances (PFAS). This precautionary measure would affect both current propellants in pMDIs and the transition to NGPs, with global implications for inhaled medicines.
Erika Penz, Associate Professor of Respirology, Critical Care, and Sleep Medicine at the University of Saskatchewan, Canada, noted that suboptimal management of respiratory disease is associated with a disproportionately high burden on both patients and the environment. The forthcoming availability of pMDI medicines with NGPs alone will not resolve this larger issue. As every healthcare interaction carries a carbon footprint, which increases with the intensity of treatment, the implementation of guidelines into clinical practice would improve patient outcomes and reduce the demand on healthcare services and the associated carbon emissions.
Co-chair Helen Reddel, Clinical Professor and Research Leader at the Woolcock Institute of Medical Research, Australia, concluded by re-emphasising the urgent need to implement guidelines immediately for the benefit of both patients and the environment.
Healthcare decision-makers are facing significant challenges that will intensify in the coming years as they work to address health inequities, improve system resilience, and reduce carbon emissions. As Hurst highlighted, the global burden of respiratory disease continues unabated, placing a significant burden on patients, healthcare systems, and society. In the UK alone, 40% of asthma patients are uncontrolled,1 with delays in referrals to specialist services for severe asthma diagnoses and management.2 Additionally, COPD is a common cause of emergency admissions,3 with more than one in three patients not receiving maintenance therapy following one severe or more than one moderate COPD exacerbation(s).4 Only 44% of those who experience a COPD exacerbation survive after 5 years.5 Furthermore, Hurst reported a “lack of access to lifesustaining,” inhaled corticosteroid (ICS)containing therapies in up to two-thirds of low-to-middle-income countries.6,7
The situation is expected to become ever more challenging as the global population ages, increasing the prevalence of respiratory diseases and the complexity of patients’ needs.8,9,10 These challenges are compounded by climate change, which poses a significant health risk and is associated with an increase in respiratory illnesses and other health emergencies.11,12 Hurst stated, “As respiratory clinicians, we have some big challenges on our hands, but this is not the only challenge, we have the wider challenge of planetary health, and as a subset, we should be thinking about climate change.” Rising temperatures are projected to cause an estimated 250,000 additional deaths annually between 2030–2050.12 Ironically, the healthcare sector itself is a major greenhouse gas (GHG) emitter; if it were a country, it would rank as the fifth-largest GHG emitter in the world.13 Therefore, healthcare is a critical sector for decarbonisation, and there is an urgent need to reduce carbon emissions now.
Hurst emphasised that these seemingly conflicting challenges of increasing demand and reducing carbon emissions do not need to be in conflict. He stated, “They are intimately connected, and by solving both together, we can achieve the most benefit.” Hurst advocated for urgent changes in the delivery model and for innovative solutions to provide respiratory care more efficiently and proactively by preventing disease onset, diagnosing disease early, and optimising its management.14-16 This approach would reduce the demand for urgent or emergency care and keep patients out of hospitals.14
To achieve a more preventative approach to respiratory care, Hurst proposed implementing global, evidence-based recommendations for COPD (e.g., the Global Initiative for Chronic Obstructive Lung Disease [GOLD])17 and asthma (e.g., the Global Initiative for Asthma [GINA]),18 into local guidelines and routine practice. He argued, “Implement these guidelines properly, and we improve the health of hundreds of millions of patients around the world, and at the same time improve planetary health.” This is crucial for optimising patient outcomes, reducing the strain on overstretched resources, and decreasing the carbon footprint of care.14-16,19 Hurst specified that while the delivery model for healthcare requires urgent change to achieve its goals, restricting clinical choice and access to innovative medicines is not the way forward.
The Importance of Inhaler Choice to Personalise and Optimise Treatment
Omar Usmani
Usmani expanded on Hurst’s message, highlighting that inhaled medicines are the foundation of treatment for patients with asthma and/or COPD.20 According to current guidelines, they are recommended for use across all stages of disease severity.17,18 It is therefore crucial to have a diverse range of inhalers and treatment regimens available to enable personalised and optimised care for respiratory diseases.17,18 The choice of an inhaled medicine should be guided by a combination of disease and patient-specific
factors,21 which is why Usmani emphasised that inhalers should not be considered readily interchangeable.22
Considering the Disease, Drug, and Device for Personalised Respiratory Care
When selecting the most appropriate inhaler regimen, several factors must be considered for personalised care.17,18,23 Usmani summarised these factors as relating to the device, the drug, and the disease, emphasising that all three play a significant role in achieving the best possible patient outcomes. In terms of the disease, considerations include the diagnosis, severity, and presence of any comorbidities. The choice of the device relies on a patient’s ability for correct use, which is particularly important for vulnerable populations such as children, the elderly, or those with a compromised ability to use dry powder devices.24 To accommodate the heterogeneity of patients with respiratory disease, an array of inhaler delivery options are available, reflecting the principle that there is no “one size fits all” solution.24 Usmani emphasised, “We should personalise and select the best device for the patient.” Patient preference and satisfaction with their inhaler are also crucial to ensuring treatment adherence.21
Usmani further noted that what is often overlooked by healthcare professionals (HCP) is selecting the medication contained within the inhaler device. Multiple factors must be considered, including efficacy, safety, contraindications, dosing regimen, metabolism, and drug-to-drug interactions.25-28 He pointed out a common misconception: assuming that all drugs within the same pharmacological class have the same profile.25-28 To illustrate this, Usmani discussed the case of ICS, which are commonly prescribed either alone or in combination with bronchodilators for patients with asthma and/or COPD.17,18 Despite being in the same class, ICS can differ significantly in their pharmacokinetic and pharmacodynamic profiles leading to differences in their profiles for efficacy and safety, and the way they are recommended in guidelines.25-28
Usmani indicated that it is essential for HCPs to recognise and apply these fundamental elements to prescribe the right inhaler regimen for each patient. He stated, “We have a choice to personalise the drug and the device to our patients.” Thus, clinical choice is imperative to optimise patient outcomes.
Global Warming Potential of Current Inhaler Devices
The global warming (GWP) potential for current medical propellants has led some in the respiratory community to advocate for a blanket switch from pMDIs to DPIs.29 However, pMDIs play a critical role in respiratory care, representing 77% of inhaler usage globally and being the most commonly used inhaler type in 49 out of 53 countries analysed.30 Nevertheless, Usmani emphasised the importance of considering this in the context of total global anthropogenic carbon emissions, noting that the contribution of pMDIs is less than 0.04%.31
Usmani argued that implementing policies on the availability and use of pMDI medicines solely based on their environmental impact, without a patientcentric approach, could be detrimental to both patients and clinical practice.32 He also noted that in other areas of medicine with similar prognosis to asthma or COPD, patients are not denied effective treatments based on their carbon footprint. It is essential not to compromise on the quality of care by ensuring that the most effective medicines remain available.
Considering Patient and Healthcare Professional Perspectives in Inhaler Device Switching
Usmani highlighted the importance of ensuring that the voice of the respiratory community, including patients, is heard by those advocating for restrictions on inhaler device type, based on environmental factors. He presented recent findings from the largest global survey of its kind, which ranked the priorities of HCPs and patients with asthma and/or COPD when prescribing or choosing an inhaler device based on medical, nonmedical, and environmental factors.33 The
survey, conducted across 42 countries in six continents and involving 468 HCPs and 270 patients, found that clinical efficacy was ranked as the most important factor while environmental impact was considered the least important.33 Additionally, fewer than half (45.9%) of HCPs and less than twothirds (60.1%) of patients expressed concern about the potential contribution of inhalers to climate change.33
Usmani also discussed the impact of nonclinical, non-consensual device switching and the potential for unintended consequences, such as unpredictable disease outcomes and increased healthcare resource utilisation (HCRU).34-36 He cited the potential for harm to the doctor-patient relationship especially when switches are without the patient’s consent.34,37 In qualitative surveys, patients have reported feeling a lack of control and believing their health and life were at risk in such situations.34
Moreover, a recently convened global expert panel on quality statements related to inhaler regimen switches concluded that it is essential to consider fully the time and resources required to implement such a switch, as well as the complexity of doing so at scale. The panel provided a practical checklist of essential activities to ensure any switch is both effective and safe.35
Approximately 18.2 million people with asthma and/or chronic lower respiratory disease (including COPD) use a pMDI as part of their care in the EU.35 Usmani described the significant challenges healthcare would face if environmentally driven policies enforced a blanket switch for a large number of patients. Data on the impact of switching inhaler regimens is limited; however, a systematic review of real-world outcomes concluded that it is difficult to predict clinical outcomes, including exacerbations and other factors that impact HCRU.34
Transition to Next-Generation Propellants (NGPs) for pMDI Inhalers
In the final part of Usmani’s presentation, he provided an update on the progress toward transitioning to NGPs, which have
lower GWPs.38,39 His main focus was on hydrofluoroolefin (HFO)-1234ze(E) with a 100-year GWP of 1.4, which is considered a near-zero propellant.39 This is 99.9% lower than the propellant most commonly used today (hydrofluoroalkane (HFA)134a).39 Using the example of a fixed-dose combination triple therapy pMDI approved for use in COPD, he showed that a device using HFO-1234ze(E) would reduce GHG emissions by 85%, bringing its carbon footprint in line with that of DPIs (Figure 1).40 Usmani reported that the clinical trials required for regulatory approval of an HFO-1234ze(E)containing NGP had been completed, with submission expected later in 2024 and availability anticipated from 2025.38 He emphasised that transition to NGPs is an important step in decarbonising healthcare, enabling the use of lower carbon devices without needing to change prescriptions or risk the potential for harm from non-clinically driven switches.
Usmani then highlighted draft legislation that is being evaluated by the ECHA for a wide restriction on PFAS chemicals which has global implications for inhaled medicines.41-44 The objective of the legislation is to minimise exposure to the environment of molecules which may be persistent. PFAS have been defined by chemical structure and the entire class of approximately 12,000 molecules is in the scope of the ban, including HFO1234ze, despite a degradation half-life of 18 days.41,42 No exemption is currently proposed for medical propellants.45 He emphasised the importance of the respiratory community, as experts on the essential role of inhaled medicines, to inform the ongoing legislative process during the next public consultation phase expected in 2025. He provided a link for the audience to find more information on the ECHA proposal.46
The key takeaway from Usmani was that personalised inhaled therapy for those with asthma and/or COPD involves selecting both the medicine and the device.21 He emphasised that switching inhaler regimens for non-clinical reasons can lead to variable clinical outcomes.34 The transition to pMDIs with a carbon footprint similar to a DPI is
Figure 1: Next-generation propellant pressurised metered-dose inhalers containing HFO-1234ze have a similar carbon footprint to a dry powder inhaler.40
expected to begin from 2025.38,40 Lastly, Usmani opined that the greenest inhaler is the one that a patient can and will use effectively,47 highlighting that the bigger challenge is addressing suboptimal care.
Addressing the Patient and Societal Burden of Suboptimal Respiratory Care and Its Environmental Impact
Erika Penz
The delivery of care is a contributor to healthcare GHG emissions, with more intensive treatment resulting in a higher carbon footprint.48 Penz highlighted that every healthcare interaction has a carbon footprint (Figure 2),49 which means that clinical choices can directly impact healthcare emissions and the carbon footprint of care.14 She used her presentation to illustrate how common suboptimal management of respiratory
disease is associated with increased HCRU, from poor disease control, exacerbations, and increased use of short-acting β2agonist (SABA) relievers, all of which contribute to increased GHG emissions.50 In addition to impacting patients and stretching healthcare resources, this also has environmental consequences.51 Thus, adopting a more preventative approach to managing respiratory disease would also offer an environmental benefit.
Implications of Poor Respiratory Control on Carbon Footprint
According to the SABINA CARBON study, patients with poorly controlled asthma have a carbon footprint (measured as per capita [per 10,000 person-year] GHG emissions) approximately three times higher than those with well-controlled asthma.52 In the UK, the carbon footprint of overall asthma care is over 750,000 tonnes CO2 equivalent (CO2e) per year.52 Around 40% of this is attributed to treating the consequences of
Figure 2: Greenhouse gas emissions (kg of CO2 equivalent) per healthcare resource utilisation event in the UK.49
*Note this data excludes emissions associated to prescriptions. GP: general practitioner.
poor control, such as exacerbations and SABA overuse, amounting to approximately 300,000 tonnes CO2e per year.52
Overuse of SABA relievers is also common in COPD and is associated with poor clinical outcomes.53 The high use of SABA is associated with a significantly higher risk of both moderate and severe exacerbations, as well as higher overall mortality rates.53 Overall, SABA relievers constitute the majority of inhaler use and carbon footprint in Europe and Canada, ranging from 33–71% of inhaler use depending on the country,51 contributing to two-thirds of the total GHG emissions from inhalers, and revealing that suboptimal treatment of respiratory disease remains widespread and has an environmental consequence.51
Penz highlighted that the impact of even a single COPD exacerbation can extend beyond the lungs and last up to a year.54,55
The EXACOS-CV study found that the risk of severe cardiovascular events increases after even a moderate COPD exacerbation.54 More broadly, the SHERLOCK study showed that one or more moderate or severe exacerbations increased all-cause HCRU (comprising primary care, outpatient visits, and hospitalisations) in the 12 months of follow-up.55 Penz noted that the growing
Intensity
body of evidence suggests that, regardless of disease severity, taking a more preventative approach to COPD treatment is crucial for improving patient outcomes.
The consequences of suboptimal COPD care have a disproportionate impact on the carbon footprint of COPD-related HCRU. The carbon footprint of patients with COPD in England has recently been quantified in the EXACOS CARBON study.56 Notably, maintenance inhalers, which have been a focus of the inhaler device carbon debate and calls for switching, make a relatively minor contribution to the overall healthcare carbon footprint of these patients (63,867 tonnes CO2e for COPD maintenance inhalers alone), whereas the carbon footprint of COPD patients’ HCRU is approximately six-fold higher (414,187 tonnes CO2e of HCRU) than that of routine medicines. 56 Penz also reported the disproportionate impact of COPD exacerbations on the carbon footprint. Patients who experienced two or more severe exacerbations had GHG emission rates seven-fold greater than those with no exacerbations (Figure 3).56 Overall, an estimated 6.8% of the GHG emissions of the National Health Service (NHS) in England result from the HCRU of patients with COPD.56
Real-World Impact of Guideline Implementation on Patient Outcomes and Carbon Footprint
Choices in patient care can directly impact the carbon footprint of healthcare.14 Penz stated that up-to-date, evidence-based treatment recommendations guide on how to optimise treatment for COPD17 and asthma.18 This was exemplified through several studies.
Regarding asthma care, the implementation of the GINA recommendations18 and the 2020 national New Zealand asthma guidelines (which prefer the use of an anti-inflammatory reliever) was associated with a reduced risk of hospital admission.57 Penz stated that the active implementation of the New Zealand guideline led to a >2-fold increase in the use of guidelinerecommended therapy in the second half of 2022 compared with the second half of 2019.57 Over the 3 years following the implementation of the guidelines, there was a 17% reduction in hospital asthma discharges.57 These findings,
Penz noted, underscored the importance of implementing guidelines to facilitate real-world practice changes that lead to improved patient outcomes.
Penz also summarised the SENTINEL programme, which involved a real-world, system-wide adoption of guideline-directed medical therapy in England, which included a maintenance and reliever therapy (MART)preferred strategy; free from the use of SABA as a reliever as it does not treat the underlying inflammation in asthma.15,58 The quality improvement programme targeted those patients with asthma who were most at risk of an exacerbation, identified through high SABA prescribing (≥3 SABA canisters) or a history of exacerbations.15 A pharmacist-led treatment review was used to optimise their management in line with local guidelines, including the prescription of MART in appropriate patients.15 During the implementation phase, the proportion of patients prescribed MART increased approximately four-fold and was maintained over the observation period.15 The proportion
Figure 3: Greenhouse gas emissions from the HCRU of patients with COPD in England based on exacerbation history over a baseline period.56
of patients prescribed three or more SABA canisters over a 12-month period fell by 48.3%.15 Importantly, there was a 29.8% reduction in severe asthma exacerbations.15 SENTINEL is a quality improvement programme, that includes what is believed to be the first prospective analysis to investigate improvements in patient outcomes and carbon reduction through guideline implementation. The full results will be published in due course, but Penz reported interim data showing that SABA prescribing declined by 27,609 inhalers, equating to a saving of 773 tonnes of CO2e.58
Penz also highlighted that proactive and preventative care is crucial for COPD management. She presented real-world evidence from Canada’s Best Care COPD programme, which implemented a primary care-based, integrated disease management approach to improve patient outcomes in COPD.59 The programme, which involved collaboration between primary care providers, patients/caregivers, certified respiratory educators, and case managers, focused on education, skills, and treatment management.59 The trajectory of COPDrelated and all-cause HCRU changed from an increasing trend over 3 years before the intervention to a sustained long-term reduction in both COPD-related emergency department visits and hospital admissions over the 3 years following implementation.59 Her message was that these choices in clinical care would also have a direct impact on its carbon footprint.
Penz also discussed PROMETHEUS Canada, a modelling study that investigated the potential impact of fully implementing the 2023 Canadian Thoracic Society COPD guideline recommendations for single inhaler triple therapy over a 10year period in the country, which were new data being presented at the ERS conference.60 The study estimated that guideline implementation could decrease exacerbations (a 13.1% [n=200,000] reduction in ≥1 severe exacerbation[s] and a 17.5% [n=1,070,000] reduction in ≥1 moderate exacerbation[s]), decrease mortality (22.2% reduction in all-cause mortality, avoiding 180,000 deaths), and reduce HCRU and overall healthcare costs
(7.7% reduction in severe exacerbation cost, and 12.6% reduction in moderate exacerbation cost), equating to total savings of approximately 3.5 billion CAD.60 As every healthcare interaction has a carbon footprint, the reduced demand on resources would also be expected to yield a carbon benefit.14
Penz concluded by re-emphasising that poorly controlled disease and exacerbations have a disproportionate impact on patients, healthcare systems, and the environment.51,52,55,56 Guideline recommendations indicate how to optimise treatment for both COPD17 and asthma.18 Therefore, implementing guidelines is a powerful way to improve patient outcomes and, consequently, reduce the carbon footprint of healthcare.15,58-60 This builds on Usmani’s perspective by saying that ‘the greenest patient is the one whose respiratory condition is well controlled’.47
Prioritising Patients and Planet: Advocating for Change in Respiratory Care
Helen Reddel
A more proactive, preventative model of healthcare is urgently needed to address the current and growing burden of respiratory diseases like asthma and COPD worldwide.14 Amid the increasing demand for healthcare and the need to address climate change, it is essential to maintain clinical choice and provide personalised treatment options for patients. Reddel suggested that this can be achieved by personalising respiratory care from the point of diagnosis and throughout its management. This includes selecting the right inhaled medication and device according to the individual’s needs, skills, and patient preferences.21
Reddel re-emphasised the importance of advocating for the implementation of guidelines to address suboptimal respiratory care and reduce environmental impact. Treatment recommendations such as GINA,18 highlight the importance of personalised treatment for optimal patient care. This
approach includes ensuring access to the right class of medication, where optimal inhaler selection is the safest and most effective for both the patient and the planet, while also ensuring availability, patient satisfaction, and proper inhaler use, and taking into account their environmental impact.18 From 2025, the transition of pMDI propellants to more climate-friendly NGPs is expected to significantly reduce the carbon footprint of pMDIs to levels comparable to those of DPIs.38,40,61 However, Reddel highlighted that implementing guidelines now is also a powerful way to immediately improve outcomes for patients and reduce the carbon footprint associated with healthcare.15,58-60
Reddel then reminded the audience about the proposed restriction by the ECHA on PFAS chemicals. This proposal has global implications for inhaled medicines.43,44 Reddel urged her colleagues to share information about the ECHA proposal with their colleagues and to be aware of the potential unintended consequences on patient outcomes,37,43 as outlined earlier by Usmani. She also noted the upcoming opportunity to participate in the next round of consultation, expected in 2025, and provided a link for the audience to find
References
1. Asthma UK. Asthma care in a crisis. Annual asthma survey. 2020. Available at: https://www.asthmaandlung.org. uk/sites/default/files/2023-03/aas2020_2a-1.pdf. Last accessed: 10 September 2024.
2. Asthma UK. Slipping through the net: the reality facing patients with difficult and severe asthma. 2018. Available at: https://www.asthmaandlung.org. uk/sites/default/files/2023-03/auksevere-asthma-gh-final.pdf. Last accessed: 10 September 2024.
3. Lane ND et al. Specialist emergency care and COPD outcomes. BMJ Open Respir Res. 2018;5(1):e000334.
4. Vogelmeier CF et al. COPD exacerbation history and impact on future exacerbations - 8-year retrospective observational database cohort study from Germany. Int J Chron Obstruct Pulmon Dis. 2021;16:2407-17.
5. van Hirtum PV et al. Long term survival after admission for COPD exacerbation: a comparison with
more information about the ECHA proposal (available in the reference list).46
Conclusion
Healthcare is facing significant challenges due to increasing demand and limited resources, which are set to increase with an ageing population and the impacts of climate change. It is also a major contributor to GHG emissions,13 and the healthcare sector must strive to achieve near net-zero carbon emissions across societies within the next few decades. Suboptimal management of respiratory disease is common and is associated with a disproportionate burden on patients, healthcare services, and the environment. Every healthcare interaction has a carbon footprint. Transitioning to medicines with a lower carbon impact, as anticipated for pMDIs from 2025, is crucial to maintaining clinical choice and preventing the unintended consequences of inhaler switching. However, there is a more urgent need to advocate today for better implementation of respiratory guidelines to improve outcomes both for patients and the planet.
the general population. Respir Med. 2018;137:77-82.
6. World Health Organization (WHO). Asthma. 2023. Available at: https:// www.who.int/news-room/fact-sheets/ detail/asthma. Last accessed: 10 September 2024.
7. Stolbrink M et al. Availability, cost and affordability of essential medicines for chronic respiratory diseases in lowincome and middle-income countries: a cross-sectional study. Thorax. 2024;79(7):676-9.
8. Chen X et al. Global, regional, and national burden of chronic respiratory diseases and associated risk factors, 1990-2019: results from the global burden of disease study 2019. Front Med (Lausanne). 2023;10:1066804.
9. Galiatsatos P et al. The association between neighborhood socioeconomic disadvantage and chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2020;15:981-93.
10. Alsallakh MA et al. Association of socioeconomic deprivation with asthma care, outcomes, and deaths in
Wales: a 5-year national linked primary and secondary care cohort study. PLoS Med. 2021;18(2):e1003497.
12. World Health Organization (WHO). Climate change. 2023. Available at: https://www.who.int/news-room/factsheets/detail/climate-change-andhealth. Last accessed: 10 September 2024.
13. Health Care Without Harm. Health care’s climate footprint. 2019. Available at: https://noharm-global.org/sites/ default/files/documents-files/5961/ HealthCaresClimateFootprint_092319. pdf. Last accessed: 10 September 2024.
14. Sustainable Markets Initiative (SMI). Decarbonising patient care pathways. 2022. Available at: https://a.storyblok. com/f/109506/x/88fe7ea368/smi-hstfpcp-whitepaper.pdf. Last accessed: 10 September 2024.
15. Crooks MG et al. Improving asthma
care through implementation of the SENTINEL programme: findings from the pilot site. ERJ Open Res. 2023;9(3):00685-2022.
16. Alzaabi A et al. Greenhouse gas emissions from respiratory treatments: results from the SABA CARBON international study. Adv Ther. 2023;40(11):4836-56.
17. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for prevention, diagnosis and management of COPD: 2024 Report. 2024. Available at: https://goldcopd.org/2024-goldreport/. Last accessed: 10 September 2024.
18. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention. 2024. Available at: https://ginasthma. org/2024-report/. Last accessed: 10 September 2024.
19. Wilkinson AJK et al. Environmental sustainability in respiratory care: an overview of the healthCARe-Based envirONmental Cost of Treatment (CARBON) Programme. Adv Ther. 2022;39(5):2270-80.
20. Usmani OS et al. Critical inhaler errors in asthma and COPD: a systematic review of impact on health outcomes. Respir Res. 2018;19(1):10.
21. Usmani OS. Choosing the right inhaler for your asthma or COPD patient. Ther Clin Risk Manag. 2019;15:461-72.
22. Björnsdóttir US et al. Potential negative consequences of nonconsented switch of inhaled medications and devices in asthma patients. Int J Clin Pract. 2013;67(9):904-10.
23. Bonini M, Usmani O. The importance of inhaler devices in the treatment of COPD. COPD Res Pract. 2015;DOI:10.1186/s40749-015-0011-0.
24. Scichilone N. Asthma control: the right inhaler for the right patient. Adv Ther. 2015;32(4):285-92.
25. Derendorf H et al. Relevance of pharmacokinetics and pharmacodynamics of inhaled corticosteroids to asthma. Eur Respir J. 2006;28(5):1042-50.
26. Rohatagi S et al. Risk-benefit value of inhaled glucocorticoids: a pharmacokinetic/pharmacodynamic perspective. J Clin Pharmacol. 2004;44(1):37-47.
27. Winkler J et al. How the lung handles drugs: pharmacokinetics and pharmacodynamics of inhaled corticosteroids. Proc Am Thorac Soc. 2004;1(4):356-63.
28. Daley-Yates PT. Inhaled corticosteroids: potency, dose equivalence and therapeutic index. Br
J Clin Pharmacol. 2015;80(3):372-80.
29. Wilkinson AJK et al. Costs of switching to low global warming potential inhalers. An economic and carbon footprint analysis of NHS prescription data in England. BMJ Open. 2019;9(1):e028763.
30. Bell J et al. An assessment of pressurized metered-dose inhaler use in countries in Europe and the rest of the world. Abstract 24041. The International Primary Care Respiratory Group IPCRG 2024, 9-11 May, 2024. Available at: https://www. ipcrg.org/24041. Last accessed: 10 September 2024.
31. Emeryk AW et al. Impact of inhalers used in the treatment of respiratory diseases on global warming. Adv Respir Med. 2021;89(4):427-38.
32. MedTech Europe. MedTech Europe Position on the Proposal for A REACH Universal PFAS Restriction. 2023. Available at: https://www. medtecheurope.org/resource-library/ medtech-europe-position-on-theproposal-for-a-reach-universalpfas-restriction/. Last accessed: 10 September 2024.
33. Lough G et al. Patient and provider perspectives driving inhaler choice: optimizing sustainable health care. Chest. 2024;DOI:10.1016/j. chest.2024.06.3774.
34. Usmani OS et al. Real-world impact of nonclinical inhaler regimen switches on asthma or COPD: a systematic review. J Allergy Clin Immunol Pract. 2022;10(10):2624-37.
35. Bell J et al. Potential impact of the draft PFAS legislation on patients with asthma and chronic lower respiratory diseases in the European Union. Abstract 24040. The International Primary Care Respiratory Group IPCRG 2024, 9-11 May, 2024. Available at: Available at: https://www.ipcrg. org/24040. Last accessed: 10 September 2024.
36. Attar-Zadeh D et al. Health-care resource requirements and potential financial consequences of an environmentally driven switch in respiratory inhaler use in England. J Health Econ Outcomes Res. 2021;8(2):46-54.
37. Doyle S et al. What happens to patients who have their asthma device switched without their consent? Prim Care Respir J. 2010;19(2):131-9.
38. Pritchard JN. The Climate is changing for metered-dose inhalers and action is needed. Drug Des Devel Ther. 2020;14:3043-55.
39. Smith C et al. The Earth’s energy budget, climate feedbacks and climate sensitivity supplemental material. In: Masson-Delmotte V et al. Climate
change 2021: the physical science basis. 2021. Available at: ipcc.ch/ report/ar6/wg1/downloads/report/ IPCC_AR6_WGI_Chapter07_SM.pdf. Last accessed: 10 September 2024.
40. Hargreaves C et al. S60 A new medical propellant HFO-1234ze(E): reducing the environmental impact of inhaled medicines. Thorax 2022;77(Suppl1):A38-9.
41. European Chemicals Agency (ECHA). Annex XV restriction report. Proposal for a restriction. 22 March 2023. Available at: https://echa.europa.eu/ documents/10162/1c480180-ece91bdd-1eb8-0f3f8e7c0c49. Last accessed: 10 September 2024.
42. United States Environmental Protection Agency (EPA). TSCA 8(a)(7) PFAS Chemicals. 2024. Available at: https://cdxapps.epa.gov/ oms-substance-registry-services/ substance-list-details/490. Last accessed: 10 September 2024.
43. Levy ML et al. Global access and patient safety in the transition to environmentally friendly respiratory inhalers: the global initiative for asthma perspective. Lancet. 2023;402(10406):1012-6.
44. Freshfields Bruckhaus Deringer. The EU’s chemicals strategy for sustainability – the story so far. 22 May 2024. Available at: https:// sustainability.freshfields.com/ post/102j8a0/the-eus-chemicalsstrategy-for-sustainability-the-storyso-far. May 2024. Last accessed: 10 September 2024.
45. European Commission. Guiding criteria and principles for the essential use concept in EU legislation dealing with chemicals. 22 April 2024. Available at: https://environment.ec.europa. eu/document/download/fb27e67ac275-4c47-b570-b3c07f0135e0_ en?filename=C_2024_1995_ F1_COMMUNICATION_FROM_ COMMISSION_EN_V4_P1_3329609. PDF. Last accessed: 10 September 2024.
46. AstraZeneca. The voice of the respiratory community is important to inform on the need for exemptions to ECHA PFAS restrictions, in order to safeguard supply of inhaled medicines for patients. September 2024. Available at: https://congresspublication. com/rrk3bb?utm_term=QR&utm_ medium=Poster&utm_campaign=ERS2024&utm_content=Placeholder-forAnna-Lawson---ERS-SustainabilitySymposium-InfoGraphic&utm_ source=&utm_contentcategory=NotDetermined-Yet. Last accessed: 19 September 2024.
47. Pritchard A, Usmani OS. The greenest inhaler: a patient-centric approach. EMJ Respir. 2022;10(Suppl 2):2-7.
48. Tennison I et al. Health care's response to climate change: a carbon footprint assessment of the NHS in England. Lancet Planet Health. 2021;5(2):e84-e92.
49. Coalition for Sustainable Pharmaceuticals and Medical Devices (CSPM). Care pathways: guidance on appraising sustainability. 2015. Available at: https://shcoalition. org/wp-content/uploads/2019/10/ Sustainable-Care-PathwaysGuidance-Summary-Oct-2015.pdf. Last accessed: 10 September 2024.
50. Nwaru BI et al. Overuse of shortacting β2-agonists in asthma is associated with increased risk of exacerbation and mortality: a nationwide cohort study of the global SABINA programme. Eur Respir J. 2020;55(4):1901872.
51. Janson C et al. The carbon footprint of respiratory treatments in Europe and Canada: an observational study from the CARBON programme. Eur Respir J. 2022;60(2):2102760.
52. Wilkinson AJK et al. Greenhouse gas emissions associated with suboptimal asthma care in the UK: the SABINA healthCARe-Based envirONmental
cost of treatment (CARBON) study. Thorax. 2024;79(5):412-21.
53. Janson C et al. High use of shortacting β2-agonists in COPD is associated with an increased risk of exacerbations and mortality. ERJ Open Res. 2023;9(3):00722–2022.
54. Hawkins NM et al. Heightened long-term cardiovascular risks after exacerbation of chronic obstructive pulmonary disease. Heart. 2024;110(1):702-9.
55. de Nigris E et al. Short- and long-term impact of prior chronic obstructive pulmonary disease exacerbations on healthcare resource utilization and related costs: an observational study (SHERLOCK). COPD. 2023;20(1):92100.
56. Bell J et al. A54 EXACOS CARBON: Describing the greenhouse gas emissions of healthcare resource utilization by frequency and severity of COPD exacerbation in England (abstract). Am J Respir Crit Care Med. 2024;209:A2113.
57. Noble J et al. Patterns of asthma medication use and hospital discharges in New Zealand. J Allergy
Clin Immunol Glob. 2024;3(3):100258.
58. The Sentinel Project. Improving outcomes for asthma patients in Hull and East Yorkshire 2024. Available at: https://hullasthma.co.uk/. Last accessed: 10 September 2024.
59. Licskai C et al. Quantifying sustained health system benefits of primary care-based integrated disease management for COPD: a 6-year interrupted time series study. Thorax. 2024;79(8):725-34.
60. Bhutani M et al. PA1170 Implementation of 2023 CTS guidelines for SITT could reduce exacerbation and mortality rates in COPD: PROMETHEUS Canada. Abstract PA1170. European Respiratory Society (ERS) Congress 2024, 7-11 September 2024. Available at: https://www.ersnet.org/wpcontent/uploads/2024/08/CongressProgramme-2024-0508.pdf. Last accessed: 10 September 2024.
61. Pernigotti D et al. Reducing carbon footprint of inhalers: analysis of climate and clinical implications of different scenarios in five European countries. BMJ Open Respir Res. 2021;8(1):e001071.
Heterogeneity of Inflammatory Processes and Pathways Driving
Chronic Obstructive Pulmonary Disease Pathology
These symposia took place on the 9th and 10th of September 2024 as part of the European Respiratory Society (ERS) Congress held in Vienna, Austria.
Chairpersons: Klaus Rabe1 and Henrik Watz2
Speakers: Mona Bafadhel,3 Stephanie Christenson,4 Alberto Papi,5 Klaus Rabe,1 Paola Rogliani,6 Henrik Watz2
1. Director of the Department of Pneumology, LungenClinic, Grosshansdorf, Germany
2. Medical Director, German Centre for Lung Research, Grosshansdorf, Germany
3. Chair of Respiratory Medicine and Director of the King’s Center for Lung Health, King’s College London, UK
4. Associate Professor of Medicine, University of California, San Francisco, USA
5. Professor of Respiratory Medicine and Director of Diseases, University of Ferrara, Italy
6. Director of Respiratory Medicine, University of Rome ‘Tor Vergata’, Italy
Disclosure: Rabe has received grants and research support from the German Federal Ministry for Research and Technology (BMFT); honoraria or consultation fees from AstraZeneca, Berlin-Chemie, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Menarini, Novartis, Sanofi, Regeneron, and Verona Pharma. Rabe serves as the Director of the Airway Research Centre North (ARCN) within the Deutsche Zentrum für Lungenforschung (DZL). Watz has received consulting fees, payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events; support for attending meetings and/or travel; and participation on a data safety monitoring board or advisory board, all from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, and Sanofi. Watz is disease area coordinator of COPD for the German Centre for Lung Research and coordinator of the German COPD guideline. Bafadhel has received grants and research support from AstraZeneca, Roche, Sanofi, and GlaxoSmithKline; honoraria and consulting fees from AstraZeneca, Sanofi, and GlaxoSmithKline; and acted as a scientific advisor for Areteria and AlbusHealth. Christenson has acted as a consultant for AstraZeneca, GlaxoSmithKline, Glenmark, and Sanofi/Regeneron; and has provided writing services for UpToDate. Papi has been a board member and/or received grants, research, consulting, lecture, or travel support from Chiesi Farmaceutici, AstraZeneca, GlaxoSmithKline, Mundipharma Research Limited, Novartis, Sanofi, Menarini, Zambon, Edmond Pharma, and Elpen. Rogliani has received grants and research support from Arcede, AstraZeneca, Boehringer Ingelheim, Chiesi Farmaceutici, GlaxoSmithKline, Menarini Group, Novartis, Sanofi, and Verona Pharma; and honoraria or consultation fees from AstraZeneca, Boehringer Ingelheim, Chiesi Farmaceutici, GlaxoSmithKline, Menarini Group, Novartis, Recipharm, Sanofi, and Zambon.
Acknowledgements: Medical writing assistance was provided by International Meetings and Science (IMsci), Stamford, Connecticut, USA.
Support: The symposia were sponsored by Sanofi and by Regeneron Pharmaceuticals Inc., and this article was commissioned and supported by the same companies. Sanofi and Regeneron Pharmaceuticals Inc. have reviewed this article for medical accuracy.
Meeting Summary
Two symposia occurred during the European Respiratory Society (ERS) Congress 2024, highlighting the heterogeneity in chronic inflammatory pathways that underlie chronic obstructive pulmonary disease (COPD) pathophysiology. In 'A Breath of Fresh Air: A Greater Understanding of COPD With Type 2 Inflammation', Henrik Watz (Chair), German Center for Lung Research, Grosshansdorf, Germany, provided an overview of both the pathophysiology and the burden of disease of COPD. He discussed how exacerbations, which may be increased in those with evidence of Type 2 inflammation, contribute to the cycle of worsening COPD. Mona Bafadhel, King’s College London, UK, provided an examination of the mechanisms and biomarkers of Type 2 inflammation in COPD. Finally, Alberto Papi, University of Ferrara, Italy, summarised the latest research on biological treatments targeting Type 2 inflammation in COPD. The second symposium, 'Targeting interleukin-33 (IL-33) in COPD: Exploring New Frontiers for COPD Management', discussed inflammation in COPD, focusing on the central role of IL-33 as a mediator for both Type 2 and Type 1/Type 3 inflammation. Klaus Rabe (Chair), LungenClinic, Grosshansdorf, Germany, reviewed the structure and function of IL-33 and its initial processes that lead to downstream immune responses. Stephanie Christenson, University of California, San Francisco, USA, explored how genetic and environmental factors contribute to IL-33 activity in COPD pathology. Next, Paola Rogliani, University of Rome ‘Tor Vergata’, Italy, presented an examination of IL-33 inflammatory processes and evidence from COPD animal models illustrating the role of IL-33 in airway inflammation and lung function decline. Klaus Rabe concluded with an examination of IL-33 as a target for new COPD treatment approaches.
Introduction
A persistent, often progressive, lung disease, COPD results from chronic inflammation that leads to structural changes resulting in airway remodelling and airflow obstruction.1,2 However, just as individuals with COPD can present with different symptom patterns, the inflammatory pathways involved in COPD pathophysiology are
also heterogeneous.1 Although Type 1/ Type 3 inflammation drives COPD in most individuals, up to ~30−40% have Type 2 inflammation, and there is also potential overlap in inflammatory mechanisms.3-5
PHARMA
A Breath of Fresh Air: A Greater Understanding of COPD with
Type 2 Inflammation
Living with COPD: Linking Inflammation with Patient Burden
Henrik Watz
Chronic inflammation, triggered by irritants and oxidative stress (eg., tobacco smoke, pollutants), is the key factor driving the airway and parenchymal structural changes that characterise COPD and limit airflow in the lungs (Figure 16).1,2,7 Pathophysiological changes in the airway specifically linked to chronic inflammation in COPD include barrier disruption, goblet cell hyperplasia, inflammation and excess mucus, and remodelling. Parenchymal structural changes include breakdown of the alveolar membranes (emphysema) and air trapping.1,2 Smoking, pollutants, environmental or occupational exposure, abnormal lung growth and development, and genetics and early life events all increase the risk of chronic inflammation leading to COPD.1 Even in individuals with COPD who have
stopped smoking, the risk of exacerbations, morbidity, and mortality remains elevated for years.8
Traditionally, COPD was informally categorised based on the clinical observation of predominant symptoms, including the 'pink puffer' emphysema phenotype, associated with dyspnoea, hyperinflation, air trapping, and cachexia, and the 'blue bloater' chronic bronchitis phenotype, associated with chronic productive cough, respiratory infections, exacerbations, and being overweight.1,9 These characterisations were of limited clinical utility, only applicable for describing severe disease, and insufficient to encompass COPD pathophysiological or phenotype heterogeneity.9,10 Currently, COPD categorisation reflects an evolving, broader disease spectrum that includes emphysema- and bronchitis-predominant phenotypes, as well as a frequent exacerbator or rapid decliner phenotype, and two endotypes based on the underlying inflammatory pathway: 1) Type 1/Type 3 and 2) Type 2.1,9,11-14
Figure 1: COPD is driven by chronic inflammation and structural changes.6
COPD: chronic obstructive pulmonary disease.
Airflow limitation
inflammation
Structural changes of airways
In addition to increasing morbidity and mortality, COPD places a heavy physical and emotional burden on individuals and contributes to physical debilitation and poor health-related quality of life.1,15,16 In interviews, individuals with persistent COPD symptoms cite exhaustion, breathlessness, feelings of depression and dread, limits on physical activity, and difficulties in lying down at night to sleep.17
More than 80% of individuals with COPD are estimated to have >1 comorbid condition.18 Associated pulmonary conditions include bronchiectasis, asthma, pulmonary arterial hypertension, and an increased risk of lung cancer.1,19,20 Extrapulmonary conditions seen in individuals with COPD include cardiovascular (CV) conditions, such as heart failure, ischaemic heart disease, and arrhythmias; osteoporosis; renal failure; metabolic syndrome; diabetes; gastrooesophageal reflux disease; and neurologic or psychiatric conditions.1,19-21 Multi-morbidity significantly impacts quality of life and health outcomes and is associated with increased COPD exacerbations, hospitalisations, medical costs, and mortality.22
Exacerbations of COPD increase disease burden, hospitalisations, and re-hospitalisations, and are associated with a poor prognosis. An analysis of 32 studies found 9−26% and 18−39% of COPD hospitalisations resulted in readmission within 30 days and 90 days, respectively. The most common significant risk factors for readmission were comorbidities, previous exacerbations and hospitalisations, and longer initial hospital stay, with frequent COPD exacerbations increasing readmission risk 2.5-fold.23 Patients who experience more severe exacerbations tend to have an increased incidence of CV events.24 Exacerbations also lead to an increased risk of CV death, whether the patient is hospitalised or not.25 Increased frequency and severity of exacerbations have been associated with increased rates of all-cause mortality, COPD-related mortality rate, and future exacerbations.26,27 Importantly, repeated exacerbations lead to progressive and potentially irreversible lung damage. Following a moderate or severe COPD exacerbation, forced expiratory volume in
1 second (FEV1) may not reach a patient’s pre-exacerbation levels, even after ≥1 month.28 Further, individuals who have frequent exacerbations show a significantly faster decline in FEV1 than those with infrequent exacerbations.29 Severe lung function impairment has been shown to be significantly associated with increased 90-day post-discharge mortality.30 In all, low FEV1 is a risk factor for COPD exacerbations and hospitalisations, contributing to a vicious cycle of exacerbations and declining lung function.13
Evidence from studies investigating increased blood eosinophil (EOS) counts, which can correspond to increased lung EOS numbers and elevated markers of Type 2 inflammation in the airways, supports a higher disease burden for individuals with COPD associated with Type 2 inflammation.1,31 An analysis of data from the Genetic Epidemiology of COPD study in 1,553 individuals with COPD found the risk for COPD exacerbations increased with increasing blood EOS counts, particularly for those with blood EOS ≥300 cells/µL.31 The Canadian Cohort of Obstructive Lung Disease study examined blood EOS counts in participants aged ≥40 years with and without COPD. The study found that the annual decline in FEV1 for those with EOS ≥300 cells/µL was significantly greater than for those with lower EOS levels (P≤0.01).32 Elevated EOS count (≥300 cells/µL) has been shown to be a marker for COPDrelated rehospitalisation at 30 days up to 12 months and for all-cause rehospitalisation at 90 days up to 12 months.33 In an observational study, individuals with COPD with ≥300 EOS cells/µL were 3.21 times more likely to be readmitted to the hospital for COPD than those with EOS <300 EOS cells/µL.34
In summary, Watz emphasised that worsening disease in COPD contributes to a vicious cycle.35 Increased chronic inflammation and its attendant structural damage worsens symptoms and increases exacerbation risk, leading to a progressive decline in lung function.1,2,7
Unravelling the Role of Type 2 Inflammation in COPD
Mona Bafadhel
The Type 1/Type 3 and Type 2 endotypes of COPD have distinct characteristics.1,14 Type 1/Type 3 inflammation is marked by elevations in sputum neutrophils, Type 1 cytotoxic and T helper (Th) 1 and 17 cells, and innate lymphoid cell (ILC) 3, whereas Type 2 inflammation markers include elevated sputum EOS, Th2 cells, ILC2, and Type 2 cytokines IL-4, IL-13, and IL-5.36-40
Bafadhel underscored the potential roles of Type 2 cytokines in COPD with Type 2 inflammation, including airway remodelling, goblet cell hyperplasia, mucus production, and EOS trafficking to tissues (Figure 26).41-45 Blood EOS is recognised by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) as a biomarker for inhaled corticosteroid (ICS) use, with levels ≥300 cells/μL indicating a higher likelihood that ICS may prevent COPD exacerbations.1 However, COPD endotyping
remains an emerging concept, and the lack of established biomarkers to differentiate inflammatory profiles complicates the treatment decision-making process.11,46,47 To date, fibrinogen remains the only circulating biomarker approved by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) to assess the risk of COPD exacerbations and mortality.48 Other biomarkers that have been investigated in relation to COPD clinical outcomes include blood and sputum EOS count, fractional exhaled nitric oxide (FeNO), and alpha-1 antitrypsin.10,48,49
Bafadhel highlighted the potential of biomarkers to improve COPD understanding and treatment. She emphasised their practicality and ease of use in clinical settings, suggesting that with further research, these biomarkers could play a larger role in personalised COPD therapy. To highlight these points, she summarised several studies illustrating the potential utility of EOS and FeNO in assessing COPD disease and treatment. In a study of 226
Figure 2: Potential roles of Type 2 cytokines in COPD with Type 2 inflammation.6
individuals with COPD, the annualised rate of moderate and/or severe acute COPD exacerbations was significantly higher in individuals with ≥2 visits where FeNO measured ≥20 parts per billion than in individuals with 0 or 1 visit (P<0.05).50 Elevated EOS was associated with an increased incidence rate ratio of severe and moderate COPD exacerbations in a study of >7,000 individuals with COPD participating in the Copenhagen General Population Study.51 Another analysis of data from this study found that blood EOS ≥300 cells/µL and FeNO ≥20 parts per billion separately and together were significantly associated with FEV1 decline (P≤0.004).52 Lastly, Bafadhel showed data supporting EOS and FeNO as biomarkers to predict ICS responsiveness in COPD. In a post hoc analysis of a randomised trial, annual COPD exacerbation rates were lower with budesonide+formoterol than with formoterol alone in individuals with blood EOS ≥340 cells/μL, but not in individuals with blood EOS <100 cells/μL.53 A separate study showed that ICS plus a long-acting β2 agonist reduced COPD Assessment Test scores by 7.20 points from baseline in individuals with COPD and high baseline FeNO, but was not as effective for improving this measure in those with low baseline FeNO.54
On Target: Perspectives From the Evolving Biologic Landscape in COPD
Alberto Papi
The 2024 GOLD algorithm for therapy escalation after a COPD exacerbation uses blood EOS levels to guide decisions.1 According to GOLD, all individuals experiencing an exacerbation should be treated with a long-acting β-agonist plus a long-acting muscarinic antagonist, but those with EOS ≥300 cells/μL also should receive ICS.1 Despite the optimisation of inhaled treatment with triple therapy, some individuals remain at risk for exacerbations. Papi reviewed the evolving COPD treatment landscape and presented data from clinical studies in COPD for biological therapies targeting steps in the Type 2 inflammatory pathway.
Targeting IL-33 in COPD: Exploring New Frontiers for COPD Management
Understanding the Role of IL-33 Size and Activity in the Pathophysiology of COPD
Klaus Rabe
Rabe reviewed the complexity and diversity of the inflammatory pathways associated with COPD pathology and discussed the structure and function of IL-33. Full-length IL-33 (IL-33FL) secretion from airway epithelial cells is induced in response to inhaled irritants, pathogens, and allergens. In this form, IL-33FL can be cleaved by proteases from inflammatory cells or allergens to form hyperactive, mature IL-33, which has 30- to 60-fold higher activity than IL-33FL, or inactivated by oxidation, sequestration, and proteolytic degradation. Mature, activated IL-33 stimulates ST2+ immune cells, triggering both Type 1 and Type 2 inflammation that can underpin COPD pathology. However, inactivated IL-33 may induce ST2-independent signalling and also promote a COPD phenotype.55,56 Because of its key role in the pathophysiology of different COPD endotypes and phenotypes, IL-33 is a promising therapeutic target.
What Do We Know About IL-33 Genetics?
Stephanie Christenson
Christenson discussed how IL-33 activity in COPD pathology involves a convergence of genetic variations and environmental exposures. To characterise the impact of IL-33 genetics on COPD risk, investigators performed an analysis of IL-33 loss-offunction (LOF) and gain-of-function (GOF) variants known to affect asthma risk among individuals of European ancestry utilising data from the UK Biobank and Geisinger Health System studies in COPD.57 Three variants were selected for analysis: 1) a rare IL33 LOF slice-acceptor allele that reduces total IL33 messenger RNA (mRNA) and decreases asthma risk; 2) a common IL33 intronic GOF variant that increases IL33
mRNA and asthma risk; and 3) a common IL1RL1 (gene that encodes the IL-33 receptor) intronic GOF variant that lowers plasma levels of soluble IL-33 receptor and increases asthma risk. The results showed that the rare LOF variant was associated with a 21% reduction in the risk of COPD and a reduction in blood EOS (P<0.0001), but the two common GOF variants were associated with significantly increased odds of COPD (P<0.05 for each variant).57
Next, Christenson reviewed how smoking influences IL-33 activity in COPD and highlighted the importance of considering the complex effects of smoking on IL-33 activity within the context of COPD. An analysis of IL-33 levels in 62 individuals with COPD showed that smoking pack-years was positively correlated with IL-33 expression in the lungs (R=-0.58). In this study, a larger proportion of individuals with high IL-33 had previously regularly smoked cigarettes than patients with low IL-33; in contrast, those who were currently regularly smoking cigarettes tended to have low IL-33.58 This trend of individuals who currently regularly smoke having lower IL-33 expression than those who formerly regularly smoked has been confirmed in multiple studies of samples collected by bronchial biopsy or bronchial brushings.59 This finding may be due to the shifting of basal cells towards a more differentiated state in those who currently regularly smoke, and may explain the clinical observation of greater efficacy of anti-IL-33 treatment in those with COPD who previously regularly smoked.59 However, even in those with COPD who currently regularly smoke, high IL-33 expression has been associated with lower percent predicted median residual volume and lower percent predicted and percent mean residual volume to total lung capacity.60
The Role of IL-33 in COPD Pathophysiology and Its Impact on Disease Remodelling
Paola Rogliani
Rogliani began with a closer look at the key role IL-33 plays in COPD as an initiator and amplifier of broad inflammatory cascades.
Stimulation from smoke, pollutants, infections, or oxidative stress induces IL-33 production and secretion from the airway epithelium and the endothelium of blood vessels in the lungs.55,61 IL-33 then activates immune cells and non-haematopoietic lung cells to promote immune responses and increase inflammation (Figure 362).61 As a central mediator of inflammation in COPD, IL-33 drives both Type 1/Type 3 and Type 2 inflammatory responses, and stimulation of IL-33 can lead to increased neutrophil and blood EOS levels.5,45,63 The chronic inflammation initiated and amplified by IL33 results in airway remodelling, including airway smooth muscle thickening and fibrosis in small airways.7,64
Evidence from animal models illustrates how IL-33 plays a role in both Type 1/Type 3 and Type 2 inflammatory responses.65,66 In mice, systemic IL-33 overexpression produced through hydrodynamic DNA delivery induced significant neutrophilia, associated with Type 1/Type 3 inflammation, and eosinophilia, associated with Type 2 inflammation, in lung tissue, as well as production of Type 1 and Type 2 inflammatory cytokines.65 A separate study in mice found that prolonged exposure to house dust mites resulting in upregulation of IL-33 induced features of severe airway diseases, such as smooth muscle thickening, increased collagen deposition, and epithelial degeneration.66 Although initial inflammatory responses had Type 2 characteristics, including increased EOS, longer exposures led to a mixed inflammatory phenotype, with increased neutrophils and other markers of Type 1/ Type 3 inflammation.66
IL-33: A Promising Target
Klaus Rabe
Rabe reviewed the landscape of available therapies and those in development that target the chronic inflammation underlying COPD pathophysiology. He also presented data supporting IL-33 as a potential target for COPD treatment. Ongoing research is refining the understanding of IL-33 in COPD, focusing on identifying ideal patient subgroups for IL–33–targeted therapies,
IL-33 mediation of immune response and airway obstruction and remodelling
Fibroblasts
Endothelial cells
• Stimulation by infection, allergens, and environmental factors induce IL-33 production and release from lung tissue cells
• IL-33 activates immune cells and non-hematopoietic lung cells to promote immune response and airway remodelling
and evaluating the long-term efficacy and safety of these interventions. In all, Rabe articulated a shared vision of more personalised approaches in medicine, where treatments are tailored to individual patients based on their unique biological mechanisms.
Conclusion
As illustrated by the presentations in these symposia, COPD is a
References
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Available at: https://goldcopd. org/2024-gold-report/. Last accessed: 26 August 2024.
heterogeneous condition with variations in symptomatology, the events that trigger the chronic inflammation driving the disease processes, and the nature of the inflammatory pathways. Understanding the heterogeneity of inflammation in COPD pathophysiology helps to guide diagnosis and treatment. Optimal COPD treatment is critical to arresting the vicious disease cycle of exacerbations and worsening lung function that increases disease morbidity and mortality.
2. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16-27.
3. Singh D et al; ECLIPSE investigators. Eosinophilic inflammation in COPD: prevalence and clinical characteristics. Eur Respir J. 2014;44(6):1697-700.
4. Leigh R et al. Stable COPD: predicting benefit from high-dose inhaled corticosteroid treatment. Eur Respir J. 2006;27(5):964-71.
5. Yousuf A et al. T2 biologics for chronic obstructive pulmonary disease. J Allergy Clin Immunol Pract. 2019;7(5):1405-16.
6. Watz H. A breath of fresh air: a greater understanding of COPD with type 2 inflammation. Presentation Session 290. 7-11 September 2024.
7. Linden D et al. Respiratory viral infection: a potential "missing link" in the pathogenesis of COPD. Eur Respir Rev. 2019;28(151):180063.
8. Godtfredsen NS et al. COPD-related
Figure 3:
in COPD.62
Mast cell
Neutrophils T cell
Macrophage
morbidity and mortality after smoking cessation: status of the evidence. Eur Respir J. 2008;32(4):844-53.
9. Lan LTT, Dinh-Xuan AT. Pathophysiology updates for chronic obstructive pulmonary disease. Curr Respir Care Rep. 2013;2:139-44.
10. Hersh CP et al. COPDGene and ECLIPSE Investigators. Nonemphysematous chronic obstructive pulmonary disease is associated with diabetes mellitus. BMC Pulm Med. 2014;14:164.
11. Kakavas S et al. Pulmonary function testing in COPD: looking beyond the curtain of FEV1. NPJ Prim Care Respir Med. 2021;31(1):23.
12. Castaldi PJ et al. Cluster analysis in the COPDGene study identifies subtypes of smokers with distinct patterns of airway disease and emphysema. Thorax. 2014;69(5):415-22.
13. Garcia-Aymerich J et al. Lung function impairment, COPD hospitalisations and subsequent mortality. Thorax. 2011;66(7):585-90.
14. Aksoy E et al. Neutrophil to lymphocyte ratio is a better indicator of COPD exacerbation severity in neutrophilic endotypes than eosinophilic endotypes. Int J Chron Obstruct Pulmon Dis. 2018;13:2721-30.
15. Watz H et al. Physical activity in patients with COPD. Eur Respir J. 2009;33(2):262-72.
16. Miravitlles M, Ribera A. Understanding the impact of symptoms on the burden of COPD. Respir Res. 2017;18(1):67.
17. Cook N et al. Impact of cough and mucus on COPD patients: primary insights from an exploratory study with an online patient community. Int J Chron Obstruct Pulm Dis. 2019;14:1365-76.
18. Putcha N et al. Comorbidities and chronic obstructive pulmonary disease: prevalence, influence on outcomes, and management. Semin Respir Crit Care Med. 2015;36(4):57591.
19. Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009;33(5):116585.
20. Dal Negro RW et al. Prevalence of different comorbidities in COPD patients by gender and GOLD stage. Multidiscip Respir Med. 2015;10(1):24.
21. Gaddam S et al. Prevalence of chronic kidney disease in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. BMC Pulm Med. 2016;16(1):158.
22. Le TT et al. Prevalence and newly diagnosed rates of multimorbidity in older Medicare beneficiaries with
COPD. COPD. 2021;18(5):541-8.
23. Alqahtani JS et al. Risk factors for allcause hospital readmission following exacerbation of COPD: a systematic review and meta-analysis. Eur Respir Rev. 2020;29(156):190166.
24. Graul EL et al. Temporal risk of nonfatal cardiovascular events after chronic obstructive pulmonary disease exacerbation: A population-based study. Am J Respir Crit Care Med. 2024;209(8):960-72.
25. Kunisaki KM et al. Exacerbations of chronic obstructive pulmonary disease and cardiac events. A post hoc cohort analysis from the SUMMIT randomized clinical trial. Am J Respir Crit Care Med. 2018;198(1):51-7.
26. Whittaker H et al. Frequency and severity of exacerbations of COPD associated with future risk of exacerbations and mortality: A UK routine health care data study. Int J Chron Obstruct Pulm Dis. 2022;17:427-37.
27. Rothnie KJ et al. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice-based population with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(4):464-71.
28. Watz H et al. Spirometric changes during exacerbations of COPD: a post hoc analysis of the WISDOM trial. Respir Res. 2018;19(1):251.
29. Donaldson GC et al. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10):847-52.
30. Hartl S et al. Risk of death and readmission of hospital-admitted COPD exacerbations: European COPD Audit. Eur Respir J. 2016;47(1):113-21.
31. Yun JH et al. Blood eosinophil count thresholds and exacerbations in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2018;141(6):2037-47.e10.
32. Tan WC et al. High eosinophil counts predict decline in FEV1: results from the CanCOLD study. Eur Respir J. 2021;57(5):2000838.
33. Hegewald MJ et al. Blood eosinophil count and hospital readmission in patients with acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulm Dis. 2020;15:2629-41.
34. Couillard S et al. Eosinophils in COPD exacerbations are associated with increased readmissions. Chest. 2017;151(2):366-73.
35. Agusti AGN. COPD, a multicomponent disease: implications for management.
Respir Med. 2005;99(6):670-82.
36. Barnes PJ. Inflammatory endotypes in COPD. Allergy. 2019;74(7):1249-56.
37. Chen L et al. Imbalance between subsets of CD8(+) peripheral blood T cells in patients with chronic obstructive pulmonary disease. Peer J. 2016;4:e2301.
38. Ghebre MA et al. Biological exacerbation clusters demonstrate asthma and chronic obstructive pulmonary disease overlap with distinct mediator and microbiome profiles. J Allergy Clin Immunol. 2018;141(6):2027-36.e12.
39. Barczyk A et al. Cytokine production by bronchoalveolar lavage T lymphocytes in chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2006;117(6):1484-92.
40. Christenson SA et al. Asthma-COPD overlap. Clinical relevance of genomic signatures of type 2 inflammation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;191(7):758-66.
41. Cooper PR et al. Involvement of IL-13 in tobacco smoke-induced changes in the structure and function of rat intrapulmonary airways. Am J Respir Cell Mol Biol. 2010;43(2):220-6.
42. Doyle AD et al. Eosinophil-derived IL13 promotes emphysema. Eur Respir J. 2019;53(5):1801291.
43. Zheng T et al. Inducible targeting of IL-13 to the adult lung causes matrix metalloproteinase- and cathepsindependent emphysema. J Clin Invest. 2000;106(9):1081-93.
44. Alevy YG et al. IL-13-induced airway mucus production is attenuated by MAPK13 inhibition. J Clin Invest. 2012;122(12):4555-68.
45. Gandhi NA et al. Targeting key proximal drivers of type 2 inflammation in disease. Nat Rev Drug Discov. 2016;15(1):35-50.
46. Petersen H et al. Early endotyping: a chance for intervention in chronic obstructive pulmonary disease. Am J Respir Cell Mol Biol. 2018;59(1):13-7.
47. Stockley RA et al. Chronic obstructive pulmonary disease biomarkers and their interpretation. Am J Respir Crit Care Med. 2019;199(10):1195-204.
48. Cazzola M et al. Evolving concepts in chronic obstructive pulmonary disease blood-based biomarkers. Mol Diagn Ther. 2019;23(5):603-14.
49. Tang B et al. Relationship of blood eosinophils with fractional exhaled nitric oxide and pulmonary function parameters in chronic obstructive pulmonary disease (COPD) exacerbation. Med Sci Monit. 2020;26:e921182.
50. Alcázar-Navarrete B et al. Persistently elevated exhaled nitric oxide fraction is associated with increased risk of exacerbation in COPD. Eur Respir J. 2018;51(1):1701457.
51. Vedel-Krogh S et al. Blood eosinophils and exacerbations in chronic obstructive pulmonary disease. The Copenhagen General Population Study. Am J Respir Crit Care Med. 2016;193(9):965-74.
52. Çolak Y et al. Type-2 inflammation and lung function decline in chronic airway disease in the general population. Thorax. 2024;79(4):349-58.
53. Bafadhel M et al. Predictors of exacerbation risk and response to budesonide in patients with chronic obstructive pulmonary disease: a post-hoc analysis of three randomised trials. Lancet Respir Med. 2018;6(2):117-26.
54. Wu YK et al. Treatment of chronic obstructive pulmonary disease in patients with different fractional exhaled nitric oxide levels. Medicine (Baltimore). 2018;97(47):e11922.
55. Cayrol C, Girard JP. Interleukin-33 (IL33): a critical review of its biology and
the mechanisms involved in its release as a potent extracellular cytokine. Cytokine. 2022;156:155891.
56. Strickson S et al. Oxidised IL-33 drives COPD epithelial pathogenesis via ST2-independent RAGE/EGFR signalling complex. Eur Respir J. 2023;62(3):2202210.
57. Rabe KF et al. Safety and efficacy of itepekimab in patients with moderateto-severe COPD: a genetic association study and randomised, double-blind, phase 2a trial. Lancet Respir Med. 2021;9(11):1288-98. Session 450.
58. Joo H et al. Association between plasma interleukin-33 level and acute exacerbation of chronic obstructive pulmonary disease. BMC Pulm Med. 2021;21(1):86.
59. Faiz A et al. IL-33 Expression is lower in current smokers at both transcriptomic and protein levels. Am J Respir Crit Care Med. 2023;208(10):1075-87.
60. Kim SW et al. Factors associated with plasma IL-33 levels in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulm Dis. 2017;12:395-402.
61. Donovan C, Hansbro PM. IL-33 in chronic respiratory disease: from preclinical to clinical studies. ACS Pharmacol Transl Sci. 2019;3(1):56-62.
62. Rabe KF. Targeting IL-33 in COPD: exploring new frontiers for COPD management. Presentation Session 450. 7-11 September 2024.
63. Chan BCL et al. IL33: roles in allergic inflammation and therapeutic perspectives. Front Immunol. 2019;10:364.
64. Aghapour M et al. Airway epithelial barrier dysfunction in chronic obstructive pulmonary disease: role of cigarette smoke exposure. Am J Respir Cell Mol Biol. 2018;58(2):157-69.
65. Srivatsan S et al. IL-33 drives type 1 and type 2 inflammation and instructs airway remodeling. Presented at: American Thoracic Society 2023 International Conference; 19-24 May 2023.
66. Allinne J et al. IL-33 blockade affects mediators of persistence and exacerbation in a model of chronic airway inflammation. J Allergy Clin Immunol. 2019;144(6):1624-37.e10.
- 1.0 - 10/2024
Speakers:
Bronchiectasis Exacerbations: Are We Doing Everything We Can?
Talks from this industry-sponsored symposium took place during the European Respiratory Society (ERS) Congress 2024, held in Vienna, Austria from 7th–11th September 2024.
Pieter Goeminne,1 Michal Shteinberg2-4
1. Department of Respiratory Diseases, Vitaz Saint-Nicholas Hospitals, Belgium
2. Pulmonology Institute and CF Center - Carmel Medical Center, Haifa, Israel
3. Israel Institute of Technology, Haifa, Israel
4. The B. Rappaport Faculty of Medicine, Haifa, Israel
Disclosure: Goeminne received support from AstraZeneca, Chiesi, GSK, Insmed, and Merck Sharp & Dohme. Shteinberg received grants/research support from GSK, Novartis, and Trudell Pharma; honoraria or consultation fees from AstraZeneca, Boehringer Ingelheim, GSK, Synchrony Medical, Vertex Pharmaceuticals, and Zambon; speaker's fees from AstraZeneca, Boehringer Ingelheim, Dexcel, GSK, Insmed, Kamada, Novartis, Sanofi, Teva, and Truemed; and they are on the management board of the European Multicenter Bronchiectasis Audit and Research Collaboration (EMBARC).
Acknowledgements: Medical writing assistance was provided by Eleanor Roberts, Beeline Science Communications, Ltd, London, UK.
Disclaimer The symposium content and views expressed herein are those of the speakers and not necessarily of the sponsor.
Support: The symposium and publication of this article were sponsored by Insmed Incorporated (USA).
Meeting Summary
At the European Respiratory Society (ERS) Congress 2024, two experts in bronchiectasis, Pieter Goeminne, Department of Respiratory Diseases, Vitaz Saint-Nicholas Hospitals, Belgium, and Michal Shteinberg, Pulmonology Institute and CF Center - Carmel Medical Center; Israel Institute of Technology; and The B. Rappaport Faculty of Medicine, Haifa, Israel, discussed bronchiectasis’ pathogenesis and exacerbations, along with unmet needs regarding diagnosis and treatment. Bronchiectasis is a chronic and progressive inflammatory disease with a rising prevalence. Commonly associated conditions/related comorbidities of bronchiectasis include post-infective diseases and other airway conditions (such as chronic obstructive pulmonary disease [COPD] and asthma), although the cause
of bronchiectasis may remain unknown in over a third of patients. Development of bronchiectasis involves the intersection of four pathogenic components: chronic infections, airway ciliary dysfunction, chronic inflammation (mostly neutrophilic), and structural lung damage, commonly known as the 'vicious vortex.' In particular, bronchiectasis development, progression, and exacerbation also involve upregulated and dysregulated neutrophil function. Exacerbations in bronchiectasis are marked by symptoms of increased cough, sputum changes, decreased lung function, and fatigue, among others. Careful clinical examination and awareness of bronchiectasis symptoms are needed to properly diagnose and treat the initial condition and prevent exacerbations. Triggers for exacerbations can be endogenous, such as neutrophil or eosinophil increases, as well as exogenous, including the presence of infectious agents and pollution. Research regarding treatment for bronchiectasis is limited, but European guidelines recommend airway clearance techniques and antibiotics during exacerbations. To enable more targeted treatment for bronchiectasis from first occurrence, to limit exacerbations, and during an exacerbation, there are unmet needs for better identification of resistant genes, treatments for pathogens and inflammation, and biomarkers of exacerbation triggers.
Introduction
The chronic and progressive inflammatory disease bronchiectasis is characterised by permanent bronchi dilation and by symptoms such as recurrent bronchial infection, sputum production, chronic cough, dyspnoea, and exacerbations.1 Bronchiectasis prevalence estimates range by geographical region, gender, and age, with indications that prevalence is rising.2-4
One of the most common causes of bronchiectasis, as shown in 16,963 patients in the European Multicentre Bronchiectasis Registry Audit and Research Collaboration (EMBARC) registry, is post-infective disease (21.2%).5 Other causes include COPD (8.1%), asthma (6.9%), tuberculosis (4.9%), and immunodeficiency (4.1%). Of note though, 38.1% of patients in the registry had a cause listed as idiopathic. Bacteria are frequently linked with bronchiectasis, with the most common types found in the EMBARC cohort being Pseudomonas aeruginosa (in 25.1% of sputum samples) and Haemophilus influenzae (23.6%), followed by Enterobacteriaceae (15.9%), Staphylococcus aureus (8.6%), Streptococcus pneumoniae (8.5%), and Moraxella catarrhalis (5.4%).
Co-infection was common, with 36.1% of patients having samples positive for at least two pathogens. Occurrence of these
infectious agents may differ geographically, for example, H. influenzae infection was lower in Southern Europe, where P. aeruginosa predominated, and was higher in Northern and Western Europe.5
In the first two parts of this symposium, two leading experts in bronchiectasis, Goeminne and Shteinberg, discussed the pathogenesis of bronchiectasis as well as the recognition and control of exacerbations. Such exacerbations can greatly impact a patient’s health-related quality of life (HRQoL).
Bronchiectasis Development and Exacerbation
As shown in Figure 1, four pathogenic components intersect to drive bronchiectasis development, persistence, and exacerbations.6 The first two, chronic infections and dysfunction of airway epithelial cells and their cilia, result in hypersecretion of mucus. Inflammation, the third component, accompanies these phenomena, and together they can result in the fourth component, characteristic of bronchiectasis, permanent airway injury, and dilatation. This opens the airways up to increased epithelial cell damage, infection, and inflammation. As each
Figure 1: The four pathogenic components of bronchiectasis.
Adapted from Chalmers et al., 20236
Phagocytosis
Reactive oxygen species
NETs/ protease Inflammation
Pulmonary infection and inflammation, MCC dysfunction, and structural lung damage are common features of the pathophysiology of bronchiectasis regardless of cause. The interactions between these four aspects are not best represented as a cycle; this is due to the fact that each of the individual components can independently affect all of the other aspects, and therefore it is better described as a "vicious vortex".
This material has not been reviewed prior to release; therefore, the European Respiratory Society may not be responsible for any errors, omissions or inaccuracies, or for any consequences arising there from, in the content. Reproduced with permission of the ERS 2024. Chalmers JD et al. Basic, translational and clinical aspects of bronchiectasis in adults. Eur Respir Rev. 2023;32(168):230015.
individual component may not only lead to, but also be brought about by, one of the others, and they do not necessarily occur in any particular sequence, the model of bronchiectasis has moved from being seen as a ‘vicious cycle’ to being recognised as a ‘vicious vortex.’1,7
The Role of Neutrophils in Bronchiectasis
Neutrophils usually contribute to acute infection control in a number of ways, including phagocytosis of pathogens,
release of granule-resident cytotoxic and microbicidal molecules, extrudation of neutrophil extracellular traps, and generation of reactive oxygen and nitric oxide species. Neutrophils can also have a large influence on the activity of other immune cells, including macrophages and T cells.8 Such actions are usually relatively time-limited; however, a key feature of bronchiectasis is persistent overabundant neutrophil infiltration into the airways that helps drive the viscous vortex through inflammation and promotion of bacterial colonisation.7
Typically, neutrophils survive for only short periods of time; however, in bronchiectasis, their lifespan can be extended in response to bacterial products, cytokines, and interferons.7 Additionally there is a decrease in neutrophil apoptosis and impaired phagocytosis, compared with healthy controls.9
The primary protease involved in tissue damage and remodelling in bronchiectasis is neutrophil elastase. During neutrophil maturation, this protease is activated by dipeptidyl peptidase 1 (DPP1) in the bone marrow, prior to packaging into granules.10 Neutrophil elastase overabundance, along with other proteases, such as cathepsin, matrix metalloproteinase, and proteinase 3 may occur over anti-proteases such as alpha-1 antitrypsin, alpha-1 macroglobulin, secretory leukocyte protease inhibitor, and elafin.11,12 This imbalance, Goeminne posited, may be a key driver of bronchiectasis. Indeed, neutrophil elastase is found in high
concentrations in patients with a number of neutrophil-associated lung diseases, including bronchiectasis11 and there is a significant positive relationship between the level of this protease and bacterial load in bronchiectasis.11,13 The pathogenesis of lung damage associated with neutrophil elastase release includes activation of pro-inflammatory cytokines and pathways; impaired immune cell function; goblet cell metaplasia and increased airway mucin expression and dehydration; impaired ciliary motility; and epithelial cell apoptosis and impaired proliferation.11,14
Bronchiectasis Exacerbations
Exacerbations in bronchiectasis are important clinical entities to identify, and while precise definitions may vary slightly according to different guidelines (Table 1), common to all are a number of signs and symptoms, including increased cough
Table 1: Definition of exacerbation according to different guidelines.
Guideline
2010 British Thoracic Society guidelines15
2016 consensus definition for clinical research16
2017 Spanish Society of Pulmonology guidelines17
2024 German guidelines (Deutsche Gesellschaft für Pneumologie und Beatmungsmedizin e.V.)18
Recommendations
Worsening of one or more of: sputum volume or purulence, dyspnoea, cough, or lung function decline. Increased fatigue/malaise.
New appearance of one or more of: fever, pleurisy, haemoptysis, or requirement of antibiotic treatment.
Deterioration in ≥3 of the following symptoms for at least 48 hours: cough, sputum volume and/or consistency, sputum purulence, breathlessness and/or exercise tolerance, fatigue and/or malaise, and haemoptysis and a clinician-determined change in bronchiectasis treatment.
Increasing cough and changes in sputum characteristics (increased volume, thicker consistency, greater purulence).
May be accompanied by: worsening dyspnoea, fever, asthenia, general discomfort, anorexia, weight loss, chest pain, haemoptysis, changes in thoracic objective exam, need for bronchiectasis treatment changes, and declining lung function.
Worsening of ≥3 of the following for ≥48 hours: sputum volume and/or consistency; tiredness, fatigue, and/or malaise; new/increased: cough; sputum purulence; haemoptysis; shortness of breath; and/or worsened exercise tolerance. Alternative causes ruled out or unlikely; therapy change necessary.
Exacerbation diagnosis supported by: fever/temperature ≥38 °C, saturation of peripheral oxygen <92% or respiratory rate ≥30 /min, pleuritic chest pain, change in auscultation findings, increased systemic inflammatory values, lung function deterioration, and chest X-ray changes.
and sputum purulence, volume, and/or consistency; decreased lung function; exercise intolerance and/or worsening dyspnoea; increased fatigue and/or feelings of malaise; new or increased haemoptysis; and a change required in current treatment. Also present may be fever, pleurisy, chest pain, and asthenia.15-18 However, Shteinberg discussed that typically, lung infiltrates are not shown on X-ray, and fever may not be present, so these should not be relied upon to make a positive diagnosis. Importantly, Goeminne highlighted, is the role of a healthcare professional in interpreting clinical signs and symptoms as a bronchiectasis exacerbation so that appropriate supportive treatments can be initiated.
In the study utilising EMBARC data, patients had a median of two exacerbations per year, with approximately 40% having at least three per year and over a quarter (26.4%) being hospitalised during an exacerbation in the year prior to the study. Bronchiectasis was generally more severe in Eastern and Central Europe than in other regions. Patients in these parts of Europe also had increased exacerbation frequency, and 57.9% had exacerbations leading to hospitalisation.5 These findings, said Shteinberg, illustrate how common bronchiectasis exacerbations are.
Exacerbation Risk Factors
The highest risk for bronchiectasis exacerbations, as shown in a study including 2,572 patients in Europe, is the number of previous exacerbations. Here, the adjusted incidence rate ratio of a future exacerbation following one exacerbation was 1.81 (95% CI: 1.54, 2.12; p<0.0001), following two exacerbations was 3.07 (95% CI: 2.62, 3.60; p<0.0001), and following three or more exacerbations was 5.18 (95% CI: 4.51, 5.95; p<0.0001), all compared to no exacerbations. Risk of future exacerbations was also associated with type of infection (greater with H. influenzae or P. aeruginosa) and comorbid medical condition (most notably COPD).19
As expected, there is an intimate relationship between lung function and bronchiectasis, with one study showing a decline in the
annual rate of forced expiratory volume during the first second (FEV1) of -31.6 mL/ year.20 Lower lung function increases the risk of future exacerbations.19 Additionally, more rapid lung function decline is significantly associated with more hospitalisations and/or intravenous antibiotic treatment needed due to an exacerbation.20
Notable is an association between bronchiectasis exacerbations and cardiovascular events; for example, in 1,230 patients with an exacerbation history, both risk of and time to acute myocardial infarction and congestive heart failure was higher compared to 9,484 patients with no exacerbation history.21 There is also a relationship between the number of exacerbations per year and all-cause mortality, which is particularly increased in patients who have ≥3 exacerbations per year.19
Bronchiectasis exacerbations can occur due to exogenous triggers such as pathogens6 and pollution levels.22 These may change regional growth characteristics of the disease through mechanisms such as inflammation, immune dysregulation, and cell damage at the DNA and mitochondrial level.23 There may also be changes in the endogenous microbiome during exacerbations whereby they shift from a less interactive to an ‘antagonistic’ relationship.24 This may occur due to changes in regional growth characteristics of the disease, as well as to changes in microbial immigration and elimination, epithelial cell interactions, and inflammatory cell concentration and activation.25,26
Neutrophils and Eosinophils in Bronchiectasis Exacerbations
Neutrophil activity is a key endogenous trigger of exacerbations. Neutrophil elastase activity is associated with increased exacerbation risk as well as with disease severity, as evidenced by clinical and radiological extent of bronchiectasis, sputum volume, and lung function decline (both occurrence and rate).11,27,28 There is also a correlation between resolution of neutrophil elastase activity after antibiotic treatment for an exacerbation,13 with neutrophil
bacterial phagocytosis and killing ability only increasing following antibiotic administration.9
Notably, an association is shown between neutrophil elastase activity and post-exacerbation hospital admission, shorter time to next severe exacerbation requiring hospitalisations or intravenous antibiotic use, and all-cause mortality.11 There is also evidence of a relationship between high neutrophil extracellular trap concentration (>20 mg/mL) and both occurrence of, and shorter time to, bronchiectasis exacerbations.29
While approximately 80% of patients with bronchiectasis are classified as ‘neutrophilic’, with blood eosinophil counts <150 cells/mL, the remaining 20% are considered ‘eosinophilic’, with blood eosinophil counts >300 cells/mL and/or sputum eosinophils >3. Characteristics of such patients include having severe disease, frequent exacerbations, no history of asthma or allergic bronchopulmonary aspergillosis, and possible involvement of P. aeruginosa.30 A relationship is shown between higher eosinophil count and higher annual hospitalisation and exacerbation rates, with the highest levels when blood eosinophil counts are >300 cells/mL. A role of these inflammatory mediators is also shown as treatment with inhaled corticosteroids of patients with eosinophils >300 cells/mL leads to lower annual bronchiectasis-related hospitalisation and exacerbation rates compared to those with low (<100 cells/ mL) or interim (101–300 cells/mL) blood eosinophil counts.31
Current thinking points to the existence of a number of endotypes of bronchiectasis exacerbations based on neutrophil and eosinophil expression and bacterial species. For example, one study32 showed a neutrophilic and Pseudomonas dominated endotype, an eosinophilic endotype with no specific dominance, a Haemophilus dominated endotype that had a bacterial response, and a Streptococcus dominated endotype with excess mucus production. Differences between these endotypes were shown in neutrophil elastase activity and in the expression
of the pro-inflammatory cytokine IL-1b and the hormone resistin.32 These are exciting findings regarding bronchiectasis, explained Goeminne, “as we are now realising how important inflammation really is.”
Exacerbations and Health-Related Quality of Life
The European study discussed above (n=2,572) investigated the impact of exacerbations on HRQoL utilising the St. George’s Respiratory Questionnaire (SGRQ), which assesses disease-specific health status for asthma and COPD. This is scored on a scale from 0−100 (where a higher score indicates worse HRQoL), with a minimal clinically important difference of around 4.0 points.33 Here, the median SGRQ total score increased according to the number of exacerbations per year, with each additional exacerbation leading to a significant 3.7-point score increase (95% CI: 2.58, 4.87; p<0.0001). Investigation of the data according to hospitalisations found that while there was a 1.4-point increase for each individual outpatient exacerbation (95% CI: 0.57, 2.07; p=0.001), there was a 9.8-point increase for patients with a history of hospitalised exacerbations (95% CI: 6.28, 13.3; p<0.0001).19 These findings echo patient testimony shown as part of the symposium regarding how exacerbations, particularly, can impact their HRQoL.
Management of Bronchiectasis Exacerbations
The American Lung Association suggests a number of ways to help manage bronchiectasis symptoms and limit flareups, including quitting smoking and avoiding second-hand smoke; maintaining a healthy diet and staying hydrated; taking medications as prescribed and staying upto-date with recommended vaccinations; as well as performing daily mucus clearance techniques.34 However, despite prevention and management strategies, around 75% of patients with bronchiectasis experience exacerbations,5 and challenges remain regarding identifying biomarker triggers and
<<< Width of figure size on page >>>
Understanding the interaction between pathogens, pollutants, and inflammation
Overcoming
Identifying biomarkers for different exacerbation triggers
Challenges
antibiotic-resistance by identifying resistance genes
resistance genes to help target treatments, and understanding the interactions between triggers and bronchiectasis-associated inflammation (Figure 2).
Defined airway clearance techniques, as taught by a respiratory physiotherapist, are part of exacerbation management recommended in British Thoracic Society (BTS) guidelines for all patients with bronchiectasis.36 While these are recommended both during and between exacerbations, Shteinberg discussed how, for patients with mild exacerbations, increased airway clearance should be the first step recommended, reviewing their progress after 2−3 days to ascertain if further treatment is needed. The BTS also recommend using postural drainage, which may be modified and targeted in patients with radiological changes, and, for patients with ongoing airway clearance difficulties, addition of manual techniques, use of positive pressure devices, and enhanced airway humidification/hydration using isotonic or hypertonic saline if secretions are viscous.36
Identifying ways to reduce antibiotic treatment, including use of antivirals and anti -inflammatories
Antibiotics and Other Treatments
According to BTS
36 and ERS37 guideline recommendations, the primary treatment for acute bronchiectasis exacerbations is antibiotics. Of note, however, recommendations may be based on lowquality evidence.36,37 Eradication is not a treatment goal, discussed Shteinberg, “rather, the rationale in treating with antibiotics is to reduce bacterial load in the airways, which improves symptoms”.13 According to these guidelines, standard antibiotic treatment is for 14 days, although shorter periods may be considered in patients with variable disease severity or activity.36,37 The BTS guidelines recommend intravenous antibiotics in patients who are ‘particularly unwell, have resistant organisms, or who fail to respond to oral therapy’.36 Antibiotic choice can be guided by the identification of bacterial genus and species,38 and it is recommended that such treatment is always used if a patient is infected with P. aeruginosa.36,37
Shteinberg echoed good practice points from the BTS when discussing her patient consults. These include initiating empiric antibiotics while awaiting microbiology results, taking into account results from previous exacerbations. Once microbiology results are received, antibiotic choice can be adjusted if needed.
36
Figure 2: Challenges in the clinical management of exacerbations.24,35
Microbial response to an antibacterial agent is typically assessed using one of several in vitro ‘antimicrobial susceptibility testing’ methods. However, these do not necessarily reflect lung diseases where there may be polymicrobial infection, anaerobic airway niches, and diversity in biofilm growth and phenotype.39 As such, instead of antimicrobial susceptibility testing, Shteinberg discussed how one challenge in bronchiectasis is the need to use genotyping methods to identify antibiotic-resistance genes (Figure 2).24 Another difficulty with regard to antibiotic use is that their primary action in the airways is usually only at the level of the mucus layer, which contains far fewer bacteria than in the underlying biofilm due to inactivation by material released from bacteria therein.40
Studies point to the feasibility of shortening the 14 days recommended for antibiotic use during exacerbations. For example, in one study involving patients with severe pulmonary exacerbations treated with an intravenous antibiotic, 47 were administered 14 days’ treatment and 43 were treated according to bacterial load in sputum samples (bacterial load-guided group: BLGG). Results demonstrated that, on Day 7, 84% of all participants in both groups showed colony-forming units per mL <106. This meant that in the BLGG, bacterial load was considered low enough that treatment could be stopped in 88% of patients on Day 8. In all other participants in the BLGG, treatment could be stopped on Day 11. While clinical recovery was not affected by group, time to next exacerbation was significantly sooner in the 14-day group compared to the BLGG (p=0.0034).41
Studies have also assessed dual antibiotic use, taking advantage of different delivery methods. In one double-blind, randomised study, an oral antibiotic was combined with either an inhaled antibiotic or a placebo in 53 patients with bronchiectasis and chronic P. aeruginosa infection. At Day 21,
References
1. Chan ED et al. Diagnostic evaluation of bronchiectasis. Respiratory Medicine: X. 2019;1:100006.
no differences were found in bacterial load or clinical outcome, which, the authors postulated, may have been related to the finding of more treatment-related wheeze in the inhaled antibiotic group compared with the placebo group.42
Shteinberg also highlighted the challenge of needing to find ways to reduce antibiotic use (antibiotic resistance), for example, by understanding if exacerbations are caused by viral infection, pollutants, or host inflammatory responses (Figure 2).35 Other treatments for bronchiectasis include mucolytics, the use of which is associated with significant improvements in expectoration, sputum volume, auscultatory findings, and FEV1 43 As bronchiectasis is associated with inflammation,1 an antiinflammatory agent may be prescribed during acute exacerbations. However, in a singlecentre, retrospective study (n=43), the use of systemic glucocorticoids in such cases was associated with significantly increased in-hospital mortality (p=0.0474).44
Conclusion
Overall, this symposium highlighted how both patients and their primary healthcare providers need to be educated in identifying bronchiectasis exacerbations and in understanding the impact of exacerbations on a patient’s general health and HRQoL. Daily airway clearance techniques should be taught and escalated if needed during exacerbations, and discussion of antibiotic treatment should include details of how this should result in clinical improvement but may not lead to pathogen eradication. Challenges that remain regarding clinical management of bronchiectasis exacerbations include understanding the interaction between associated triggers35 and identifying biomarkers for such,24 as well as providing clinically evidenced treatment regimens.
2. Quint JK et al. Changes in the incidence, prevalence and mortality of bronchiectasis in the UK from 2004 to 2013: a population-based cohort study. Eur Respir J. 2016;47(1):186-93.
3. Weycker D et al. Prevalence and incidence of noncystic fibrosis bronchiectasis among US adults in 2013. Chron Respir Dis. 2017;14(4):377-84.
4. Feng J et al. Increasing prevalence and burden of bronchiectasis in urban Chinese adults, 2013-2017: a nationwide population-based cohort
study. Respir Res. 2022;23(1):111.
5. Chalmers JD et al. Bronchiectasis in Europe: data on disease characteristics from the European Bronchiectasis registry (EMBARC). Lancet Respir Med. 2023;11(7):637-49.
6. Chalmers JD et al. Basic, translational and clinical aspects of bronchiectasis in adults. Eur Respir Rev. 2023;32(168):230015.
7. Watt AP et al. Neutrophil apoptosis, proinflammatory mediators and cell counts in bronchiectasis. Thorax. 2004;59(3):231-6.
8. Perobelli SM et al. Plasticity of neutrophils reveals modulatory capacity. Braz J Med Biol Res. 2015;48(8):665-75.
9. Bedi P et al. Blood Neutrophils are reprogrammed in bronchiectasis. Am J Respir Crit Care Med. 2018;198(7):880-90.
10. Palmér R et al. Dipeptidyl peptidase 1 inhibitor AZD7986 induces a sustained, exposure-dependent reduction in neutrophil elastase activity in healthy subjects. Clin Pharmacol Ther. 2018;104(6):1155-64.
11. Chalmers JD et al. Neutrophil elastase activity is associated with exacerbations and lung function decline in bronchiectasis. Am J Respir Crit Care Med. 2017;195(10):1384-93.
12. Polverino E et al. The role of neutrophil elastase inhibitors in lung diseases. Chest. 2017;152(2):249-62.
13. Chalmers JD et al. Short- and longterm antibiotic treatment reduces airway and systemic inflammation in non-cystic fibrosis bronchiectasis. Am J Respir Crit Care Med. 2012;186(7):657-65.
14. Voynow JA, Shinbashi M. Neutrophil elastase and chronic lung disease. Biomolecules. 2021;11(8):1065.
15. Pasteur MC et al. British Thoracic Society guideline for non-CF bronchiectasis. Thorax. 2010;65(Suppl 1):i1-58.
16. Hill AT et al. Pulmonary exacerbation in adults with bronchiectasis: a consensus definition for clinical research. Eur Respir J. 2017;49(6):1700051.
17. Martínez-García M et al. Spanish Guidelines on the evaluation and diagnosis of bronchiectasis in adults. Arch Bronconeumol (Engl Ed). 2018;54(2):79-87.
18. Ringshausen FC. Management erwachsener Patientinnen und Patienten mit Bronchiektasen-
Erkrankung (Management of adult patiens with bronchiectasis disease). Available at: https://www.pcd-ks. info/files/B0C5V2I/s2k_leitlinien_ bronchiektasen_2024_06.pdf. Last accessed: 4 October 2024.
19. Chalmers JD et al. Characterization of the "frequent exacerbator phenotype" in bronchiectasis. Am J Respir Crit Care Med. 2018;197(11):1410-20.
20. Martinez-García MA et al. Pseudomonas aeruginosa and lung function decline in patients with bronchiectasis. Clin Microbiol Infect. 2021;27(3):428-34.
21. Kwok WC et al. Cardiovascular outcomes following hospitalisation for exacerbation of bronchiectasis: a territory-wide study. BMJ Open Respir Res. 2024;11(1):e001804.
22. Goeminne PC et al. The impact of acute air pollution fluctuations on bronchiectasis pulmonary exacerbation: a casecrossover analysis. Eur Respir J. 2018;52(1):1702557.
23. Eckhardt CM, Wu H. Environmental exposures and lung aging: molecular mechanisms and implications for improving respiratory health. Curr Environ Health Rep. 2021;8(4):281-93.
24. Mac Aogáin M et al. Integrative microbiomics in bronchiectasis exacerbations. Nat Med. 2021;27(4):688-99.
25. Dickson RP et al. Spatial variation in the healthy human lung microbiome and the adapted island model of lung biogeography. Ann Am Thorac Soc. 2015;12(6):821-30.
26. Dickson RP et al. Towards an ecology of the lung: new conceptual models of pulmonary microbiology and pneumonia pathogenesis. Lancet Respir Med. 2014;2(3):238-46.
27. Tsang KW et al. Sputum elastase in steady-state bronchiectasis. Chest. 2000;117(2):420-6.
28. Gramegna A et al. Sputum neutrophil elastase in bronchiectasis: a Southern European cohort study. Eur Respir J. 2020;DOI:10.1183/13993003.017022020
29. Keir HR et al. Neutrophil extracellular traps, disease severity, and antibiotic response in bronchiectasis: an international, observational, multicohort study. Lancet Respir Med. 2021;9(8):873-84.
30. Pollock J, Goeminne PC. Eosinophils in bronchiectasis: a u-turn for bronchiectasis management. Chest. 2023;164(3):561-3.
31. Oscullo G et al. Bronchiectasis-COPD overlap syndrome: role of peripheral eosinophil count and inhaled corticosteroid treatment. J Clin Med. 2023;12(19):6417.
32. Gao Y et al. Endotypes of exacerbation in bronchiectasis: an observational cohort study. Am J Respir Crit Care Med. 2024;210(1):77-86.
33. Jones PW. St. George's Respiratory Questionnaire: MCID. Copd. 2005;2(1):75-9.
34. Association AL. Treating and managing bronchiectasis. Available at: https:// www.lung.org/lung-health-diseases/ lung-disease-lookup/bronchiectasis/ treating-and-managing. Last accessed 4 October 2024.
35. Choi H, Chalmers JD. Bronchiectasis exacerbation: a narrative review of causes, risk factors, management and prevention. Ann Transl Med. 2023;11(1):25.
36. Hill AT et al. British Thoracic Society Guideline for bronchiectasis in adults. Thorax. 2019;74(Suppl 1):1-69.
37. Polverino E et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur Respir J. 2017;50(3):1700629.
38. Zemanick E et al. Antimicrobial resistance in cystic fibrosis: a Delphi approach to defining best practices. J Cyst Fibros. 2020;19(3):370-5.
39. Kidd TJ et al. Defining antimicrobial resistance in cystic fibrosis. J Cyst Fibros. 2018;17(6):696-704.
40. Tan M et al. Magnetic nanoparticlebased drug delivery approaches for preventing and treating biofilms in cystic fibrosis. Magnetochemistry. 2020;6(4):72.
41. Bedi P et al. Feasibility of shortening intravenous antibiotic therapy for bronchiectasis based on bacterial load: a proof-of-concept randomised controlled trial. Eur Respir J. 2021;58(6):2004388.
42. Bilton D et al. Addition of inhaled tobramycin to ciprofloxacin for acute exacerbations of Pseudomonas aeruginosa infection in adult bronchiectasis. Chest. 2006;130(5):1503-10.
43. Olivieri D et al. Role of bromhexine in exacerbations of bronchiectasis. Double-blind randomized multicenter study versus placebo. Respiration. 1991;58(3-4):117-21.
44. Finklea JD et al. Predictors of mortality in hospitalized patients with acute exacerbation of bronchiectasis. Respir Med. 2010;104(6):816-21.
Abstract Reviews
Explore the latest developments in respiratory health with novel abstracts presented by experts in the field at the European Respiratory Society (ERS) Congress 2024. Read on for their fascinating insights.
Antifibrotic Treatment Efficacy in Progressive Pulmonary Fibrosis: Single Centre Experience
In cases of pulmonary fibrosis attributable to interstitial lung disease, whether the aetiology is known or unknown, the presence of at least two out of three criteria defined as worsening respiratory symptoms, functional impairment, and radiological progression within the past year characterises progressive pulmonary fibrosis (PPF).1-3 There are several diseases that can lead to PPF, and there is insufficient experience with antifibrotic treatment in patients other than those with idiopathic pulmonary fibrosis (IPF). This study aims to investigate the effectiveness of antifibrotic therapy in the treatment of cases with PPF other IPF.
METHOD
Patients followed up at the Interstitial Lung Diseases Outpatient Clinic of the Department of Chest Diseases, Istanbul University Faculty of Medicine, Türkiye, diagnosed with PPF according to the current guidelines, were included in the study.1,2 Patients under 18 years of age, those with transaminases or bilirubin levels >1.5 times the upper limit of normal, those with creatinine clearance <30 mL/min, and those with chronic liver disease were excluded from the study. Demographic characteristics, clinical features, comorbidities, blood oxygen saturation (SpO2), 6-minute walking distance (6MWD), spirometry, and diffusing capacity measurements of patients using antifibrotics for at least 6 months were recorded. Functional parameters at 6 months and 1 year of treatment were compared with baseline data.
RESULTS
In accordance with the guidelines, 105 cases diagnosed with PPF and under antifibrotic treatment were included in the study. Thirty-seven percent of the cases (n=39) had systemic sclerosis, 16% (n=15) had hypersensitivity pneumonitis, 11% (n=12) had rheumatoid arthritis, and in 37% (n=38) of the cases there was lung involvement associated with other systemic diseases (Table 1). The majority of cases (n=91; 86.7%) were using nintedanib, while
14 cases were using pirfenidone. The most common side effect associated with nintedanib use was diarrhoea (n=10; 10%), followed by elevated liver function tests (n=12; 11%). Treatment was discontinued in eight cases with treatment-resistant weight loss, and they were switched to pirfenidone therapy. Four cases discontinued medication therapy during follow-up at their own request. Fifteen cases (14.3%) were lost during the course of antifibrotic use. At 6 months, functional evaluation was available for 58 cases, and at 1 year, it was available for 36 cases. In the pre-antifibrotic treatment evaluation, the mean forced vital capacity (FVC) was 1975.05±650.598 mL
Table 1: Subgroup diseases of the patient population.
(range: 730–3,800), FVC% was 65.367%, diffusing capacity for carbon monoxide (DLCO) was 47.15±14.796% (range: 17–80), and 6MWD was 403.89±89.148 m (range: 105–600). At the 6-month mark, the mean FVC was 2079.12±682.368 mL (range: 730–3,500), FVC% was 67.22% (range: 23–143), DLCO was 49±14.2% (range: 17–85), and 6MWD was 443.43±72.629 m (range: 260–550) (Table 2).
At the end of 1 year of treatment, FVC was determined to be 2051.53±619.833 mL, FVC% was 68.22±22.271% (range: 33–145), DLCO was 48.53±16.168% (range: 12–80), and 6MWD was 424.94±97.680 m
N/A: not applicable; NSIP: non-specific interstitial pneumonia; PPFE: pleuroparenchymal fibroelastosis.
Table 2: Functional changes of the study population after treatment.
6MWD: 6-minute walking distance; DLCO: diffusing capacity of the lungs for carbon monoxide; FVC: forced vital capacity.
(range: 47–583). When compared with baseline values, there was no significant loss in FVC and DLCO at 6 months and 1 year. However, there was a significant increase in 6MWD (p<0.001 at 6 months; p<0.001 at 1 year). Except for the 12 cases identified with exertional desaturation during the pretreatment functional assessment, no new cases with exertional desaturation were observed during follow-up.
CONCLUSION
No significant functional changes were observed in the 6-month functional assessment of PPF cases under nintedanib treatment. Our results suggest that rapid functional decline can be prevented with nintedanib therapy. In light of the available data, large-scale prospective studies are needed to demonstrate the efficacy
of antifibrotic treatment in different PPF subgroups.4
References
1. Raghu G et al. Idiopathic pulmonary fibrosis (an Update) and progressive pulmonary fibrosis in adults: an official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med 2022;205(9):e18-47.
2. Turkish Thoracic Society. Idiopathic Pulmonary Fibrosis (IPF) and progressive pulmonary fibrosis (PPF) Diagnosis and Treatment Concensus Report. 2023. Available at: https://toraks.org.tr/ site/community/library/bRhTSGc0ZBpE7M_B. Last accessed: 1 May 2023.
3. Travis WD et al. An official American Thoracic Society/European Respiratory Society statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188(6):733-48.
4. Iwanami Y et al. Benefits of pulmonary rehabilitation in patients with idiopathic pulmonary fibrosis receiving antifibrotic drug treatment. J Clin Med. 2022;11(18):5336.
Inhalation Innovation: Phase IIb Study Design
of Inhaled Pirfenidone in the Treatment of Progressive Pulmonary Fibrosis
Authors: Martin Kolb,1 Colin Reisner,2 Deepthi
Nair,3 Felix Woodhead,3 Howard Lazarus,3
*Craig Conoscenti3
1. McMaster University, Hamilton, Canada
2. DevPro Biopharma, Basking Ridge, New Jersey, USA
3. Avalyn Pharma, Cambridge, Massachusetts, USA
*Correspondence to cconoscenti@avalynpharma.com
Disclosure: Kolb has received payment from Avalyn Pharma for providing advice for the MIST trial; has received research funding for preclinical work from Boehringer Ingelheim, United Therapeutics, and Structure Therapeutics; has received consulting fees from Boehringer Ingelheim, Roche, Horizon, Abbvie, Bellerophon, Algernon, CSL Behring, United Therapeutics, Fortrea, Structure Therapeutics, Astra Zeneca, Sanofi, GSK, Pliant, Avalyn, and Trevi; has received payments or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Glenmark, Novartis, and Boehringer Ingelheim; and payment for expert testimony from Roche. Reisner is the CEO and
co-founder of DevPro Biopharma and has provided consultation and consulting fees from Avalyn Pharma on the design and implementation of this study; has grants and contracts with multiple pharma companies under confidentiality; has stock options in Astrazeneca, Immunocore, Albus Health, Novo, Sandoz and is an individual investor in multiple companies that DevPro Biopharma does not work with directly. Nair and Woodhead have received all the support for this manuscript from Avalyn Pharma as an employee; has stock options in Avalyn Pharma as an employee. Lazarus has received all the support for this manuscript from Avalyn Pharma as an employee. Conoscenti has received all the support for this manuscript from Avalyn Pharma as an employee; has stock options in Avalyn Pharma as an employee and receives salary from the same as an employee. Conoscenti all the support for this manuscript as the drug developer from Avalyn Pharma; has stock options at Avalyn Pharma and receives salary from the same as an employee. The authors declare no conflict of interest.
Screening period (up to 28 days), including at least 1 week of saline nebulisation.
Baseline (Day 1)
52-Week Double-blind Treatment Period
Randomisation to treatment (2:1:2)
BID: twice daily; TC: telephone call.
INTRODUCTION
Progressive pulmonary fibrosis (PPF) is an increasingly recognised condition, defined in 2022 to address the progression of pulmonary fibrosis in patients with interstitial lung diseases (ILD) other than idiopathic pulmonary fibrosis (IPF).1 Oral pirfenidone has been studied in non-IPF ILDs but never achieved a statistically significant change in the primary endpoint. Trends seen in secondary endpoints support efficacy in PPF.2-4
OBJECTIVE
Data from the AP01-002 (ATLAS) Study of inhaled pirfenidone in IPF demonstrated efficacy and improved safety compared to that seen with oral pirfenidone.5 The AP01007 (MIST Study, Figure 1) is designed to study the efficacy and safety of AP01 (aerosolised pirfenidone) in patients with PPF. Patients will remain on background immunosuppression, and up to 30% of patients will remain on background nintedanib therapy.
Figure 1: MIST study design.
METHODS
The primary objective is to observe the change in the annual rate of decline in forced vital capacity in the AP01 treatment groups as compared to placebo. In addition, efficacy will be measured in secondary endpoints of time to progression, change in 6-minute walk test, change in fibrotic scores via quantitative high-resolution CT, and change from baseline quality of life. Safety outcomes will be assessed as well. Cough will be analysed through cough counts and cough questionnaires, which should allow differentiation of cough related to PPF versus the nebulisation procedure.
CONCLUSION
MIST will study the safety and efficacy of AP01 (aerosolised pirfenidone) in patients with PPF. In addition to the safety and efficacy endpoints, MIST will carefully
examine the presence of cough in this population of patients.
References
1. Raghu et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: an official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am J Respir Crit Care Med. 2022;205(9)e18-47.
2. Maher et al. Pirfenidone in patients with unclassifiable progressive fibrosing interstitial lung disease: a double-blind, randomised, placebocontrolled, phase 2 trial. Lancet Respir Med. 2020;8(2):147-57.
3. Behr et al. Pirfenidone in patients with progressive fibrotic interstitial lung diseases other than idiopathic pulmonary fibrosis (RELIEF): a doubleblind, randomised, placebo-controlled, phase 2b trial. Lancet Respir Med. 2021;9(5):476-86.
4. Fernandez-Perez et al. Pirfenidone in fibrotic hypersensitivity pneumonitis: a double-blind, randomised clinical trial of efficacy and safety. Thorax. 2023;78(11)1097-104.
5. West A et al. Inhaled pirfenidone solution (AP01) for IPF: a randomised, open-label, dose-response trial. Thorax. 2023 Sep;78(9):882-9.
The following abstract highlights spotlight selected abstracts presented at the European Respiratory Society (ERS) Congress 2024. They cover key topics, including lung cancer screening and management, Chronic obstructive pulmonary disease, cystic fibrosis, effects of smoking on airway inflammation, and the role of biologic therapy in asthma. These highlights showcase the latest cutting-edge developments and most talked-about topics in the field today.
Hyperpolarised 129-Xenon MRI Shows Promise for Measuring Lung Function in PF-ILD
A STUDY presented at the 2024 ERS Congress demonstrated how a novel MRI technique using hyperpolarised 129-Xenon gas could revolutionise how doctors assess gas transfer in patients with progressive fibrosing interstitial lung disease (PF-ILD).
PF-ILD is a group of diseases that lead to scarring in the lung tissue, causing reduced lung capacity and impaired gas exchange. Typically, healthcare professionals use the single-breath carbon monoxide uptake test to measure overall gas transfer capacity in the lungs. However, this test doesn’t capture regional variations in gas transfer, which may be crucial for understanding how the disease progresses in different areas of the lungs.
The new technique involves inhaling hyperpolarised 129-Xenon (HP 129Xe) gas, which acts as a contrast agent during an MRI scan. As the gas is absorbed into the lung tissue and binds to red blood cells, the MRI can distinguish between gas in the airways and gas that has dissolved into the blood, allowing researchers to measure regional gas transfer. The ratio of red blood cell-bound gas to tissue-bound gas is used as an indicator of pulmonary gas transfer efficiency.
The MRI can distinguish between gas in the airways and gas that has dissolved into the blood, allowing researchers to measure regional gas transfer
Preliminary results from three patients showed a lower red blood cell ratio in lung regions affected by fibrosis, compared to healthy controls reported in literature. This regional imaging technique also showed a strong correlation with traditional single-breath carbon monoxide uptake measurements, supporting its potential clinical utility.
The study suggests that hyperpolarized 129-Xenon MRI could provide a more detailed understanding of lung function in patients with PF-ILD, potentially aiding in earlier diagnosis and more targeted treatments.
Impact of Lung Cancer Screening on Early Diagnosis and Management of Interstitial Lung Disease
A STUDY was recently presented at the 2024 ERS Congress examining the impact of lung cancer screening on the timely diagnosis of interstitial lung disease (ILD).
In 2023, 5,110 CT scans were performed in southeast London, leading to 39 referrals to the ILD service.
Patients with ILD often face delays of about 2.3 years from symptom onset to diagnosis, leading to worse outcomes. A pilot programme in the UK, the Targeted Lung Health Check (TLHC), screens individuals aged 55–74 years with a smoking history via CT scans.
A pilot programme in the UK, the Targeted Lung Health Check (TLHC), screens individuals aged 55–74 years with a smoking history via CT scans
In 2023, 5,110 CT scans were performed in southeast London, leading to 39 referrals to the ILD service. Of those referred, 33 (87%) were assessed, and 26 were diagnosed with ILD, including 11 smoking-related cases. Notably, 14 patients had minimal or no symptoms, indicating early-stage disease. Around 30% of patients were discharged without needing further care, and 18% received treatments like immunosuppressives or antifibrotics. The average time from CT scan to ILD diagnosis was 77 days (range: 19–168 days; median: 74 days).
The study concludes that lung cancer screening can shorten the time to ILD diagnosis, allowing earlier treatment and potentially preventing severe lung damage. It suggests refining referral criteria to improve efficiency and reduce the burden on ILD services.
Periodontal Therapy Shows Potential to Enhance Lung Function
A CHRONIC inflammatory disease caused by bacterial infections in the gums, periodontitis, is known to affect overall health; however, its potential influence on respiratory health remains unclear.
A study presented at the ERS Congress 2024 aimed to investigate whether periodontal therapy, which involves the removal of dental biofilm, could reduce the presence of harmful bacteria and improve lung function by decreasing inflammation in the lungs.
A total of 62 patients with periodontitis, who were non-smokers and free from other medical conditions, were recruited for this investigator-masked clinical trial. Periodontal health was assessed through full-mouth recordings of periodontal pockets, clinical attachment loss, and bleeding on probing. Participants underwent a comprehensive periodontal therapy involving a full-mouth disinfection protocol.
Lung function was assessed using the forced oscillation technique to measure airway resistance (Rrs) and reactance (Xrs). Spirometry was also conducted to measure forced expiratory volume in 1 second, forced vital capacity, and the forced expiratory volume in 1 second/forced vital capacity ratio. These assessments were conducted at baseline (T0) and 3 and 6 weeks posttherapy (T1). Changes in lung function were analysed using a linear mixed-effects model.
The results indicated that all participants showed significant improvement in
periodontal health (p<0.001) following therapy. At baseline, lung function was within the normal range for all participants. Post-therapy, airway resistance at 11 Hz and 19 Hz decreased by 4.7% and 5.4%, respectively (p<0.05). A trend suggesting a 3.4% reduction in R5, an oscillometry variable, was also observed (p=0.054), although no significant changes were seen in spirometric variables or Xrs indices.
Post-therapy, airway resistance at 11 Hz and 19 Hz decreased by 4.7% and 5.4%, respectively
The study demonstrated that periodontal therapy can significantly reduce airway resistance, suggesting a potential link between periodontal infection control and improved respiratory health. These findings highlight the need for further research, including larger randomised controlled trials, to explore the broader impact of periodontitis prevention and treatment on lung function and respiratory outcomes.
The Effect of Smoking and Airway Inflammation on IL-33 Levels
THE RELATIONSHIP between smoking status, airway inflammation, and IL-33 expression in patients with asthma or chronic obstructive pulmonary disease (COPD) has been a growing area of interest in respiratory research over recent years.
Previous studies have shown that IL-33 may be influenced by smoking and the nature of airway inflammation. This study, presented at the 2024 ERS Congress, aimed to explore the association between IL-33 levels in sputum and these factors in patients with asthma, COPD, and healthy controls.
The study included patients with various severity levels of COPD, individuals with severe asthma, and a group of healthy controls. Airway inflammation was characterised using specific cutoffs for eosinophilia, defined as eosinophil levels ≥2%, and neutrophilia, defined as neutrophils ≥50%, while IL-33 levels in sputum were measured through a digital single-molecule assays.
The results indicated that IL-33 levels were significantly higher in patients with COPD and severe asthma, with median levels of 38.7 pg/mL and 32.0 pg/mL, respectively, compared to the healthy controls (14.1 pg/ mL). Among COPD patients, former smokers had IL-33 levels of 64 pg/mL, significantly higher when compared to 23 pg/mL for active smokers (p=0.002). Further analysis revealed that former smokers with pre-mild or mild-moderate COPD showed elevated IL-33 levels compared to healthy controls. However, both former and active smokers with severe COPD exhibited higher IL-33 levels compared to controls or former smokers with mild-moderate COPD, (p<0.05).
In severe patients with asthma, IL-33 levels did not differ significantly between former smokers and never-smokers (p=0.56), nor between individuals with high or low T2 markers.
Patients with asthma with mixed granulocytic inflammation, however, had significantly higher IL-33 levels than the controls (p=0.014).
These findings suggest that IL-33 may be a promising therapeutic target, particularly for former smokers with COPD. However, in cases of severe COPD, the disease's severity may have a more dominant effect than smoking status. In patients with asthma, targeting IL-33 might be beneficial regardless of T2 inflammation status. These results highlight the complex role of IL-33 in airway diseases, emphasising the need for personalised treatment approaches.
IL-33 may be a promising therapeutic target, particularly for former smokers with COPD
Small Airway Disease Reduces Biologic Therapy Response in Severe Asthma
RESAERCH presented at the ERS Congress 2024 revealed that small airways disease (SAD) in patients with severe asthma predicts a negative response to biologic therapy.
The prevalence of SAD in patients with severe asthma is poorly understood, largely due to challenges in accurately assessing the endobronchial district, and the absence of a definitive gold standard for measurement. Furthermore, only a limited number of studies have explored the correlation between small airway involvement in severe asthma and the response to biological therapies. Therefore, researchers aimed to determine the prevalence of SAD, and response to biologics, in patients with severe asthma.
The study included 160 patients with severe asthma who were either treated with omalizumab (n=60), benralizumab (n=23), mepolizumab (n=32), or dupilumab (n=41). Spirometry and forced oscillation technique (FOT) was used to establish the prevalence of SAD in the cohort. Response to biologics was defined as a complete suspension of systemic corticosteroids and less than two asthma flare-ups 1 year after treatment. Statistical analysis included ANOVA with Bonferroni correction and multivariate linear logistic regression.
The analysis revealed SAD was more prevalent among non-responders, affecting over 50%, as indicated by X5% values below the lower limit of normal, and R5-R20 kPa/L/s values greater than 0.03. Logistic regression analysis further demonstrated that an X5% less than the lower limit of normal is a negative predictive factor for response to biological therapy. Additionally, it was revealed that after 1 year of treatment, patients who received omalizumab showed significantly impaired lung function and a lower response to therapy.
These findings emphasise the need for more comprehensive assessment of small airways when tailoring biologic therapies for severe asthma, as well as further research to optimise treatment strategies for this group of patients.
The study included 160 patients with severe asthma who were either treated with...
(n=60)
(n=23)
mepolizumab (n=32)
dupilumab (n=41)
omalizumab
benralizumab
Among children, the baseline level of TNFα was found to be linked to improved BMI and reduced IgG levels after therapy
The study was conducted on 133 patients with CF, including 65 adults and 68 children. The research analysed the impact of HEMT
Modulator Therapy Boosts Lung Function in Cystic Fibrosis
A STUDY presented at the 2024 ERS Congress has found that highly effective modulator therapy (HEMT) improves lung function and BMI in patients with cystic fibrosis (CF), but its influence on airway inflammation remains uncertain.
The study was conducted on 133 patients with CF, including 65 adults and 68 children. The research analysed the impact of HEMT (elexacaftor/tezacaftor/ivacaftor, symkevi, lumacaftor/ivacaftor) over a 3-month period.
While HEMT led to notable improvements in BMI and lung function in adults and increased lung capacity (measured as forced expiratory volume in 1 second) in children, the therapy did not significantly alter key inflammatory markers, such as neutrophils and IgG, or cytokine levels like TNFα and TNFβ, which are typically associated with inflammation.
Among children, the baseline level of TNFα was found to be linked to improved BMI and reduced IgG levels after therapy. However, this effect was not seen in adults, nor were there any significant changes related to TNFβ levels in either age group.
The study’s findings suggest that HEMT provides more significant clinical benefits for adult patients with CF in the short term, with children potentially needing a longer observation period due to their better baseline health. Further research is needed to understand the therapy's long-term effects on inflammation in patients with CF.
Digital Monitoring and Home Spirometry for Patients with COPD
REMOTE digital monitoring for patients with chronic obstructive pulmonary disease (COPD) following an acute exacerbation is both feasible and safe, with lower-than-expected exacerbation and readmission rates, according to research presented at the ERS Congress 2024.
COPD is a significant public health challenge, with high rates of readmission and mortality after acute exacerbations. Therefore, researchers have sought to use digital tools to improve outcomes in this patient population. Specifically, the feasibility of remote digital monitoring with home spirometry, activity wristbands, and pulse oximeters was assessed in patients recently discharged after an acute COPD exacerbation. Teleconsultations with a pulmonologist and spirometry were conducted every 6 weeks for 3 months.
Data from the wearables, home devices, and patient-reported outcomes were integrated using the DATOS platform, which allowed daily review of the data by a nurse case-manager.
From August 2022–January 2024, 50 patients were recruited, with a median age of 66 years, of which 46% were male, 59% classified as GOLD Stage 3–4, and the mean CAT score was 15.8±9.8. Among the cohort, 37 patients completed followup, there were five exacerbations, and no readmissions. User feedback revealed that the digital tools were user-friendly and well-accepted by patients.
User feedback revealed that the digital tools were user-friendly and well-accepted by patients
The results demonstrate that remote monitoring through digital tools appears to be a feasible and user-friendly approach to managing patients with COPD after acute exacerbations. The reduction in exacerbations and readmissions suggests that home spirometry could serve as an effective alternative to hospital-based care. Future research should focus on refining these digital tools and expanding their use in clinical practice to further improve patient outcomes.
Automated CT with Machine Learning Predicts Functional Decline in Cystic Fibrosis
A DEEP learning model that utilises CT imaging has been shown to predict the rate of decline in forced expiratory volume in the first second (FEV1) in patients with cystic fibrosis (CF).
Clinical trials in CF face challenges due to the variability in measurement of FEV1. Therefore, researchers aimed to explore the use of computer algorithms to quantify airways, fat, and muscle on CT imaging, aiming to identify patients more likely to experience a decline in FEV1
The research team used a deep learning model to automatically segment representative skeletal muscle, subcutaneous fat volumes at the 9th thoracic vertebrae, and patent airway trees. AirQuant, a computational pipeline, was used to measure intersegmental airway tapering and intrasegmental tortuosity in patients with mild-to-moderate disease (FEV1 >40%), and linear mixedeffects models were used to predict FEV1 percentage decline over 1 year.
In a derivation cohort, 25 of 84 patients experienced an FEV1 decline of more than 5%. By maximising the Youden Index, thresholds for muscle, fat, and airway measures that predict an FEV1 decline of more than 5% were identified. These thresholds were tested on a validation cohort (n=74), and prediction accuracy was measured using the area under the curve (AUC).
25 of 84 patients experienced an FEV1 decline of more than 5%
In the validation cohort, 24 of 74 patients exhibited an FEV1 decline of more than 5%. The CT measurements with the highest predictive accuracy in the validation cohort were muscle volume (AUC: 0.63), airway tortuosity (AUC: 0.60), airway intertapering (AUC: 0.57), and fat volume (AUC: 0.56).
The results presented at the 2024 ERS Congress suggest that automated CT measurements can help predict FEV1 decline in patients with CF, offering a potential tool for cohort enrichment in clinical trials. Future research should explore the utility of these algorithms in clinical practice, particularly in tailoring treatment and intervention strategies.
Congress Interview
Joanna Chorostowska-Wynimko spoke with EMJ, sharing insights from the 2024 European Respiratory Society (ERS) Congress, the evolving role of molecular diagnostics, AI in lung cancer care, and the importance of patient education. Chorostowska-Wynimko also discussed her remarkable journey into respiratory medicine and ERS leadership.
Joanna ChorostowskaWynimko
ERS Vice President and Head of the Department of Genetics and Clinical Immunology at the National Institute of Tuberculosis and Lung Diseases (NITLD), Warsaw, Poland
Your extensive career in respiratory medicine and genetics has brought you to many prestigious roles, including your current position as Vice President of the ERS. Can you share with us how your journey with the ERS began and what motivated you to take on a leadership role within the organisation?
As always, it's about dedication and enthusiasm. My journey with the ERS began many years ago. I attended my first congress in 1994, shortly after graduating from university. It was my first major international event, and I was absolutely impressed with the size, the people, and the expertise, and that has inspired me to follow the same pattern. After a few years, I was elected as a national ERS delegate for Poland, and that’s what started my very close interaction with the ERS, which wasn’t always easy but very stimulating for me as a clinician and as a scientist. The ERS provides an opportunity to truly enrich your professional career in a very positive way. It offers an international perspective through meeting people who serve as inspiring examples of
where you can aim to go, who to follow, and how to shape your professional goals.
ERS is an environment where you can visualise the direction you want your life to take. This is especially important now, as we discuss work-life balance more than ever. ERS allows you to see people who have reached various stages of professional and personal development, providing a point of comparison and inspiration.
Starting as a national delegate, I took on multiple roles and eventually became ERS Secretary General before becoming a candidate for the presidential election. I hope I proved myself to many, and now I am the ERS Vice President.
Q2 What sessions are you most looking forward to about this year’s ERS Congress?
Professionally, I am involved in the diagnostics of respiratory diseases, with a specific focus on molecular techniques and technologies that can be implemented in routine clinical work.
This is reflected in my interest in lung cancer, which I believe is a rapidly progressing field in terms of diagnostics, molecular diagnostics, and genetics. These aspects are now a standard part of the routine evaluation of patients and are crucial steps before making decisions regarding optimal therapy.
Nowadays, respiratory specialists play a key role in diagnosing both advanced and early-stage lung cancer, forming a crucial part of the multidisciplinary team, and taking responsibility for the treatment process. We have been involved with lung cancer primary prevention (smoking cessation programmes) for decades, and recently we have been working towards strengthening low-dose CT lung cancer screening projects in Europe.
Nowadays, respiratory specialists play a key role in diagnosing both advanced and early-stage lung cancer, forming a crucial part of the multidisciplinary team
Q3
So, there's a lot we as medical professionals with interest in respiratory field can do for potential patients and people in general. This is very well reflected in the ERS Congress programme this year. Number of sessions addresses the topics I have just mentioned. Modern therapies require modern diagnostics, as you’ve mentioned. What are the biggest challenges currently facing the implementation of molecular diagnostics in lung cancer?
Many challenges exist, but fundamentally, it's about organising the process. In recent times, diagnostics and treatments have become complex, involving many experts, starting from respiratory physicians, radiologists, molecular biologists, genetics, clinical oncologists, thoracic surgeons, radiotherapists, psychologists, and physiotherapists. Having all these specialists engaged in the patient journey is very important, and organising the process so that these professionals have the opportunity to communicate with each other is crucial.
Another key aspect is patient involvement. This is incredibly important because some decisions are life-changing for the patient. I firmly believe it's essential to have patients or a patient representative involved in the decision-making process.
From a technological standpoint, one key tool is next-generation sequencing (NGS), which provides vital data for the optimal management of lung cancer. A lot of clinically important data can be derived from NGS analysis. So, the question now is, how do we use this information for the patient's benefit?
Q4 Your work focuses on extending survival but also improving the quality of life for patients. What are some of the key elements in your practice that contribute to achieving both these goals simultaneously?
I believe it’s how we deliver healthcare. The process is complex and often lengthy, so making it more concise and efficient is vital for patients. The waiting period for a final diagnosis is particularly challenging, making it crucial to shorten this time.
At the same time, I strongly believe that providing psychological care should be a routine part of healthcare, not only at the moment when the diagnosis is presented to the patient but also throughout the waiting period for the diagnosis. This waiting time is often just as difficult for the person as the diagnosis itself, even if they aren't officially a patient diagnosed with cancer yet. So, I think time efficiency is incredibly important, not just for us as healthcare providers but even more so for the patient.
Q5 You’ve discussed the benefits of targeted therapies and immunotherapy on patients’ daily lives. How important do you think patient education and involvement are in the decision-making process for their treatment?
I believe patient education is important nowadays for essentially any respiratory disease. This is true for lung cancer, asthma, and COPD. I am a strong believer in patient education, not only because I feel that patients have the right to understand what’s going on and why a particular treatment has been chosen, but also because they have the right to be part of the decision-making process.
Feeling empowered and having the opportunity to speak their mind transforms the patients from subjects of treatment to active participants.
Feeling empowered and having the opportunity to speak their mind transforms the patients from subjects of treatment to active participants
I always do my best with my patients to explain where their symptoms come from and what we can do to alleviate them. For instance, explaining when and how to use an inhaler in specific situations. This approach is greatly appreciated by patients because it gives them a sense of partnership, and it's appreciated by me because I feel like I have a partner in their care.
Q6
Do you hope to emphasise this level of patient education and involvement in your role as Vice President of ERS?
I have been working with the ERS for many years, and I do believe that ERS is the organisation that provides high-quality information. While education for healthcare professionals is a cornerstone of our organisation, providing high-quality patient education is an equally important goal, and that’s where the ERS excels. And we work hand in hand with the European Lung Foundation (ELF), the key patient-led European organisation in our field.
Additionally, ELF and ERS are a part of the International
Respiratory Coalition, and one of the key goals of both the international and national coalitions is to support and build educational activities directed towards patients as well as the general public. I think it's important to inform the general public because the information is also a form of prevention. This approach has been a part of ERS policy for many years, so it's not new, it's about continuity and being consistently there for patients.
Q7
Artificial intelligence is a major theme of this year's congress, and it's increasingly being integrated into healthcare. How do you see AI transforming the field of respiratory medicine, particularly in areas like lung cancer diagnosis?
AI has already been transforming the field of lung cancer screening. For example, I don’t believe an efficient national lung cancer screening programme would be possible without AI involvement. There are AI tools that have been validated for clinical use, which support radiologists within national screening programmes in Europe. AI helps to make the process faster and more efficient, enhancing our day-to-day work in medicine.
AI is not only used in prevention but also in diagnostics and treatment. For example, in genetics and NGS, where broad molecular panels involve hundreds of genes, AI is crucial for analysing the vast amount of information generated. It helps us link genetic data to clinical information to better understand the clinical significance of specific gene alterations. Without AI, we would struggle to fully comprehend the complexity and potential clinical value of these findings.
Q8 As someone deeply involved in both clinical and scientific leadership, what do you think are the most pressing challenges for the respiratory community today, and how do you think the ERS can help to address those?
There are many pressing challenges, but in lung cancer specifically, the rising prevalence, particularly among women, is a key concern. This situation is almost like an epidemic, and we must make every effort to prevent it. A key factor is smoking, as unfortunately, about 30% of the European population are still smokers. Additionally, new forms of nicotine use, like vaping, are also a concern. Vaping is definitely not safe, and ERS has been emphasising this for years. Recently, we issued a new statement on this issue. It's crucial that this message reaches the general public, especially the younger generation, who are starting to smoke again.
AI has already been transforming the field of lung cancer screening. For example, I don’t believe an efficient national lung cancer screening programme would be possible without AI involvement.
Policymakers and politicians also play a critical role since they make decisions about budgets and regulations. Addressing these challenges requires action at multiple levels. In the context of lung cancer, it's a disease that carries a heavy burden, both
psychologically and economically. Therefore, our approach must include primary prevention, such as smoking cessation, secondary prevention, like lung cancer screening, and if cancer is suspected, ensuring the best possible care for the patient This includes providing access to advanced molecular diagnostics at a professional and comprehensive level, not just in Europe but globally.
Q9Finally, what are you most looking forward to in your new role as President-Elect of the ERS?
This is a challenging question because there are so many activities that I'm excited about. As the President-Elect, I represent over 34,000 members of the ERS. It's a significant responsibility that I truly feel, but it’s also a great honour. Being elected by your peers for
such a role makes you proud. I see my role in several ways: firstly, representation, and secondly, bringing the voice of respiratory experts to others, to the public, policymakers, and other medical specialties, such as cardiologists, radiologists, clinical oncologists, and many others. Collaboration with medical professionals is especially important because we share common interests, particularly in patient care.
I also believe strongly in primary and secondary prevention. Prevention is one of the most effective ways to improve health outcomes; it's better to prevent diseases than to treat them. This is something I want to particularly emphasise during my presidency.
Coming from Poland, which is in Central and Eastern Europe, I
am aware of the specific issues within this region. I hope to further engage my colleagues from this area within the ERS. They are already very active, but I see many opportunities, especially for young members, to be even more involved. ERS is a wonderful organisation that embraces not only clinicians but essentially anyone interested in respiratory medicine, at any stage of their professional career.
I'm particularly proud of our Early Career Members Assembly. It’s not just an opportunity for networking and shaping professional paths; it's also about having fun and making the journey enjoyable. I believe that enjoying your career is an important part of professional life, and that's something I hope to foster.
Interviews
EMJ had the pleasure to interview Patricia Silveyra and Antonio Anzueto, who shared insights into their respective fields of respiratory health. Silveyra explained how her childhood experiences with pollution and family health inspired her to focus on sex differences in lung diseases, placing an emphasis on interdisciplinary research and advocacy for underrepresented groups. Anzueto discussed advancements and treatments in chronic obstructive pulmonary disease, and how these have improved patient outcomes and quality of life. Both emphasise the importance of collaboration, mentorship, and persistence, encouraging the next generation of medical professionals to prioritise patient care.
Featuring: Patricia Silveyra and Antonio Anzueto
Patricia Silveyra
Associate Professor and Chair, Department of Environmental and Occupational Health, Indiana University, Bloomington, USA
What initially inspired you to begin working in respiratory health, specifically researching sex differences in lung disease?
The menstrual cycle phase affected many aspects of our health, including asthma exacerbations, allergic responses, headaches, and other conditions
I grew up in a big city with lots of visible air pollution, and a high prevalence of smoking and chronic obstructive pulmonary disease (COPD), so I was always interested in helping my community reduce the burden of these factors on their health. Also, my grandfather had asthma and was ‘treated’ by moving away from the city to a less polluted area with high altitude, which also made me curious (why would altitude help asthma?). While I initially didn’t study lung diseases (my PhD focused on molecular endocrinology), it was during my postdoc that I was introduced to the field of female health and sex differences, and found out that many lung diseases disproportionally affect adult
females, especially those that were caused or exacerbated by inhaled pollutants and toxicants. Thus, I decided to apply my knowledge of hormone-mediated mechanisms to understand the basis for these sex disparities in lung disease.
Q2
What has been the most surprising finding, in your opinion, in your research on sex differences in lung inflammatory responses to environmental factors?
I knew from personal experience and from talking with other females that the menstrual cycle phase affected many aspects of our health, including asthma exacerbations, allergic responses, headaches, and other conditions. However, these experiences were often dismissed or thought to be serendipitous. While working on a model of ozone-induced lung inflammation, my lab was able to
identify the connection between hormonal changes that occur in the menstrual cycle and the expression of genes associated with inflammatory responses, as well as immune cells infiltrated to the lungs. While I expected to find an association, I didn’t expect to find so many genes, cells, and mechanisms involved, nor to find a role of both male and female hormones in mediating these mechanisms.
Q3 Your research lab at Indiana University, Bloomington, USA, places particular emphasis on interdisciplinary approaches to research. How do you think this approach has benefitted your research projects?
The interdisciplinary aspect of my research has allowed me to think outside of the box and include new perspectives to understand health problems. Working with physicians, I get to learn about patient experiences and what doesn’t make it to the papers or charts. Working with epidemiologists, I get to integrate multiple variables, social and biological, to better understand the multiple factors that affect the diseases I study and to take the research direction that is more likely to satisfy the needs of the community. Working with nurses and community leaders,
I get to communicate my findings to a broader audience and increase the impact of my work.
Q4 In 2022, you were named the inaugural Anthony D. Pantaleoni Eminent Scholar, as well as Chairperson for the Department of Environmental and Occupational Health. How have these appointments, as well as your many other awards, opened doors for you in terms of your work and research?
I am honoured to have received these recognitions, and to have been chosen to lead the department. Leadership is about serving others, and I have always enjoyed supporting my colleagues and trainees. The awards have helped me establish a reputation in a competitive field, and allowed me to have a seat at the table where important decisions about science and medicine are made.
Q5 Can you tell our readers about some of the major projects you have been involved in as an advocate for females and other underrepresented groups in science, working with Society for Advancement of Chicanos and Native Americans in Science (SACNAS)?
The work I get to do in this area is both exciting and impactful. Serving in organisations like
SACNAS allows me to reach thousands of students around the country. The main activities involve mentored scientific presentations, exposure to role models, leadership training, and training in science communication. Most students who come to SACNAS have never had a professor or teacher of colour, nor met an accomplished scientist that looks like them. The exposure to these role models and the mentoring provided at the meeting impact their careers tremendously, allowing them to deal with feelings of imposter syndrome or stereotype threat, and giving them inspiration and motivation to become the best scientists they could be.
Q6 What do you think the next steps are for societies such as SACNAS when it comes to getting females and other minority groups involved in science and medicine?
Mentoring and sponsorship are crucial because they open doors and provide clear pathways to success. Exposure to role models, and inclusive practices that de-centre individuals and focus on the environment, are key to increase representation. Individuals from minoritised groups face challenges at every step of their career, by having disproportionate service burdens, lacking access to mentors,
Mentoring and sponsorship are crucial because they open doors and provide clear pathways to success
networks, and opportunities, and experiencing bias. It is important to address these challenges along the way, not just by recruiting more individuals into careers, but also providing the necessary tools for success and retention.
Q7
You work with the National Academies of Sciences, Engineering, and Medicine (NASEM) on their ‘New Voices’ initiative, aiming to bring diverse perspectives from earlycareer leaders to the field. Why do you think this initiative is so important in medicine today?
I often describe New Voices as the perfect combination of young experts in the most pressing disciplines that advance our society. These early- and midcareer leaders are those having high level discussions that will be impacting science, technology, and medicine in the coming decades. While all of us are leading and impacting our respective fields and communities, working together has created a synergistic effect that allows the creation of
recommendations, communications, and technologies to quickly address pressing challenges and disrupt exclusionary systems. It has also allowed the expansion of discussions to the international level, integrating important voices to pressing challenges such as the current climate crisis.
Q8 What changes do you hope to see in the near future as a result of your work with New Voices?
I hope to continue to expand my network of collaborators and give direction to the science I conduct in the lab, so that it has a broader reach to communities outside of the USA. I also hope to be able to communicate science in a more effective and inclusive way, using different available technologies and languages, so that I can help fight misinformation, serve as a role model for future generations, and ensure that all members of society benefit and learn from the discoveries that are made with their tax contributions.
Antonio Anzueto
University of Texas Health Science Center at San Antonio, Department of Medicine, Pulmonary/Critical Care, South Texas Veterans Health Care System, San Antonio, USA
Q1What has led you to pursue a career in pulmonary medicine, and what led you to specialise in chronic obstructive pulmonary disease (COPD)?
conditions that will lead to acute respiratory failure.
In 24 years of development, the biggest achievement was the development of effective bronchodilators
Before I decided to pursue a career in pulmonary medicine, I did internal medicine, and was really fascinated by dyspnoea (difficulty breathing). I found it interesting how some people would experience shortness of breath, which not only made them uncomfortable but also led to significant drops in their oxygen levels, in turn making them significantly ill. Eventually, this led me to multiple clinical interests. I started working with patients suffering from chronic bronchitis and COPD, as well as those with acute respiratory injuries. In the USA, the fields of pulmonary and critical care are often intertwined, which allowed me to treat acutely ill patients in the intensive care unit who also had underlying pulmonary diseases.
I realised that understanding the underlying diseases is crucial in treatment, for example, in COPD, when patients develop acute respiratory failure, it is triggered by events like pneumonia. My goal was to understand what exacerbates these conditions and how we could prevent some of those conditions that lead to multiorgan failure, sepsis etc. I have been focused on what seems like different areas of pulmonary medicine, like pneumonia, respiratory failure, and COPD, but all have a lot in common. At the end of the day, it will be the interactions between the patient and multiple
My interest in COPD specifically grew over the years, in part because, back in the late 1980s and early 1990s, we had very little understanding of the disease and no effective treatments. It was an underdefined condition, which made it both challenging and fascinating. When I began to see patients, we had no treatments, no understanding, and no definition of the disease. Over the past 24 years, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) has provided a framework that revolutionised our approach to COPD. Since its first publication in 2001, a tremendous amount of research has been conducted, leading to effective therapies that can slow the progression of COPD and even decrease mortality.
Q2Since starting your career, what do you think has been the most significant change in COPD management and treatment?
I think it’s three-fold. One is that we now have a better understanding from the epidemiological point of view. Initially, we had observational cohorts that were limited and not well established, and now we have long-term cohorts of individuals. We also now recognise that different conditions can precipitate disease. For example, we studied at length the use of tobacco, and its impact on the disease, and recognised it as an important cause of COPD; but
in the world biomass exposure, there are also pulmonary infections like tuberculosis and some genetic conditions that are ultimately responsible for patients developing the disease. It’s about putting all those pieces together to understand what precipitates a condition. Furthermore, we now know that pharmacotherapy, especially bronchodilators, has a significant impact on the disease, and we are more focused on the prevention of acute events like as exacerbations, hospitalisations, and mortality. Putting all of this together, we now understand that COPD is not limited to the lungs and that the patients who have COPD also have cardiovascular conditions, so we need to further enhance our understanding of these interactions and how the management of one impacts the other and vice versa.
allows us to have available not one but three fixed triple therapy formulations for managing COPD. Putting all of this together, we can now see that having triple therapy is having a significant impact on improving lung function, but also improving quality of life, decreasing exacerbation, and probably impacting mortality.
to medications. These studies show that starting triple therapy during hospitalisation can prevent readmissions.
The evolution of COPD treatment is not just about developing pharmacotherapy but also about its implementation and timing. This holistic approach is crucial for improving patient outcomes.
COPD is not limited to the lungs and that the patients who have COPD also have cardiovascular conditions
Q3In a recent interview, you discussed the importance of triple therapy in managing COPD. So, could you elaborate on how this treatment has evolved and what impact it’s had on re-hospitalisations and improving patient outcomes?
In 24 years of development, the biggest achievement was the development of effective bronchodilators. We’re very excited that in these years the end-product is to have long-active bronchodilators with inhaled steroids delivery in a single device. This is the culmination of a huge amount of research that
I really want to emphasise that COPD is a treatable and possibly reversible condition, and what’s most important for my patients is that they feel better. My patients often tell me they want to feel better rather than just hearing about improved lung function. Triple therapy has not only improved lung function but also significantly enhanced patients' quality of life, exercise capacity, social interactions, and sleep. It has also reduced exacerbations more effectively than monotherapies, potentially decreasing all-cause mortality in patients with COPD.
Reflecting on the objectives set in the first GOLD document in 2001, we have achieved improved lung function, prevention of exacerbations, and increased survival rates. However, our work isn't finished. One of the big questions now is when to start this therapy. Recent realworld evidence suggests that initiating triple therapy during hospitalisation for exacerbations, rather than waiting, provides better outcomes.
Over the past few years, many healthcare systems have faced challenges when patients are readmitted within 30 days after a COPD exacerbation, often resulting in financial penalties. To address this, we've implemented mechanisms like nurse managers and patient education to ensure adherence
Q4
The American Thoracic Society (ATS) has been a significant part of your professional journey. Can you tell us about your experience with ATS and what initiatives you’ve been involved with since you joined?
I have been attending ATS meetings for the past 35 years in person, with the only exception being during the 2020 pandemic, when I attended online. This annual meeting is a unique opportunity to interact with people involved in many areas of pulmonary medicine .For example, in regards to advancing my clinical research, the ATS conference allows me to interact with top world scientists, ask questions, and discuss ideas to further improve my research. Over the years, I’ve significantly contributed to the research society by serving as chair of the programme committee for critical care and clinical problems sections. I’ve also been a member of the minority committee and the financial committee.
The big and fascinating thing about ATS meetings is the exchange of ideas among the diverse group of pulmonary and critical care providers from around the world. The meetings, which now attract over 15,000 attendees, provide an invaluable opportunity for this global community to come together and share their knowledge.
A notable initiative that I was involved with at ATS was the development of an interest group to encourage participation from Latin American association members. This initiative allowed more Latin American association members to converse and present their work at this international meeting. Additionally, I’ve been involved with other interest groups, such as the Veterans Administration in the USA, which is a unique healthcare system with thousands of pulmonary providers.
These meetings facilitate face-to-face interactions and exchange of ideas that simply can’t be replicated through email or virtual meetings. The secret to the success of these meetings, whether it’s the ATS, the European Respiratory Society (ERS), or other national and local organisations, lies in the opportunity they provide for academic and idea exchange. These interactions lead to new
ways to help our patients and advance our field.
Q5
Can you share with us some of the major challenges currently facing the field of pulmonary medicine, and what advancements do you foresee in the next decade?
The challenge that I see in pulmonary medicine is the increasing specialisation within the field. We’ve developed highly effective interventions and pharmacotherapies for specific conditions such as COPD, asthma, interstitial lung disease, and pulmonary fibrosis. This specialisation means that general pulmonologists often need to refer patients to specialists for conditions like pulmonary hypertension.
As a result, it’s becoming almost impossible for general pulmonologists to manage all these specialities effectively. However, this trend ultimately benefits patients. If I were a
patient with a specific condition, I’d want to see a specialist who focuses on managing that condition.
The primary role of a general pulmonologist, therefore, is to identify these conditions early, make appropriate referrals, and continue caring for patients with more common pulmonary issues. Looking ahead, I see this as a significant challenge over the next decade.
We’re also witnessing remarkable advancements in treating cystic fibrosis, leading to much better outcomes for patients. In COPD, the development of biologics in the next 2–3 years is expected to bring about significant structural changes. The same advancements are happening in interstitial lung disease and pulmonary infections, where we now have better diagnostic tools. The explosion in technology translates into improved patient care and more applications in patient care.
Q6 Are you currently working on anything exciting that you can share with us?
In the area of COPD, a very exciting development of new molecules. I’ve been involved with a medication called ensifentrine, which inhibits phosphodiesterase 3 and 4 in a completely different pathway than what we’re using today. This medication is an anti-inflammatory and a bronchodilator. Currently, it’s administered via nebulisation, but I can foresee it being developed in other forms, like powder. With this single molecule, we can achieve a lot more than what we’ve been able to do with other medications, which often need to be combined.
Another fascinating development is the role of biologics. Biologics have revolutionised the treatment of asthma, with six or seven medications available today. This revolution is now translating into chronic lung diseases like COPD.
We’re beginning to see the approval of biologics for individuals with higher eosinophil counts, and in the next few years, we’ll see this approach extend to a broader range of patients with more severe diseases. The ultimate objective is to halt the progression of COPD.
Biologics
have revolutionised the treatment of asthma, with six or seven medications available today
Q7 Lastly, what advice would you give to medical students or young professionals who aspire to pursue a career in respiratory medicine?
My first piece of advice is to understand that ‘there is more time than you think’. There’s no need to rush or try to accomplish everything in the next year. Take your time and focus on what you like
and gradually you can reach your goals.
My second piece of advice is to be persistent. You’re going to face many rejections, whether its articles being turned down by journals or other setbacks. Keep pushing forward and believe in what you’re doing. Persistence is key.
Always remember that the ultimate beneficiaries of our work are our patients and their families. Everything we do should focus on how we can improve their lives and make their day-to-day experiences better. We should always strive to go the extra mile and to help them in the best way possible.
And finally, remember to have fun. Enjoy the journey, even though it can be really frustrating at times. Keeping a positive outlook and finding joy in what you do will help you navigate the challenges along the way.
Don’t Hold Your Breath: Adapt and Become
More Resilient Against Air Pollution
Respiratory health effects of air pollution1,4
There is broad consensus amongst experts on the impact of air pollution and climate change on health.1,2 Even healthy individuals are impacted.1-3
• Increased risk of COPD, bronchitis, and asthma exacerbation
• Airway remodelling, oxidative stress, and inflammation
• Increased susceptibility to respiratory infections
• Reduced lung function
• Increased rates of pulmonary mortality
• Lung cancer
Strategy #1: Encourage behaviours in day-to-day life that promote resilience to air pollution
To mitigate negative effects of air pollution, it is important to promote health-modifying behaviours and manage pre-existing cardiorespiratory conditions3,7,8
Avoiding indoor tobacco smoking prevents multiple pollutants at home.7
Adaptations at home
Indoor plants can reduce air pollutants, ozone, and indoor air VOC pollution.8,9
Air purifiers cause a dramatic reduction in indoor particulate matter numbers.10
Using gaseous fuels at home instead of biomass reduces the risk of respiratory issues and pregnancy complications.11
What if electricity, which is considered a clean fuel, and gaseous fuels are not available?4,11
• Cross-ventilation (opening windows and doors) in cooking areas can be beneficial, although this must be balanced with consideration of outdoor dust levels as noted by symposium attendees
• Switching to more efficient cookstoves can be beneficial if possible.
What about when outdoors?
Maximum filtration efficiency for <300 nm and >300 nm sized particles for different mask materials at a flow rate of 1.2 CFM12
<300 nm ± error >300 nm ± error
Climate change impacts levels of such as CO2 levels and pollen counts
Strategy #2: Adapt diet and exercise against the harmful impact of air cardiorespiratory mortality with peak pollen concentrations.
Higher banana, apple, and tomato intake can slow age-related lung function decline.13
Pro-, pre-, and synbiotics may be capable of reversing the effects of air pollution via the gut–lung axis.14
While the benefits of exercise are well-known, negative effects of air pollution. Benefits of areas with high air pollution.3
Those with cardiovascular or respiratory disease events in polluted areas compared to when
Lung capacity when exercising is impacted by the benefits of walking exercise, highly polluted Odds ratio (log scale)
Experts attending the symposium highlighted that:
• If one has access to an electric car with a particulate matter meter, it allows monitoring of when to close the windows.
• Patients appear receptive to information on reducing costs of methods to support resilience, such as prescription air filters.
Key takeaways and considerations when communicating mitigation strategies
Key strategies that can be recommended:
Symposium attendees recommended work, instead of using high-exposure the benefits of exercise with the
• Behaviour, both indoors and outdoors, can be adapted to reduce risk of
• Adapting exercise pattern and diet can ameliorate negative
and reduce
concerns.
• Using anti-inflammatories and increasing intake of antioxidants can promote resilience.
This infographic was created by the Advisory Board members of The Clean Breathing Institute and funded by Haleon Content is based on a symposium delivered at ERS 2024 that was sponsored by Haleon
mortality on days concentrations.6 of air pollutants counts5
When symposium attendees were asked if they advise patients on the role of air pollution and climate change on respiratory ailments, ~55% either did not or found it not applicable to their role.
exercise to promote protective effects air pollution on both the heart and lungs
The Mediterranean diet can lower the risk of impaired lung function in adult smokers.15 the 14
Omega-3 may lower airway inflammation, but omega-6 may raise it.16,17
well-known, adaptations can be made to mitigate the exercise can be curtailed when performed in
disease can experience more respiratory in areas with lower air pollution*3
Mean estimates with p<0.05
Mean estimates with p<0.1 by air pollution.*†3 To maximise polluted areas should be avoided.3
*All study participants were at least 60 years old. In data from the United Kingdom shown, where applicable, Oxford street is indicated as a polluted area and Hyde Park is indicated as an area with clean air.3
Healthcare professionals should provide clear, evidence-based guidance to support adaptation at the individual level to ensure resiliency against increasing air pollution.
Strategy #3: Build resilience through use of antioxidants and anti-inflammatory treatments
Dietary antioxidants could alleviate oxidative stress and inflammation caused by reactive oxygen species seen in pollutioninduced airway inflammation.18
Nasal saline irrigation can reduce pollutant contact time on the respiratory mucosa in both adults and children and can have anti-inflammatory effects.21
Key antioxidant sources:18-20
Nasal anti-inflammatory steroid sprays may increase resistance of nasal mucosa against the negative effects of air pollution.22
People with rhinitis living in highly polluted areas may benefit particularly.22,23
When symposium attendees were asked if they advise their patients with allergic rhinitis to use nasal steroids to minimise effects of air pollution, 86% did not or found it not applicable to their role
Choice of answers:
A) Yes, for all my patients
B) Yes, for some of my patients
C) I don’t offer this advice to any of my patients
D) Not applicable to my professional role
Inhaled corticosteroids:24
• May decrease susceptibility to particulate matter in people with asthma.
• May increase vulnerability to nitrogen oxide and carbon monoxide.
Recommending combination regimens may be beneficial but require further study to confirm impact.25
Hours after start
walk
†Significance values are indicated as follows: *p<0·05, **p<0·01, ***p<0·001, comparing Oxford Street with Hyde Park. +p<0·05, ++p<0·01, +++p<0·001, compared with timepoint 0
recommended exercising in local parks and cycling to high-exposure public transport routes, to help balance the negative effects of air pollution.
concerns. air pollution. resilience.
Continued research will help refine guidelines and ensure recommendations are based on solid evidence.
1. Grigorieva E et al. Atmosphere. 2021;12:790. 2. Seastedt H et al. Ann Allergy Asthma Immunol. 2023;131(6):694-702. 3. Sinharay R et al. Lancet. 2018;391(10118):339-49. 4. Carlsten C et al. Eur Respir J. 2020;55(6):1902056. 5. Zhang Y et al. Nat Commun. 2022;13:1234. 6. Brunekreef B et al. Lancet. 2000;355(9214):1517–18(2). 7. Ni Y et al. Environ Res. 2020;181:108910. 8. Papinchak HL et al. HortTechnology. 2009;19(2);286-90. 9. Wood RA et al. Water, Air and Soil Pollution. 2006;175:163-80. 10. Vyas S et al. PLoS One. 2016;11(12):e0167999. 11. Puzzolo E et al. Lancet Resp Med. 2024;12(4):281-93. 12. Konda A et al. ACS Nano. 2020;14(5):6339-47. 13. Garcia-Larsen V et al. Eur Respir J. 2017;50(6):1602286 14. Keulers L et al. Environ Pollut. 2022;302:119066. 15. Catalin RE et al. Nutrients. 2023;15(5):1272. 16. Rutting S et al. Am J Physiol Lung Cell Mol Physiol. 2018;314(6):L922-35. 17. Kumar A et al. Nutr Res Rev. 2016;29:1-16. 18. Péter S et al. Nutrients. 2015;7(12):10398-416. 19. Hosseini B et al. Am J Clin Nutr. 2018;108:136-55. 20. Ezerina D et al. Cell Chem Biol. 2018;25(4):447-59.e4. 21. Head K et al. Cochrane Database Syst Rev. 2018 (6);6:CD012597. 22. Zhang Y et al. Allergy Asthma Clin Immunol. 2022;18:56. 23. Greiner AN et al. Lancet. 2011;378(9809):2112-22. 24. Staggers K et al. Am J Respir Crit Care Med. 2024;Online ahead of print. 25. Shikani AH et al. Ear Nose Throat J. 2014;93(4-5):E48-54.
Chronic obstructive pulmonary disease (COPD) is characterised by long-term persistent respiratory symptoms and airflow limitations. It is often due to long-term exposure to irritants like tobacco smoke, but may also be caused by genetic predispositions, in utero exposures or early life events. With smoking being the leading risk factor.1-2
Two main types of COPD:
Chronic bronchitis
COPD is currently diagnosed through spirometry. Additional diagnostic tools include chest X-rays or CT scans to visualise lung damage, arterial blood gas analysis, and genetic testing for alpha-1 antitrypsin deficiency.1
Healthy bronchus
Emphysema
Healthy alveoli
New Therapies in COPD
Inflamed bronchus
Inflamed alveoli
Biologics
Types of biologics
Anti-IL-5 Agents: reduce eosinophil counts by inhibiting IL-5, reducing inflammation and exacerbation rates in patients with eosinophilic COPD.6
COPD affects approximately 3.23 million deaths and is the third leading cause of death, with
384 million people
Biologics are a new class of drugs derived from living organisms that target specific immune pathways involved in the disease processes, offering a precise treatment option for COPD.5
Anti-IL-4/13 Agents: modulate IL-4 and IL-13 pathways, benefiting patients with mixed inflammatory profiles.6
Treatments and Emerging Breakthroughs
Management of COPD
Current management options for COPD focus on symptom alleviation, improving quality of life, preventing exacerbations, and slowing disease progression.
Smoking cessation
Smoking cessation is a primary intervention in COPD management, as it is the only measure proven to significantly slow disease progression and improve survival rates. It mitigates the accelerated decline in FEV1 and reduces inflammation, leading to fewer exacerbations and hospitalisations. Evidence-based approaches include behavioral counseling, pharmacotherapies like nicotine replacement therapy and comprehensive support programs tailored to individual patient needs.1 people worldwide deaths each year with around
Bronchodialators
Bronchodialators, including beta-2 agonists and anticholinergics, reduce airway resistance by relaxing airway smooth muscle through increased cyclic adenosine monophosphate or inhibition of muscarinic receptors, improving flow rates.3
Inhaled corticosteroids (ICS)
ICS reduce airway inflammation by binding to glucocorticoid receptors, repressing proinflammatory gene expression, and decreasing cytokine and chemokine production, thus reducing exacerbation frequency in patients with eosinophilic inflammation.4
Long-term oxygen therapy
Long term oxygen therapy for patients with chronic resting hypoxemia (≥15 hours/day) improves oxygen delivery to tissues and may have a survival benefit.1
Pulmonary rehabilitation
Pulmonary rehabilitation combines tailored exercise programs, education, and psychological support to help patients improve their lung function, build physical endurance, and manage symptoms more effectively. By enhancing patients’ ability to perform daily activities and reducing the frequency and severity of exacerbations, pulmonary rehabilitation improves overall quality of life and long-term outcomes for individuals with COPD.1
Challenges
Most challenges with current treatment options arise from continued disease progression, efficacy, and side effects. ICS are often associated with increased pneumonia risk and tolerance issues, while oxygen therapy can exacerbate hypercapnia in some patients.1
Ongoing clinical trials
Biologics targeting Il-4 and IL-13 cytokines block the receptors of IL-4 and IL-13, preventing the cytokines from binding and triggering inflammatory pathways. Reducing airway inflammation, mucus production, and immune response in patients with T2 inflammation. Phase III clinical trials have shown reductions in exacerbation rates, reduced lung function, and reduced need for steroids.
IL-5 targeting biologics block IL-5 or its receptor, reducing eosinophil counts in the blood and lung tissue, thereby lowering eosinophilic inflammation. Phase III clinical trials (METREX and METREO) showed 18–20% reduction in exacerbation rates in patients with high eosinophil counts.6
Precision Strikes: Personalising Potentially Surgically Resectable Stage IIIA Lung Cancer Treatment with Targeted and Immune Therapies
Authors: *Luca Bertolaccini,1 Monica Casiraghi,1,2 Antonio Mazzella,1 Claudia Bardoni,1 Giovanni Caffarena,1 Matteo Chiari,1 Filippo de Marinis,3 Lorenzo Spaggiari1,2
1. Department of Thoracic Surgery, European Institute of Oncology IRCCS, Milan, Italy
2. Department of Oncology and Hemato-Oncology, University of Milan, Milan, Italy
3. Division of Thoracic Oncology, European Institute of Oncology IRCCS, Milan, Italy
*Correspondence to luca.bertolaccini@gmail.com
Disclosure: The authors have declared no conflicts of interest.
Acknowledgements This work was partially supported by the Italian Ministry of Health with Ricerca Corrente and 5x1000 funds.
The treatment landscape for potentially surgically resectable Stage IIIA non-small cell lung cancer (NSCLC), particularly for adenocarcinoma and squamous carcinoma, has evolved significantly in recent years. Up to now, in patients diagnosed with Stage IIIA NSCLC, the standard approach typically began with neoadjuvant therapies followed by surgical resection, which is considered the cornerstone of treatment. In recent years, in the case of adenocarcinoma and squamous carcinoma, the treatment strategy may vary based on specific molecular characteristics. For instance, epidermal growth factor receptor (EGFR) mutations or anaplastic lymphoma kinase
(ALK) rearrangements may benefit from targeted therapies in adjuvant settings. For potentially surgically resectable Stage IIIA disease, neoadjuvant chemotherapy combined with immunotherapy is being explored to enhance surgical outcomes and improve long-term survival rates.1 Overall, integrating novel immunotherapies and targeted agents into the treatment paradigm is promising, with ongoing clinical trials to optimise outcomes for patients with both adenocarcinoma and squamous carcinoma subtypes. This evolving landscape emphasises the importance of personalised treatment strategies based on tumour biology and patient characteristics, ensuring that the most effective therapies are utilised to improve survival and quality of life.1
MULTIFACETED APPROACH TO POTENTIALLY RESECTABLE STAGE IIIA LUNG CANCER
If Stage IIIA NSCLC is classified as potentially resectable, this categorisation is crucial as it influences subsequent treatment decisions, including neoadjuvant or adjuvant therapies (Figure 1). In histological subtypes, adenocarcinoma and squamous carcinoma can exhibit different biological behaviours and responses to treatment, which are essential for tailoring therapy.2
The presence of EGFR and ALK can significantly influence treatment decisions and outcomes. For EGFR-positive tumours, targeted therapies such as EGFR tyrosine kinase inhibitors, like osimertinib, can be highly effective, as they specifically inhibit the activity of the mutated receptor, leading to improved response rates and survival outcomes.3 Similarly, ALK-positive tumours are candidates for ALK inhibitors, such as crizotinib or alectinib, which target specific genetic alteration and have shown significant efficacy.4
Figure 1: Overview of the treatment landscape for surgically potentially resectable Stage IIIA NSCLC.
Programmed death-ligand 1 (PD-L1) expression levels play a crucial role in treating lung cancer, particularly in determining eligibility for immunotherapy. PD-L1 is a protein that can be expressed on the surface of cancer cells, and its levels are categorised into three distinct groups:
• Less than 1% indicates a lower likelihood of response to PD-1/PD-L1 inhibitors, and patients in this category may not be considered suitable candidates for immunotherapy.
• Between 1% and 49% suggest a potential benefit from immunotherapy, but the response can be variable. Patients in this group may be considered for treatment based on additional clinical factors and the specific immunotherapy used.
• Greater than 50% of PD-L1 expression is generally associated with a more favourable response to immune checkpoint inhibitors.5,6
In potentially surgically resectable Stage IIIA, treatment sequencing is critical. Upfront surgery followed by adjuvant biological treatment involves surgery to remove the tumour as the first step. The goal of upfront surgery is to achieve complete resection of the cancer. Following surgery, patients may receive adjuvant biological treatments, such as immunotherapy or targeted therapy, to address residual disease. This strategy aims to reduce the risk of recurrence by targeting microscopic diseases that could lead to relapse.7 For instance, high PD-L1 expression or specific genetic mutations may benefit from adjuvant therapies that enhance the immune response or inhibit tumour growth. In cases where the tumour is not immediately resectable due to size, location, or involvement of surrounding structures, neoadjuvant chemotherapy aims to shrink the tumour, making it more amenable to surgical resection. Using neoadjuvant chemotherapy can also help assess the tumour’s response to treatment, which can inform postoperative management decisions.6 After surgery, patients may still receive adjuvant therapies to reduce the risk of recurrence further.
Both approaches are designed to optimise outcomes by ensuring that the most effective treatments are administered at the appropriate times, based on the individual disease characteristics and overall health status. The choice between these strategies depends on various factors, including tumour resectability, preferences, and the presence of specific biomarkers.7
For patients undergoing neoadjuvant chemo-immunotherapy, the standard regimen often includes a combination of chemotherapy and atezolizumab, an immune checkpoint inhibitor that explicitly targets PD-L1. This approach typically consists of administering four cycles of chemotherapy, followed by atezolizumab for up to 12 months. The chemotherapy component aims to reduce the size of the tumour, increasing the likelihood of achieving a complete resection crucial for long-term survival.1 Immunotherapy enhances the immune response against cancer cells. Targeting PD-L1 helps reinvigorate T cells that the tumour microenvironment may inhibit. This immune activation can lead to a more robust response against residual cancer cells that may remain after surgery.5
The combination of neoadjuvant chemoimmunotherapy aims to facilitate surgical resection and address potential micrometastatic disease that may not be detectable at the time of surgery. In addition to atezolizumab, the treatment landscape includes alternative induction therapies. Nivolumab can be administered with chemotherapy for three cycles and targets PD-1, another checkpoint protein that inhibits T cell activation.8 Similar to nivolumab, pembrolizumab can be combined with chemotherapy for four cycles. Pembrolizumab also targets PD-1 and has shown significant efficacy in improving outcomes in high PD-L1 expression. Notably, pembrolizumab is versatile as it can be utilised not only in the neoadjuvant setting but also in the adjuvant setting after surgery. This flexibility allows for tailored treatment planning based on the individual response to therapy and specific tumour characteristics, such as PD-L1 expression levels.6
FUTURE DIRECTIONS AND RESEARCH GAPS
Despite significant advances in potentially resectable Stage IIIA NSCLC treatment, several critical areas warrant further investigation to enhance patient outcomes and treatment efficacy. Current biomarkers, such as PD-L1 expression and genetic mutations, provide valuable insights but must be fully comprehensive in predicting treatment response and outcomes. Future research should focus on identifying and validating additional biomarkers better to predict patient responses to neoadjuvant and adjuvant therapies. Integrating multiomics approaches, including genomic, transcriptomic, and proteomic data, could lead to more accurate and individualised treatment strategies. While targeted therapies and immunotherapies have revolutionised the treatment landscape, resistance to these therapies remains a significant challenge. Investigating new targeted agents that address emerging resistance mechanisms is crucial.
Additionally, exploring combination therapies that synergistically enhance the efficacy of existing treatments could lead to improved outcomes. Clinical trials should evaluate novel drug combinations and assess their potential to overcome resistance and extend survival benefits. Sequencing neoadjuvant chemotherapy, immunotherapy, and surgical resection requires further optimisation. Research should focus on determining the most effective sequence and duration of therapies to maximise tumour response and minimise adverse effects. Understanding the interaction between different treatment modalities and their impact on long-term outcomes will be essential for refining treatment protocols. Personalised medicine, guided by comprehensive genomic and molecular profiling, holds promise for tailoring treatments to individual patients. Future studies should investigate how personalised treatment plans can be integrated into clinical practice based on a patient’s unique tumour biology and genetic profile. Developing tools to predict patient-specific responses and outcomes will enhance the precision of treatment
strategies. Despite advances in treatment, recurrence remains a significant concern in Stage IIIA NSCLC. Research into the mechanisms driving recurrence and metastasis is needed to develop strategies for preventing and managing relapse. This includes studying the role of residual disease and micrometastatic cells that may evade current therapies.9
DISCUSSION
A comprehensive approach for oncologists and surgeons treating potentially surgically resectable Stage IIIA lung cancer should encompass a multifaceted methodology that emphasises personalised treatment strategies based on each patient’s tumour’s unique genetic and molecular profiles.
A growing body of clinical trial data has reshaped the treatment landscape for Stage IIIA NSCLC, particularly concerning integrating immunotherapies and targeted treatments into neoadjuvant and adjuvant settings. For instance, the CheckMate-816 trial provided compelling evidence that neoadjuvant chemo-immunotherapy with nivolumab significantly improved pathological complete response rates compared to chemotherapy alone.8 This trial demonstrated that adding nivolumab resulted in higher rates of tumour downstaging, facilitating surgical resection and improving outcomes for patients with resectable Stage IIIA disease. These findings have begun to influence treatment guidelines, supporting the use of neoadjuvant immunotherapy combined with chemotherapy in clinical practice. In the context of adjuvant therapies, the ADAURA trial revolutionised the treatment approach for patients with resected EGFRmutated NSCLC. This trial demonstrated that osimertinib, an EGFR tyrosine kinase inhibitor, significantly improved diseasefree survival in patients with Stage IB-IIIA NSCLC undergoing complete surgical resection. Based on these results, adjuvant osimertinib has become a standard treatment for patients with EGFR-positive tumours, representing a significant advancement in personalised medicine for this subset of patients.3
Additionally, the IMpower010 study provided important insights into the role of atezolizumab in the adjuvant setting for patients with high PD-L1 expression. The trial showed that adjuvant atezolizumab significantly prolonged disease-free survival in patients with resected Stage II–IIIA NSCLC who had completed neoadjuvant chemotherapy, particularly in those with PD-L1 expression ≥50%. This has led to the incorporation of atezolizumab into treatment guidelines for patients with high PD-L1 expression, marking a critical development in managing Stage IIIA NSCLC.5
Understanding Stage IIIA NSCLC is crucial, as it is characterised by a tumour that may have spread to nearby lymph nodes but is still considered resectable. Genetic and molecular profiling plays a significant
role in tailoring treatment. Comprehensive genomic profiling should be conducted to identify mutations and PD-L1 expression levels. The results of biomarker testing should be used to customise treatment strategies, ensuring that therapies align with the specific characteristics of the tumour (Table 1). Treatment sequencing is another critical aspect. For patients who are not immediately resectable, neoadjuvant chemotherapy combined with immunotherapy should be considered.
After neoadjuvant therapy, the tumour’s resectability should be assessed, and surgical resection should be performed as soon as feasible to maximise the chances of complete tumour removal. Post-surgery, adjuvant therapies should be considered to target residual disease and reduce the risk of recurrence (Table 2).
1: Molecular targets and corresponding therapies in potentially surgically resectable Stage IIIA NSCLC.
EGFR EGFR mutations Osimertinib Improves disease-free survival in resectable cases
ALK ALK rearrangements Crizotinib, alectinib Significant efficacy in ALKpositive tumours
A multidisciplinary collaboration is essential in managing Stage IIIA lung cancer. Engaging a team that includes medical oncologists, surgical oncologists, radiation oncologists, pathologists, and genetic counsellors is crucial for developing and implementing a comprehensive treatment plan. Discussing various therapies’ potential benefits and risks ensures patients understand their options. A robust follow-up plan should be implemented to monitor for recurrence and manage any treatment-related side effects, which may include imaging studies and clinical evaluations at regular intervals. Supportive care services, including symptom management, nutritional support, and psychosocial counselling, enhance the patient’s quality of life throughout treatment. Continuous education is necessary to keep abreast of the latest research findings and treatment guidelines, ensuring the application of evidence-based practices in patient care.10
A comprehensive approach to managing potentially resectable Stage IIIA lung cancer should encompass not only the clinical and molecular aspects but also the patient’s perspective and quality of life considerations. Understanding Stage IIIA NSCLC requires attention to how treatment impacts patients beyond the clinical outcomes, including their daily lives, psychological wellbeing, and overall quality of life. Incorporating patient-reported outcomes into treatment planning is crucial. Various treatment strategies, including neoadjuvant chemotherapy and targeted therapies, can significantly affect patients’ experiences. For instance, side effects such as fatigue, nausea, and the psychological burden of prolonged treatment can impact patients’ quality of life. Addressing these factors in treatment decisions ensures that therapies are aligned with patients’ preferences and wellbeing.
References
1. Ferrari V, Helissey C. Revolutionizing localized lung cancer treatment: neoadjuvant chemotherapy plus immunotherapy for all?. J Clin Med. 2024;13(9):2715.
Furthermore, engaging patients in discussions about their treatment options can help tailor approaches that aim for clinical efficacy and consider patients’ values and goals. A robust follow-up plan should include regular evaluations of patient-reported outcomes to monitor and manage treatment-related side effects effectively. Supportive care services, including symptom management, nutritional support, and psychosocial counselling, enhance patients’ quality of life throughout the treatment process. By integrating these considerations, we can provide a more holistic view of the treatment paradigm, ensuring that therapeutic decisions align with clinical efficacy and patient-centred care.11
CONCLUSIONS
The management of potentially resectable Stage IIIA NSCLC has become increasingly sophisticated, driven by advances in surgical techniques and the integration of targeted therapies and immunotherapies. The standard approach of surgical resection remains pivotal, but the role of adjuvant and neoadjuvant treatments is expanding, particularly for patients with specific molecular characteristics. For instance, targeted therapies and the incorporation of immunotherapies are reshaping the treatment paradigm, offering new hope for improved survival and disease-free outcomes.
The importance of personalised medicine, guided by genetic and molecular profiling, cannot be overstated, as it allows for tailored treatment strategies that optimise therapeutic efficacy while minimising unnecessary exposure to less effective treatments. Multidisciplinary collaboration and continued participation in clinical trials will be essential in refining these strategies.
2. Bertolaccini L et al. The interdisciplinary management of lung cancer in the european community. J Clin Med. 2022;11(15):4326.
4. Wu YL et al. Alectinib in resected ALKpositive non-small-cell lung cancer. N Engl J Med. 2024;390(14):1265-76.
3. Tsuboi M et al. Overall survival with osimertinib in resected EGFRmutated NSCLC. N Engl J Med. 2023;389(2):137-47.
5. Felip E et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-smallcell lung cancer (IMpower010): a randomised, multicentre,
6. Wakelee H et al. Perioperative pembrolizumab for early-stage nonsmall-cell lung cancer. N Engl J Med. 2023;389(6):491-503.
7. Bertolaccini L et al. Long-term clinical outcomes and prognostic factors of upfront surgery as a first-line therapy in biopsy-proven clinical N2 non-
small cell lung cancer. Front Oncol. 2022;12:933278.
8. Forde PM et al. Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer. N Engl J Med. 2022;386(21):1973-85.
9. Horgan D et al. Bridging the divide: addressing discrepancies between clinical guidelines, policy guidelines, and biomarker utilization. Diagnosis (Berl). 2024;DOI:10.1515/dx-20240092.
10. Bertolaccini L et al. Revamping nonsmall cell lung cancer treatments in stages ii and iii: preparing healthcare for cutting-edge immunooncology regimens. Cancers (Basel). 2024;16(16):2842.
11. Bertolaccini L et al. Comment on the unbearable lightness of difference between statistical and clinical significance. Ann Surg Open. 2022;3(1):e114.
Advancing Respiratory Care: The Role of Simulation in Clinical Education
Author: J. Brady Scott1
1. Department of Cardiopulmonary Sciences, Division of Respiratory Care, College of Health Sciences, Rush University, Chicago, Illinois, USA
*Correspondence to jonathan_b_scott@rush.edu
Disclosure: Scott received research funding from the American Association for Respiratory Care (AARC); and was a content contributor for Relias Media.
Acknowledgements OpenAI (2023). ChatGPT with GPT-4 architecture was used to generate some draft language to improve readability. The author revised the language suggestions to his liking and takes responsibility for the content of this publication.
Received: 18.09.24
Accepted: 26.09.24
Keywords: Education, health care simulation, medical education respiratory care, simulation, simulation training.
The demand for highly skilled respiratory clinicians grows as respiratory care becomes increasingly complex with rapid advancements in medical technology and treatments. Respiratory care providers, such as respiratory therapists (RT), must possess various clinical skills, from patient assessment to managing mechanical ventilation. Simulation-based education has become a vital tool for preparing RTs by offering a controlled environment where learners can practice technical skills, enhance critical thinking, and improve patient interactions. The purpose of this article is to examine the role of simulation-based learning in respiratory care education, highlight its benefits and challenges, and explore its potential as the future of respiratory care training.
THE ROLE OF SIMULATION IN RESPIRATORY CARE EDUCATION
Simulation-based education serves as a bridge between theoretical knowledge and real-world practice. By immersing students in clinical scenarios that replicate reallife situations, simulation helps improve knowledge, confidence, and self-efficacy in essential skills without placing patients at risk.1,2 Additionally, simulation education was necessary when more traditional education approaches were unavailable. During the COVID-19 pandemic, simulation was utilised as an alternative way for training programmes to continue providing education when students could not access clinical environments due to concerns of risks (to learners) and to preserve personal protective equipment.3
In addition to clinical preparedness, simulation-based learning facilitates interprofessional collaboration, a cornerstone of modern healthcare. Simulation provides a platform for learners to engage in interprofessional education (IPE), fostering teamwork, communication, and shared decision-making.
For example, Davis et al.1 noted in their thematic analysis of simulation use in entry-to-practice respiratory care programmes during the COVID-19 pandemic that respiratory care students worked collaboratively with physical therapy, nursing, occupational therapy, and medical school students on various topics such as mechanical ventilators and oxygen therapy devices. In 2018, Obaidan et al.4 utilised standardised patients to provide a training experience for nurses, physicians, and respiratory therapists looking to use prone positioning in patients with acute respiratory distress syndrome (ARDS). Sergakis et al.5 found that interprofessional simulation promoted teamwork, confidence, communication, and professional identity among nursing, respiratory therapy, medical dietetics, occupational therapy, physical therapy, pharmacy, medicine, and nurse practitioner students. By promoting collaboration in simulated environments, learners gain valuable experience working in interdisciplinary teams, preparing them for the complexities that exist in real-world settings.
BENEFITS OF SIMULATION-BASED LEARNING IN RESPIRATORY CARE
The benefit of simulation-based education is its ability to improve clinical competence. Simulations also allow students to practice critical procedures repeatedly until they achieve proficiency in a wide variety of topics. For instance, in a narrative review by Sreedharan et al.2 the authors noted several specific clinical areas that can be trained by simulation, including patient assessment (assessment of respiratory rate, respiratory pattern, breath sounds, and arterial blood gas sampling), therapeutic procedures (oxygen administration and airway management), mechanical ventilation, and advanced procedures.2
Another benefit of simulation is the safe learning environment it provides. In respiratory care, errors during critical situations, such as difficult airway management, can have severe consequences for patients. Simulation allows students to practice procedures in a controlled environment where mistakes can be corrected without harm.6 Beyond technical proficiency, simulation can improve decision-making, situational awareness and leadership, and interdisciplinary communication and collaboration.2,6 In simulated environments, students assess patient conditions, prioritise interventions, and adapt treatment plans to mirror the clinical settings. While the simulation experience may result in learning, educators can also utilise debriefing sessions to contribute to learning. Debriefing sessions help the learners reflect on their experiences and discuss their understanding.7
TYPES OF SIMULATION IN RESPIRATORY CARE EDUCATION
Several types of simulation are used in respiratory care education, each offering unique benefits. Simulation with manikins is commonly used in healthcare education, as higher-fidelity manikins can help simulate realistic physiological responses. Higher-fidelity simulators have been shown to improve learner performance, providing feedback on learners’ actions through verbal cues and visual displays. Interestingly, however, while higherfidelity manikins are useful in healthcare education, increased fidelity does not always confer a better educational outcome than lower-fidelity manikins.8,9
Task trainers are devices designed to train key elements of procedures or skills being learnt, such as intubation or arterial blood gas sampling. These simulators allow students to practice technical skills in isolation, building a solid foundation before integrating those skills into more comprehensive simulation scenarios. For instance, students might practice intubation on a task trainer before applying those skills during a full simulation
scenario requiring clinical decision-making, communication, and troubleshooting with a high-fidelity manikin.1,2,9
Standardised patients can also provide highly realistic simulation experiences involving a higher level of realism for the learner.1,4 Often, these are actors or individuals trained to simulate actual patients, allowing students to develop skills such as communication and patient education. This type of simulation is particularly valuable in respiratory care education, as it has been shown to increase student confidence and perception of preparedness for their clinical rotations.10
Virtual reality (VR) and augmented reality (AR) are also emerging as valuable tools in respiratory care education. These technologies allow students to engage in immersive, computer-based simulations without physical equipment. VR and AR simulations provide an alternative to traditional simulation methods, particularly in distance education settings where physical simulators are inaccessible.1,2
CHALLENGES IN IMPLEMENTING SIMULATION-BASED LEARNING
Despite its many benefits, simulationbased learning faces several challenges, particularly in its implementation. One of the most significant barriers is the cost of highfidelity simulation equipment. Manikins, simulation labs, and the associated technology require substantial financial investment, which can be prohibitive for many educational programmes with limited budgets. This highlights the significance of respiratory care education initiatives that assess the outcomes and costs of different simulation modalities. As mentioned earlier, evidence suggests that higher-fidelity manikins may not necessarily influence the outcomes of simulation-based education in some instances.8,9
In addition to the financial burden, faculty training and time to coordinate effective simulations present another challenge.3 Effective simulation-based learning requires
skilled instructors in respiratory care and the operation of simulation technology. Faculty must be trained to develop realistic scenarios, operate complex equipment, and facilitate debriefing sessions, all of which require a significant time commitment.1,2
FUTURE DIRECTIONS FOR SIMULATION IN RESPIRATORY CARE EDUCATION
Simulation-based education will likely play a more significant role in respiratory care training as technology and supportive literature evolve. One of the most promising growth areas is the increased use of VR and AR. These technologies are becoming more accessible and affordable, offering new possibilities for creating immersive and realistic learning environments.2
Another future consideration is the integration of remote learning opportunities into respiratory care education. The COVID-19 pandemic accelerated the adoption of remote learning technologies, including virtual simulation platforms that enable students to participate in clinical scenarios from any location. This flexibility makes respiratory care education more accessible, particularly for students who cannot attend in-person classes. This could be used beyond students in entry-level programmes, as it could also be beneficial in continuing medical education.
Finally, there is a pressing need for a considerable effort to address the lack of research in respiratory care simulation education. Despite advancements in technology and the growing use of simulation in healthcare education, the field of respiratory care still lacks sufficient evidence to inform best practices. The lack of data to inform educators on best practices hinders understanding of the effectiveness of various simulation modalities and their impact on learner outcomes, patient care, and cost efficiency. Efforts to generate robust data in simulation would enhance educational strategies and improve the overall quality of respiratory care education.
Key Areas for Study
The key areas include:
• comparative effectiveness of highfidelity versus low-fidelity simulation in respiratory care training;
• impact of simulation-based education on clinical performance and patient outcomes;
• cost-benefit analysis of different simulation modalities in respiratory care education;
• best practices for integrating simulation into respiratory care curricula;
• long-term retention of skills and knowledge gained through simulationbased learning; and
References
1. Davis SP et al. Simulation use in entry-into-practice respiratory care programs. Respir Care. 2022;67(6):676-81.
2. Sreedharan JK et al. Simulation-based teaching and learning in respiratory care education: a narrative review. Adv Med Educ Pract. 2024;15:473-86.
3. Davis SP et al. Simulation use in entry-into-practice respiratory care programs during the covid-19 pandemic: a thematic analysis. Respir Care Educ Annual. 2023;32:12-7.
4. Obaidan A et al. Evaluation of a
• role of interprofessional simulation in enhancing team-based care.
CONCLUSION
Simulation-based education in respiratory care is widespread, offering students a safe and controlled environment to develop critical clinical and decision-making skills. However, a pressing need remains for more research to support best practices in this field. The lack of robust data hinders a comprehensive understanding of the effectiveness of various simulation modalities and their impact on learner outcomes, patient care, and cost efficiency. Significant efforts are needed to address these gaps to generate research and data that will enhance educational strategies and improve the quality of respiratory care education.
training method to improve knowledge and confidence of prone positioning. Respir Care Ed Annual. 2018;27:3-15.
5. Sergakis G et al. The impact of interprofessional clinical simulation on attitudes, confidence, and professional identity. Respir Care Educ Annual. 2016;25:11-6.
6. King J et al. Using interprofessional simulation to improve collaborative competences for nursing, physiotherapy, and respiratory therapy students. J Interprof Care. 2016;30(5):599-605.
7. Kim YJ, Yoo JH. The utilization of debriefing for simulation in healthcare:
a literature review. Nurse Educ Pract. 2020;43:102698.
8. Kim YJ, Yoo JH. Effects of manikin fidelity on simulation-based nursing education: a systematic review and meta-analysis. J Nurs Educ. 2022;61(2):67-72.
9. Weiss T et al. High-fidelity simulation versus low-fidelity simulation. Respir Care Educ Annual. 2016;25:21-9.
10. Gardner DD et al. Using standardized patients in preclinical simulation. Respir Care Educ Annual. 2018;27:43-55.
Unveiling the Rarity: Pleural Metastasis of Papillary Thyroid Cancer – A Case Report and Clinical Implications
Authors: *Jordyn Salak,1 Ekrem Yetiskul, Samer Asmar,1 Acharya Sudeep,1 Halim El Hage,1 Manuel Villa Sanchez2
1. Department of Internal Medicine, Staten Island University Hospital, New York, USA
2. Department of Surgery, Staten Island University Hospital, New York, USA *Correspondence to jsalak@northwell.edu
Disclosure: The authors have declared no conflicts of interest.
Papillary thyroid cancer (PTC) is an epithelial malignancy arising from the follicular cells within the thyroid, typically slow-growing with a benign course (5-year survival >99% in locally contained malignancies). However, in unusual cases, this condition can spread to the pleura, leading to a malignant pleural effusion. The authors present a case of an 80-year-old female presenting with dyspnoea following treatment for suspected bacterial pneumonia. Imaging revealed a substantial left-sided pleural effusion. Despite interventions such as thoracentesis and intravenous antibiotics, the pleural effusion persisted. Subsequent video-assisted thoracic surgery revealed pleural biopsies positive for PTC, a disease previously believed to have been cured almost 6 decades ago. Pleural involvement in patients with PTC is exceptionally rare. A literature review conducted between 1992–2023 revealed merely seven published reports documenting PTC metastasis to the pleura. The authors’ case emphasises the significance of exploring various potential causes of a patient showing signs of subacute dyspnoea, particularly in individuals previously diagnosed with PTC, as it emphasises the possibilities of unforeseen recurrence, featuring the uncertainties and complexities of managing PTC.
Key Points
1. Papillary thyroid cancer (PTC) is the most common thyroid malignancy, accounting for 80–85% of cases. It has a favourable prognosis with a 93% survival rate at 10 years, but recurrence and distant metastasis can still occur, impacting survival
2. Recurrence affects about 10% of PTC patients, influenced by factors like lymph node metastasis, tumour size, and patient age. While PTC commonly spreads to regional lymph nodes, distant metastases to bones or lungs occur in 1–4% of cases. Rarely, pleural metastasis with effusion can happen.
3. The manuscript presents a rare case of pleural metastasis in an 80-year-old patient, nearly 60 years after initial PTC treatment. This case emphasises the importance of thorough diagnostic evaluation in long-term PTC survivors presenting with dyspnoea and pleural effusion.
INTRODUCTION
Papillary thyroid cancer (PTC) is the most common form of thyroid cancer, accounting for 80–85% of thyroid cancer cases. Despite being the most frequent thyroid cancer, it has the best outcomes, and is rarely metastatic.1 PTC boasts a favourable survival rate; however, recurrence is a significant concern, affecting approximately up to 10% of patients at various stages of their lives.2 The average time to recurrence spans from 6 months to several decades later.3 Several factors have been identified as contributors to an elevated risk of recurrence, including, but not limited to, lymph node metastasis, histologic variant, tumour size, extrathyroidal extension, extra nodal extension, male gender, and an age >45 years at the time of initial diagnosis.3 PTC is one of the most treatable cancers relative to other differentiated and undifferentiated thyroid malignancies, boasting a survival rate of 93% at 10 years.4 Around 30–40% of PTC metastasises to regional lymph nodes. However, distant metastasis may occur and account for 1–4% of the patients, reducing the survival rates to 24–76%.5
In 5–10% of instances, distant metastasis may manifest in the bones or lungs, and in uncommon cases, it may occur in the pleura, accompanied by the accumulation of effusive fluid.5 While metastasis to the lungs is common, metastasis to the pleura with the collection of large amounts of fluid requiring thoracentesis is rare. In the last 5 years, fewer than five cases have been described. This case report describes a patient for whom a partial thyroidectomy was performed in 1965 for PTC, who presented to the hospital with progressively worsening subacute shortness of breath found to have a large pleural effusion due to unknown recurrent metastatic disease to the pleura.
CASE PRESENTATION
An 80-year-old female with a history of hypertension and papillary thyroid cancer, treated with subtotal thyroidectomy in 1965, presented to the emergency room with acutely worsening dyspnoea. Six weeks prior to presentation, she developed symptoms mimicking her husband’s
respiratory syncytial virus infection, including a productive cough. She initially was seen at an urgent care centre 4 weeks prior to presentation, where an X-ray was performed and demonstrated a left lower lobe pneumonia. At that time, she was treated with oral amoxicillin/clavulanic acid, azithromycin, and prednisone. Despite initial improvement, her condition deteriorated, leading to severe breathlessness.
On presentation to the emergency department, vital signs included a blood pressure of 137/86 mmHg, heart rate of 62 beats per minute, temperature of 36.7 °C, respiratory rate of 19 breaths per minute, and oxygen saturation of 96% on 2 L via nasal cannula. Laboratory tests revealed an elevated D-dimer level, and normal troponin and procalcitonin levels. Computed tomography angiography was performed to exclude a pulmonary embolism, which was ruled out, but the imaging demonstrated a large left pleural effusion with compressive atelectasis (Figure 1A). The patient was admitted for respiratory failure secondary to a large left-sided parapneumonic effusion.
While on the medical floor, the patient was evaluated by the in-house pulmonologist. Given the patient’s oxygen requirements and the large nature of the effusion, the decision was made to perform a thoracentesis. Pleural fluid studies established the effusion to be an exudative effusion (Table 1). However, prior to performing the thoracentesis, on point-of-care ultrasound, the effusion had characteristics consistent with a complicated effusion. After the procedure was performed, cardiothoracic surgery was consulted. They believed the effusion to still be parapneumonic, and recommended treatment with intravenous antibiotics and outpatient follow-up for resolution.
One month after discharge, the patient was noted to have a persistent pleural effusion. This led to the performance of video-assisted thoracic surgery (Figure 1B). Biopsies taken of the pleura during the procedure were positive for metastatic thyroid papillary cancer. This diagnosis comes nearly 60 years after the patient’s initial cancer treatment.
After the procedure, a CT of the neck showed changes consistent with previous thyroid surgery and new nodules in the remaining thyroid lobe (Figure 2). The patient subsequently underwent a PET/CT that showed focal fluorodeoxyglucose uptake within the medial aspect of a consolidated left lower lobe opacity, with a maximum standardised uptake value of 8.3, suspicious for biologic tumour activity. The patient was scheduled for total thyroidectomy with neck dissection, followed by radioactive iodine treatment with pleural catheter removal 4 weeks post-surgery.
DISCUSSION
PTC, an epithelial carcinoma, is the most common of thyroid malignancies, accounting for 80–85% of all cases.1 It is distinguished by follicular nuclear patterns and the ability to invade nearby lymphatic structures.6
Slow growing, PTC has the best outcomes of the thyroid cancer groups, with a 99.5% 5-year relative survival rate amongst all Surveillance, Epidemiology, and End Results (SEER) stages combined.7 The incidence is higher among women compared to men by a 3:1 ratio.8
Only 10% of cases of PTC present with metastatic disease.1 Per guidelines from the American Thyroid Association (ATA) and National Comprehensive Cancer Network (NCCN), a conservative approach in the form of a thyroid lobectomy is sufficient for low-risk disease. Low-risk disease is defined as having no prior history of radiation, no distant metastases, no cervical lymph node metastases, no extrathyroidal extension, and a tumour ≤4 cm in diameter.9 In the case of the authors’ patient, subtotal thyroidectomy was deemed appropriate in her case, as the tumour was 2 cm and had no extrathyroidal extension or lymph node involvement.
Figure 1A: Posteroanterior view of the chest on X-ray obtained on admission demonstrated a moderate-large left pleural effusion (green arrow).
Figure 1B: Posteroanterior view of the chest on X-ray after video-assisted thoracoscopic surgery and pleural catheter insertion (green arrow).
The rate of recurrence is difficult to ascertain as all re-operations on patients having already undergone subtotal thyroidectomy or thyroidectomy are labelled as recurrent disease without differentiation for persistent disease.3 Some indicators of persistent disease include re-operation within the first year of the initial surgery.3 One randomised retrospective study demonstrated only a 4.3% risk of recurrence, mostly in the neck lymph nodes, with a median time to recurrence of 56.8 months.10 This deviates from the authors’ patient as her reoccurrence occurred 720 months after her initial procedure. It is difficult to determine the exact time of recurrence as the patient stopped monitoring her thyroid function 10 years after she was disease-free.
The incidence of pleural metastasis originating from PTC stands at 0.6% of cases.11 It is often identified through pleural fluid analysis; however, the authors’ case veers from this as they had negative cytopathology results from thoracentesis. This initially negated the possibility of
PTC recurrence. However, upon reviewing the pleural biopsy, the diagnosis of metastatic papillary thyroid cancer was conclusively established.
Metastasis of differentiated thyroid cancers, including papillary, is thought to be through lymphatic spread. Typically, metastatic spread starts in nearby lymph nodes before settling into faraway tissues. In papillary thyroid cancer the preferred metastatic sites (after the lymph nodes) include the lungs and the bones. This is due to the modification of the microenvironments of the target organ prior to the establishment of tumour cells. This alteration occurs due to cytokine-cell interactions, which are still poorly understood.4
CONCLUSION
This case emphasises the significance of exploring various potential causes of a patient showing signs of subacute dyspnoea. A thorough and accurate assessment of
Table 1: Thoracentesis results.
The CT of the neck with intravenous contrast demonstrated prior resection of the right thyroid lobe and isthmus, as well as right neck dissection. The left thyroid lobe was mildly enlarged and heterogeneous with several nodules measuring up to 1.5 cm (green arrow).
both medical and surgical history is vital in acquiring crucial details necessary for an exact diagnosis. For individuals previously diagnosed with PTC who encounter aggravated or new dyspnoea, or display a new pleural effusion, the potential of pleural metastasis should be considered. Furthermore, it emphasises the possibilities of unforeseen recurrence, featuring the uncertainties and complexities in managing PTC. Given that the patient was 60 years cancer-free, metastatic recurrence of her disease seemed unlikely. However, through thorough and invasive work-up, the correct diagnosis was found.
As the financial implications of medical practices become increasingly apparent, it is essential to acknowledge that initial investigations into pleural effusions should prioritise more prevalent and less complex aetiologies. Prematurely proceeding to invasive and costly interventions may adversely impact patient outcomes both personally and clinically. Clinicians must remain cognisant of the financial implications for patients, while emphasising the importance of thorough investigation to
achieve an accurate diagnosis. Metastatic spread of papillary thyroid cancer is a negative prognostic factor, with multiple organ metastasis being associated with higher frequency of death (50.4%) versus single organ involvement (36.7%).4 The 5-year survival rate in patients with metastasis limited to one organ was 77.6%, while that in patients who develop second organ involvement was as low as 15.3%.12
New studies are aiming to use the presence of pleural effusion in metastatic disease as an independent prognostication factor outside the typical factors that are identified for a decrease in survival. This includes age >45 years, cancer with metastasis to bone, increased tumour size and tumour size >3 cm, and incomplete tumour resection.13 This case presentation aims to enrich the existing body of medical knowledge and contribute to the ongoing advancement of the field. By sharing a detailed clinical scenario, the authors hope to enhance understanding, foster informed decision-making, and encourage further research that may lead to improved patient care and treatment protocols.
Figure 2: CT of the neck with intravenous contrast.
1. Mileva M et al. Thyroid cancer detection rate and associated risk factors in patients with thyroid nodules classified as Bethesda category III. Radiol Oncol. 2018;52(4):370-6.
2. Limaiem F, Rehman A, Anastasopoulou C, et al. Papillary Thyroid Carcinoma [Internet] (2023) Treasure Island: StatPearls. [Internet]. Treasure Island. Available from: https://www.ncbi.nlm. nih.gov/books/NBK536943/.
3. Bates MF et al. Back so soon? Is early recurrence of papillary thyroid cancer really just persistent disease? Surgery. 2018;163(1):118-23.
4. Toraih EA et al. Site-specific metastasis and survival in papillary thyroid cancer: the importance of brain and multi-organ disease. Cancers (Basel). 2021;13(7):1625.
5. Sakamoto RI et al. Recurrent papillary thyroid carcinoma with pleural metastasis diagnosed by effusion
cytology: a report of cases with clinicopathologic correlation. Hawaii J Med Public Health. 2015;74(2):51-6.
6. Fridman M et al. Morphological and clinical presentation of papillary thyroid carcinoma in children and adolescents of Belarus: the influence of radiation exposure and the source of irradiation. Exp Mol Pathol. 2015;98(3):527-31.
7. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Thyroid Carcinoma. V.3.2018. Available at: https://www.nccn.org/professionals/ physician_gls/pdf/thyroid.pdf. Last accessed: 20 February 2019.
8. Lim H et al. Trends in thyroid cancer incidence and mortality in the United States, 1974-2013. JAMA. 2017;317(13):1338-48.
9. CCN Clinical Practice Guidelines in Oncology. Thyroid Carcinoma. National Comprehensive Cancer Network. Available at http://www.nccn.org/
professionals/physician_gls/PDF/ thyroid.pdf. Last accessed: 13 June 2022.
10. Ywata de Carvalho A et al. Predictive factors for recurrence of papillary thyroid carcinoma: analysis of 4,085 patients. Acta Otorhinolaryngol Ital. 2021;41(3):236-42.
11. Vassilopoulou-Sellin R, Sneige N. Pleural effusion in patient with differentiated papillary thyroid cancer. South Med J. 1994;87:1111-6.
12. Wang LY et al. Multi-organ distant metastases confer worse diseasespecific survival in differentiated thyroid cancer. Thyroid. 2014;24:1594-9.
13. Broome DT et al. Pleural effusion as a novel prognostic factor in metastatic thyroid carcinoma. Endocr Connect. 2020;9(8):812-23.