Leaders in Oncology: Aparna Parikh, Nancy Davidson, Michael Gibson, Michael A. Postow discuss the future of the field
10 Review of the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting, May 31–June 04 2024
Congress Features
25 ASCO 2024: Highlights in Breast Cancer Research
Caroline Michie
30 Navigating Bias When Using AI in Oncology
Katrina Thornber
33 New Drugs in Oncology
Aleksandra Zurowska
Abstract Reviews
37 Longitudinal Curriculum to Address Wellness and Professional Development in a Hematology/Oncology Fellowship Program
Srikumar et al.
39 Early Palliative Care Among Patients Diagnosed with Advanced
42 Michael A. Postow
44 Lower-Risk Myelodysplastic Syndromes: Putting Anemia Under the Spotlight Interviews 46 Aparna Parikh
Nancy Davidson
60 Wearable Devices for Vital Sign Monitoring in Hematology and Oncology Patients: An Integrative Review of Implementation Barriers and Detection Performance
Hui et al.
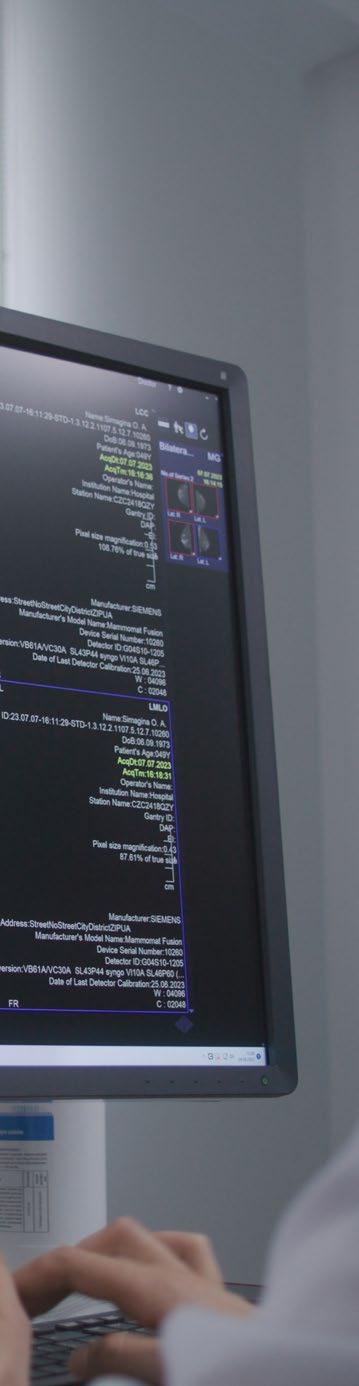
73 Recall Laterality and Bilaterality: Possible New Screening Mammography Quality Metrics
Munn et al.
"To cure sometimes, to relieve often, and to comfort always"
Editorial Board
Editor-in-Chief
Dr Erika Hamilton
Sarah Cannon Research Institute, Nashville, Tennessee, USA
Director, Breast Cancer Research Program and Chair, Executive Breast Committee
Prof Brian van Tine
Washington University School of Medicine, Missouri, USA
Dr Caroline Michie
University of Edinburgh, UK
Dr Samir Parekh
Icahn School of Medicine at Mount Sinai, New York, USA
Dr Pooja Advani
Mayo Clinic, Florida, USA
Dr Nicolò Battisti
The Royal Marsden NHS Foundation Trust, UK
Dr Roberto Leon-Ferre Mayo Clinic, Minnesota, USA
Prof Daniel McFarland
The University of Rochester Medical Center, New York, USA
Dr Ghaith Abu-Zeinah
Weill Cornell Medicine, New York, USA
Dr Ashwin Mehta
Integrative Medicine at Memorial Healthcare System, Florida, USA
Prof Benjamin Weinberg
Georgetown University, Washington D.C., USA
Aims and Scope
AMJ Oncology is an open-access, peer-reviewed eJournal committed to helping elevate the quality of healthcare in respiratory medicine by publishing high quality content on all aspects of cancer care.
The journal is published annually, 6 weeks after the American Society of Clinical Oncology Annual Meeting, and features highlights from this congress, alongside interviews with experts in the field, reviews of abstracts presented at the congress, as well as in-depth features on congress sessions. Additionally, this journal covers advances within the clinical and pharmaceutical arenas by publishing sponsored content from congress symposia, which is of high educational value for healthcare professionals. This undergoes rigorous quality control checks by independent experts and the in-house editorial team.
AMJ Oncology also publishes peer-reviewed research papers, review articles, and case reports in the field. In addition, the journal welcomes the submission of features and opinion pieces intended to create a discussion around key topics in the field and broaden readers’ professional interests. AMJ Oncology is managed by a dedicated editorial team that adheres to a rigorous double-blind peer-review process, maintains high standards of copy editing, and ensures timely publication.
Our focus is on research that is relevant to all healthcare professionals in cancer medicine. We do not publish veterinary science papers or laboratory studies not linked to patient outcomes. We have a particular interest in topical studies that advance research and inform of coming trends affecting clinical practice in the oncology field.
Editorial Expertise
AMJ is supported by various levels of expertise:
• Guidance from an Editorial Board consisting of leading authorities from a wide variety of disciplines.
• Invited contributors are recognised authorities from their respective fields.
• Peer review, which is conducted by AMJ’s Peer Review Panel as well as other experts appointed due to their knowledge of a specific topic.
• An experienced team of editors and technical editors.
Peer Review
On submission, all articles are assessed by the editorial team to determine their suitability for the journal and appropriateness for peer review.
Editorial staff, following consultation with either a member of the Editorial Board or the author(s) if necessary, identify three appropriate reviewers, who are selected based on their specialist knowledge in the relevant area. All peer review is double blind.
Following review, papers are either accepted without modification, returned to the author(s) to incorporate required changes, or rejected. Editorial staff have final discretion over any proposed amendments.
Submissions
We welcome contributions from professionals, consultants, academics, and industry leaders on relevant and topical subjects.
We seek papers with the most current, interesting, and relevant information in each therapeutic area and accept original research, review articles, case reports, and features.
We are always keen to hear from healthcare professionals wishing to discuss potential submissions, please email: editorial@americanmedicaljournal.com
To submit a paper, use our online submission site: www.editorialmanager.com/e-m-j
Submission details can be found through our website: www.emjreviews.com/contributors/authors
Reprints
All articles included in AMJ are available as reprints (minimum order 1,000). Please contact hello@emjreviews.com if you would like to order reprints.
Distribution and Readership
AMJ is distributed through controlled circulation to healthcare professionals in the relevant fields globally.
Open Access
This is an open-access journal in accordance with the Creative Commons Attribution-Non Commercial 4.0 (CC BY-NC 4.0) license.
Congress Notice
Staff members attend medical congresses as reporters when required.
AMJ Oncology is published once a year. For subscription details please visit: www.emjreviews.com
All information obtained by AMJ and each of the contributions from various sources is as current and accurate as possible. However, due to human or mechanical errors, AMJ and the contributors cannot guarantee the accuracy, adequacy, or completeness of any information, and cannot be held responsible for any errors or omissions. AMJ is completely independent of the review event (2024 ASCO Annual Meeting) and the use of the organisations does not constitute endorsement or media partnership in any form whatsoever.
Front cover and contents photograph: Chicago, Illinois marchello74 / stock.adobe.com
Editor
Evgenia Koutsouki
Vice President of Content
Anaya Malik
Editorial Manager
Darcy Richards
Copy Editors
Noémie Fouarge, Katheeja
Imani, Jenna Lorge
Editorial Co-ordinator
Abigail Craig
Editorial Assistants
Victoria Antoniou, Helena Bradbury, Ada Enesco, Laith Gergi, Katrina Thornber, Aleksandra Zurowska
Creative Director
Tim Uden
Design Manager
Stacey Rivers
Senior Designers
Roy Ikoroha, Steven Paul
Designer Owen Silcox
Junior Designers
Dillon Benn Grove, Shanjok Gurung
Senior Vice President of Business Development
Robert Hancox
Vice President of Customer Success
Alexander Skedd
Marketing Director
Kristina Mestsaninova
Chief Content Officer
Justin Levett
Chief Commercial Officer
Dan Healy
Founder and CEO
Spencer Gore
Welcome
Dear Readers,
We are extremely proud to welcome you to the inaugural issue of AMJ Oncology that brings you all the latest developments from this year’s 2024 American Society of Clinical Oncology (ASCO) Annual Meeting. Our dedicated team had the opportunity of attending this great event, which in an era of AI innovations chose to adopt the overarching theme of palliative care, highlighting the importance of the human element and compassion in patient care.
Highlighting key themes in breast cancer from ASCO 2024 is an unmissable feature article that comprehensively summarizes advances in the topic, from the first DESTINY-Breast06 results for metastatic breast cancer to the utility of circulating tumor DNA in high-risk ER+ HER2 negative early breast cancer. Make sure to also take a look at our exclusive interviews with experts who offer their insights on melanoma research, gastrointestinal oncology, and breast cancer.
For those of you interested in innovations in the field, an article examining wearable devices for vital sign monitoring in hematology and oncology patients would be of interest.
I would like to take the opportunity to thank our authors, interviews, our newly formed editorial board, and our peer reviewers for this issue, which is packed with quality content. Until the next issue, we look forward to your submitted manuscripts that feature your insights, perspectives, and research in the field.
Permissions and copyright: accountsreceivable@emjreviews.com
Evgenia Koutsouki Editor
Reprints: info@emjreviews.com
Media enquiries: marketing@emjreviews.com
We provoke conversation around healthcare trends and innovation - we also create engaging educational content for healthcare professionals. Join us for regular conversations with physician & entrepreneur, Jonathan Sackier. Listen Now
Foreword
Dear Colleagues,
We are excited to present to you the first issue of AMJ Oncology, filled with a diverse array of content, featuring compelling articles and interviews with leading experts in the field.
Our coverage includes highlights from 2024 American Society of Clinical Oncology (ASCO) Annual Meeting, where groundbreaking studies and trials were unveiled. Caroline Michie provides a comprehensive review of key data in breast cancer, emphasising the latest advancements in metastatic breast cancer treatment and pivotal research outcomes that are reshaping clinical practice. Contained here is also an interview with Michael A. Postow, Chief of the Melanoma Service at Memorial Sloan Kettering Cancer Center, New York, on his experience at ASCO.
Reina Cheong Shing Hui et al. explore the practical challenges and performance metrics of integrating wearable technology into patient care, particularly in monitoring vital signs critical to hematology and oncology practices. Another noteworthy contribution, 'Recall Laterality and Bilaterality: Possible New Screening Mammography Quality Metrics', by Samson Munn et al., examines emerging metrics in mammography quality
assessment, shedding light on potential advancements in breast cancer screening practices.
AMJ is privileged to publish interviews with distinguished experts in the field. Aparna Parikh, Medical Director for the Young Adult Colorectal Cancer Center at Massachusetts General Hospital (MGH), shares her insights on gastrointestinal oncology and the rising incidence of early-onset colorectal cancer.
I would like to thank the Editorial Board for their commitment to this new journal
In addition, we have interviews with Mike Gibson, Director of the Esophageal Cancer Program at Vanderbilt-Ingram Cancer Center, and Nancy Davidson, renowned breast cancer oncologist from Fred Hutchinson Cancer Center.
I would like to thank the Editorial Board for their commitment to this new journal, and to all contributors, reviewers, and interviewees whose invaluable insights continue to drive excellence in oncology research.
ASCO 2024
To cure sometimes, to relieve often, and to comfort always
Review of the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting Congress Review
THE ART of cancer care, the “human side of human medicine”, involves engaging with patients and their families with deep compassion and integrating supportive or palliative care as a crucial part of all treatment.
The opening words of the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting by Congress President Lynn Schuchter stressed the importance of patient care and equitable access to healthcare.
“While we continue advancing oncology science and fully leveraging the new and latest technologies, we must ensure these innovations benefit all patients,” she stated. As an expert in melanoma, a cancer that was once considered hopeless, Schuchter has witnessed the transformation of the melanoma treatment landscape over the last decades, with the advent of powerful immunotherapies and targeted therapies, such as PD-1 antibodies and BRAF inhibitors, that have drastically improved patient outcomes.
For the first time in 25 years, the ASCO presidential theme touched on palliative care. Schuchter advocated for meaningful patient support throughout the cancer experience, and honoring patients’ and families’ preferences. She drew on her personal experience with a young patient who, unfortunately, did not survive a year after her melanoma diagnosis. Re-emphasizing a
fundamental concept of medicine, she quoted Hippocrates: “To cure sometimes, to relieve often, and to comfort always, is all that may be reasonably expected of medicine.” Comfort is not optional, and it involves the delicate communication of extremely difficult information. According to recent research, oncologists deliver bad news to patients an average of 35 times per month. Furthermore, patients often interpret a 20% response rate as a 20% cure rate, unless given more explicit information. Schuchter emphasized the need for better training of clinicians in patient communication, to avoid misunderstandings, allow patients to cope with information, and best allow for advanced care planning.
This year, ASCO has been committed to helping its members become just as skilled in the art of care as they are in the science. The 2024 program includes educational sessions, communications workshop, and a plenary session on how to deliver quality palliative care through telemedicine. Schuchter stressed that integration of palliative care globally is more important than ever: “We are facing a worldwide health crisis in oncology.” By 2040, the World Health Organization (WHO)
estimates 29.5 million new cancer diagnoses per year, and cancer-related deaths will skyrocket to a projection of >16 million.
ASCO’s goal is to lower cancer-related mortality, and ease patient suffering through education, research, and professional development
To tackle this crisis, ASCO’s goal is to lower cancer-related mortality, and ease patient suffering through education, research, and professional development. This 2024 was a record year, with more than 7,000 abstracts submitted, and 44,000 in-person and virtual attendees. Furthermore, over the past 5 years, ASCO has created regional councils
in Asia Pacific, Latin America, sub-Saharan Africa, and Central and Eastern Europe to address region-specific cancer challenges. Free ASCO membership is also being provided to all oncology care professionals from low- and lower-middle income countries.
Closing her talk, Schuchter reminded the audience that, in a new era where AI algorithms can analyze complex brain MRIs in minutes, assess a tumor’s genetic makeup, or identify the best treatment avenue for patients, “no machine can explain to a patient, with human compassion, what their choices are, and what their future may hold.”
Read on for key insights from ASCO 2024, and come back next year for our coverage of ASCO 2025, also taking place in Chicago, from May 30–June 3
Asciminib: Promising First-Line Treatment for Chronic Myeloid Leukemia
A NEW study presented at ASCO 2024 highlights asciminib as a promising treatment for newly diagnosed chronic phase chronic myeloid leukemia (CML).
Asciminib, a ‘Specifically Target the ABL Myristoyl Pocket’ (STAMP) drug, has shown superior efficacy and a more favorable safety profile compared to current standard tyrosine kinase inhibitors (TKI). The Phase III ASC4FIRST trial involved 405 patients with recently diagnosed chronic phase CML, randomly assigned to receive either asciminib (201 patients) or an investigator-selected TKI (204 patients), such as imatinib or a second-generation TKI. The median age of participants was 52 years, and the study included a diverse patient population from cancer centers in 29 countries.
After 48 weeks, 68% of patients treated with asciminib achieved a major molecular response (MMR), compared to 49% in the TKI group. Additionally, 39% of asciminib patients reached a deep molecular response, suggesting potential for treatment-free remission. Subset analyses showed that asciminib was more effective than both imatinib and second-generation TKIs. For instance, 69% of patients in the imatinib subset who received asciminib achieved MMR, compared to 40% in the imatinib
group. Similarly, 66% of those in the second-generation TKI subset who received asciminib achieved MMR, versus 58% in the corresponding TKI group.
Asciminib's safety profile was notable, with fewer adverse events and lower rates of treatment discontinuation compared to TKIs. Common side effects in the asciminib group included low platelet and neutrophil counts, but severe side effects like blood clots were rare, occurring in only 1% of participants. This combination of high efficacy and better tolerability positions asciminib as a potential first-line treatment for chronic phase CML.
The study's lead author, Timothy Hughes, emphasized that asciminib’s potency and safety could enable more patients to achieve treatment-free remission, the goal of CML therapy. Researchers will continue to monitor long-term outcomes, including overall survival, progression-free survival, and the potential for treatment-free remission, to further establish asciminib's role in CML therapy.
After 48 weeks,
%
of patients treated with asciminib achieved a major molecular response
Longest Progression-Free Survival Reported in Advanced Non-small Cell Lung Cancer with Lorlatinib
NEW research presented at ASCO 2024 by lead study author Benjamin Solomon, Head of Lung Medical Oncology at the Peter MacCallum Cancer Center in Melbourne, Australia, revealed unprecedented progression-free survival (PFS) in advanced nonsmall cell lung cancer (NSCLC) with the use of lorlatinib, paving the way for new treatment outcomes.
Only 4 out of 114
patients in the lorlatinib group who did not present with brain metastases at the beginning of the study developed brain metastases within the first 16 months of treatment
The study demonstrated how lorlatinib, a third-generation anaplastic lymphoma kinase (ALK) tyrosine kinase inhibitor (TKI), provided the longest progression-free survival ever recorded in patients with advanced ALKpositive NSCLC.
The Phase III CROWN clinical trial included 296 participants (59.1% female; 43.9% Asian; median age: 59 years) with advanced, previously untreated ALK-positive NSCLC, who were randomly assigned to receive either lorlatinib (149 patients) or crizotinib (147 participants). In the beginning of the study, 25% of the participants had brain metastases.
As of October 31st 2023, results showed that 50% of participants in the lorlatinib group were still receiving treatment, compared to just 5% in the crizotinib group. The median PFS for the lorlatinib group has not yet been reached, indicating that more than half of the patients have not experienced disease progression. In contrast, the median PFS was only 9.1 months for the crizotinib group. Additionally, the 5-year PFS rate was reported at 60% in the lorlatinib group, which was significantly higher than the crizotinib group at 8%.
Notably, only 4 out of 114 patients in the lorlatinib group who did not present with brain metastases at the beginning of the study developed brain metastases within the first 16 months of treatment. Additionally, the median time to disease progression in the brain had not yet been reached with lorlatinib, whereas it had with crizotinib at 16.4 months.
Treatment-related adverse events occurred in 77% of patients in the lorlatinib group and in 57% of patients in the crizotinib group, with 5% discontinuing lorlatinib and 6% discontinuing crizotinib. Reported adverse events included edema, high cholesterol, and hyperlipidemia.
Lorlatinib has demonstrated an unprecedented duration of disease control in patients with ALK-positive NSCLC, included those with brain metastases. The findings of this study indicate that lorlatinib offers significant advantage over second-generation ALK TKIs, providing better possibilities for long-term management of NSCLC. The study will continue to monitor the participants to determine if lorlatinib also leads to longer overall survival compared to crizotinib, and to establish the median PFS for lorlatinib.
Novel Combination Therapy Minimizes Adverse Side Effects in Hodgkin Lymphoma
NOVEL combination anti-cancer therapy is effective at reducing the risk of advanced-stage classic Hodgkin lymphoma progression, relapse, or disease, resulting in a high 4-year progression-free survival rate of 94.3%.
Progressionfree survival was higher for patients receiving BrECADD at
94.3 %
The standard intensive chemotherapy regimen, BEACOPP (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone), is an effective curative treatment for classic Hodgkin lymphoma, comprising seven anti-cancer drugs. However, patients often experience acute, chronic, and potentially long-lasting adverse side effects. Researchers presented findings on an open-label Phase III clinical trial evaluating a novel combination therapy's side effects and effectiveness at ASCO 2024.
90.9 %
compared to for patients receiving BEACOPP
The GHSG-HD21 study was a multicenter, randomized clinical trial composed of 742 patients receiving the novel BrECADD therapy (brentuximab vedotin, etoposide, cyclophosphamide, doxorubicin, dacarbazine, and dexamethasone) and 740 receiving BEACOPP. Patients in the BrECADD regimen group had individualized treatment adapted to the patient's risk profile. Patients enrolled in the study were ≤60 years old with a diagnosis of advanced-stage classic Hodgkin lymphoma (average age: 31 years). Researchers used PET to determine the number of treatment cycles patients should receive, ranging from four to six.
Results from the study revealed that at a 4-year follow-up, an equivalent number of patients receiving BreCADD and BEACOPP (64%) were eligible for fewer treatment cycles. Progression-free survival was higher for patients receiving BrECADD at 94.3% compared to 90.9% for patients receiving BEACOPP. Disease progression in the BrECADD group was significantly reduced by 34% compared to the BEACOPP group. Moreover, the individualized treatment with BrECADD enabled 64% of patients in the BrECADD group to finish their treatment cycles in 3 months. Severe blood-related side effects arose in 31% of BrECADD group compared to 52% in the BEACOPP group, with almost all patients in the BrECADD group fully recovering from adverse events within 1 year.
These results led the authors to conclude that novel BrECADD treatment is associated with improved survival outcomes and reduced severe side effects in patients with advanced-stage classic Hodkin lymphoma compared to BEACOPP. The researchers aim to increase treatment efficacy without contributing to side effects, possibly by adding PD-1 inhibitors to BrECADD, thus reducing the number of treatment cycles.
Impact of Lymphadenectomy on Advanced Ovarian Cancer Outcomes
A randomized Phase III clinical trial called the CARACO trial has demonstrated that patients undergoing surgery for advanced ovarian cancer may avoid additional lymph node removal without compromising survival outcomes.
This research, presented at ASCO 2024, underscores efforts to reduce surgical morbidity while maintaining efficacy in cancer treatment. The study focused on advanced epithelial ovarian cancer, evaluating the necessity of lymphadenectomy during primary cancer surgery. Traditionally, lymphadenectomy was part of the standard treatment protocol, which included tumor removal followed by chemotherapy. However, findings from previous clinical trials indicated that omitting lymphadenectomy did not adversely affect survival rates.
Conducted between December 2008–March 2020, the Phase III CARACO trial involved 379 participants with advanced epithelial ovarian cancer, none of whom showed lymph node involvement before or during surgery. Participants were randomly assigned to either undergo lymphadenectomy (181 participants) or not (187 participants). Approximately 75% of participants received neoadjuvant chemotherapy before surgery.
The study's primary outcomes revealed no significant differences in survival between the two groups. Median progression-free survival was 14.8 months for those without lymphadenectomy compared to 18.5 months
for those with the procedure. Median overall survival was 48.9 months versus 58 months, respectively. These differences were not statistically significant. Participants who underwent lymphadenectomy experienced higher rates of post-operative complications, such as additional surgeries to address bleeding or fluid buildup (8.3% versus 3.2%) and transfusions (34% versus 25%). The mortality rate within 60 days of surgery was similar between groups (1.1% versus 0.5%).
The CARACO trial reinforces the findings of a 2019 clinical trial termed the LION trial, suggesting that lymphadenectomy can be safely omitted in advanced ovarian cancer surgeries, thereby reducing surgical complications without affecting survival outcomes. This approach may enhance post-operative recovery and resource allocation. Jean-Marc Classe, Institut de Cancerologie de l'Ouest, Nantes University, France, emphasized the trial's significance in informing surgical practices post-neoadjuvant chemotherapy. Future research will focus on assessing lymphadenectomy's role in patients with evident lymph node involvement prior to surgery. The CARACO study marks a critical step in refining surgical strategies for advanced epithelial ovarian cancer.
This research underscores efforts to reduce surgical morbidity while maintaining efficacy in cancer treatment
Neoadjuvant Immunotherapy Significantly Improves Outcomes in Stage III Melanoma
ADMINISTRATION of immunotherapy for melanoma before surgery has been shown to significantly improve outcomes for patients with Stage III melanoma compared to postsurgical immunotherapy.
At 12 months
83.7 %
of neoadjuvant therapy patients were event-free, compared to of adjuvant therapy patients
Disease recurrence is a common phenomenon in patients receiving standard therapeutic lymph node dissection followed by adjuvant therapy to treat their melanoma. Researchers presented the NADINA Phase III trial results at the 2024 ASCO Annual Meeting. The trial compared outcomes between patients receiving the combined immunotherapy before surgery and those receiving standard post-surgical immunotherapy.
57.2 %
The NADINA Phase III trial was a multicenter study comprised of 423 patients from Europe and Australia, with 212 participants receiving neoadjuvant therapy, and 211 receiving adjuvant therapy. The patients who enrolled had cancer that had spread to the lymph nodes and required surgery. Patients were treated with ipilimumab and nivolumab before surgery, and monitored for a median of 9.9 months. If the tumor response was insufficient, they received additional adjuvant therapy post-surgery.
The results showed significantly fewer disease-related events in the neoadjuvant group compared to the adjuvant group (28 versus 72 events). At 12 months, 83.7% of neoadjuvant therapy patients were eventfree, compared to 57.2% of adjuvant therapy
patients. Furthermore, around 60% of patients in the neoadjuvant group required no additional adjuvant therapy after achieving a major pathological response. The trial also assessed outcomes based on the presence of a BRAF mutation. Among patients with a BRAF mutation, 83.5% of those receiving neoadjuvant therapy were event-free at 12 months, compared to 52.2% of those receiving adjuvant therapy. For patients without a BRAF mutation, the event-free survival rates were 83.9% for the neoadjuvant group and 62.4% for the adjuvant group.
Researchers noted that, although the neoadjuvant approach showed increased efficacy, it also came with higher rates of severe side effects (29.7% versus 14.7% in the adjuvant group), including infections, diarrhea, abnormal blood counts, rash, fever, and fatigue. The authors concluded that NADINA underscores the potential of neoadjuvant immunotherapy to improve survival outcomes in Stage III melanoma, supporting the shift towards personalized and response-driven treatment strategies. The NADINA trial is the first Phase III trial to assess and demonstrate the superiority of neoadjuvant immunotherapy for Stage III melanoma.
Osimertinib Revolutionizes Treatment for Locally Advanced EGFR-Mutated NSCLC
Research
presented at ASCO 2024 by lead study author Suresh Ramalingam, Winship Cancer Institute of Emory University, Atlanta, Georgia, USA, suggests that osimertinib significantly improves progression-free survival in patients with unresectable Stage III epidermal growth factor receptor (EGFR)-mutated non-small cell lung cancer (NSCLC).
The Phase III LAURA trial enrolled patients with unresectable Stage III NSCLC with EGFR mutations who showed no disease progression during or after definitive platinum-based chemoradiotherapy. Patients were randomly assigned in a 2:1 ratio to receive either osimertinib (143 patients) or placebo (73 patients). Key patient characteristics included a median participant age of 62 years in the osimertinib group and 64 years in the placebo group; 63% female in the osimertinib group and 58% female in the placebo group; and 63% with no history of smoking in the osimertinib group, and 67% in the placebo group.
Results showed that osimertinib significantly reduced progressionfree survival (PFS), with a median PFS of 39 months versus only 6 months in the placebo group
Results showed that osimertinib significantly reduced progression-free survival (PFS), with a median PFS of 39 months versus only 6 months in the placebo group. Additionally, in the osimertinib group, 74% of participants
had no cancer growth after 12 months, and 65% after 24 months, compared to the placebo group (22% versus 13%). Osimertinib also showed a higher objective response rate, reducing cancer size by at least 30% with the treatment, compared to placebo (57% versus 33%). Additionally, the rate of new brain metastases was significantly lower in the osimertinib group at 8%, compared to placebo at 29%.
Common side effects associated with osimertinib occurred in both study groups. These side effects included radiation pneumonitis, diarrhea, and rash. However, it was reported that most patients presented with mild cases of radiation pneumonitis. Due to severe adverse events, 13% of patients discontinued therapy in the osimertinib group, and 5% in placebo.
The study will continue to follow the participants to evaluate the impact of osimertinib on overall survival, brain metastases, and other outcomes. Ongoing monitoring will help to determine the longterm benefits of osimertinib for patients with locally advanced EGFR-mutated NSCLC.
Improving Esophageal Cancer Outcomes with Post-operative Chemotherapy
NEW insights into the treatment of locally advanced esophageal adenocarcinoma have revealed that administering chemotherapy before and after surgery (the FLOT protocol) significantly improves patient survival compared to the traditional approach of pre-operative chemoradiotherapy (the CROSS protocol), according to research presented at ASCO 2024.
FLOT recipients experienced a %
30 lower risk of dying within this period [3 years]
The results were obtained from a Phase III ESOPEC clinical trial conducted across 25 centers in Germany. The trial involved 438 patients, predominantly male, with a median age of 63 years, all diagnosed with locally advanced, resectable esophageal adenocarcinoma. The participants were divided into two groups: 221 patients received the FLOT protocol, while 217 patients were treated with the CROSS protocol. Key findings revealed that 403 participants started treatment, and 371 proceeded to surgery. Post-surgery, 4.3% of the patients had died within 90 days (3.2% in the FLOT group versus 5.6% in the CROSS group).
After a median follow-up of 55 months, 218 participants had died (97 from the FLOT group and 121 from the CROSS group). The median overall survival was notably higher for the FLOT group at 66 months, compared to 37 months for the CROSS group. Three-year survival rates were 57% for FLOT and 51% for
CROSS, with FLOT recipients experiencing a 30% lower risk of dying within this period.
The results demonstrate that in patients with resectable esophageal adenocarcinoma, a combination of pre-operative and postoperative chemotherapy (FLOT) provides better outcomes than pre-operative chemoradiotherapy alone (CROSS). Researchers plan to explore if surgery can be avoided in patients who achieve a complete pathological response to FLOT or CROSS treatments, and show no cancer growth during active surveillance. This approach could preserve the esophagus, significantly enhancing the patient's quality of life. These findings may influence national and international treatment guidelines, potentially establishing the FLOT protocol as the preferred standard of care for locally advanced, resectable esophageal cancer.
Early Palliative Care Boosts Outcomes in Patients With Lung Cancer
RESEARCH shows that early palliative care enhances outcomes for patients with advanced non-small cell lung cancer, including survival.
Telehealth has the potential to significantly lessen the burden on patients, clinicians, and healthcare resources, while preserving quality care. The findings of this study presented at ASCO 2024 emphasizes the crucial need for healthcare systems and policymakers to integrate telehealth more widely into evidence-based palliative care standards.
This randomized comparative effectiveness trial included 1,250 patients recently diagnosed with advanced non-small cell lung cancer. Patients attended palliative care sessions every 4 weeks, conducted through video visits for those in the telehealth group and in person for those in the traditional care group. These sessions addressed physical and psychological symptoms, coping, illness, understanding care preferences, and treatment decisions. The mean age of patients was 65.5 years, with 54.0% identifying as women, and 66.7% being married or partnered. The racial diversity in the study was 10.4% African American or Black, 5.2% Asian, 82.7% White, and 4.8% Hispanic or Latino.
Patient quality-of-life scores were statistically similar between the telehealth and in-person groups (99.67 versus 97.67 on a scale of 0–136) at 24 weeks. Caregiver participation was significantly lower in the telehealth group compared to the in-person group (36.6% versus 49.7%). There were no significant differences between the two groups in patient-reported depression, anxiety, or coping skills.
Research shows that early palliative care enhances outcomes for patients with advanced non-small cell lung cancer
The researchers in the future plan to investigate whether particular patient subgroups benefit more from telehealth or in-person care, including assessments based on age and proficiency in technology. Additionally, they plan to study the effects of both care delivery methods on the quality of end-of-life care, especially regarding patient-clinician communication about care preferences, to further refine and optimize palliative care protocols.
Trastuzumab Deruxtecan Enhances Progression-Free Survival in Patients with Breast Cancer
RESEARCH presented at ASCO 2024 by Giuseppe Curigliano, University of Milan and European Institute of Oncology in Milan, Italy, has shown that trastuzumab deruxtecan benefits patients with human epidermal growth factor receptor 2 (HER2)-low and HER2-ultra-low metastatic cancer, and significantly improves progression-free survival in patients with metastatic breast cancer that was previously treated with endocrine therapy.
This has the potential to improve treatment strategies, and utilize treatment earlier in the management of HER+ metastatic breast cancer, especially in patients who did not previously benefit from targeted therapies post-endocrine treatment.
The study included 866 participants with metastatic breast cancer, categorized into patients with either HER2-low (713 participants) or HER2-ultra-low (153 participants) cancers. HER2-low cancer group had an immunohistochemistry score of 1+ or 2+, indicating moderate HER2 protein expression, while HER2-ultra-low cancer group had a score >0 but <1+. All participants had received at least one prior endocrine treatment, and nearly 90.4% has also received targeted therapy with a cyclin-dependent kinase 4/6 inhibitor. Patients were randomly assigned to receive either trastuzumab deruxtecan (436 participants) or a physician’s choice of chemotherapy (430 participants), including capecitabine, nab-paclitaxel, or paclitaxel.
Results showed that progression-free survival for patients with HER2-low cancer was 13.2 months with trastuzumab deruxtecan versus 8.1 months in patients who underwent chemotherapy. Similar events were noted in the HER2-ultra-low group. Patients with HER2-low cancer who received trastuzumab deruxtecan had a 38% lower chance of cancer progression compared to those on chemotherapy. The
objective response rate was 56.5% for trastuzumab deruxtecan versus 32.3% for chemotherapy in patients with HER2-low cancer. For HER2-ultra-low cancer, the objective response rate was 61.8% with trastuzumab deruxtecan versus 26.3% with chemotherapy.
In terms of side effects and treatment duration, trastuzumab deruxtecan treatment lasted longer than chemotherapy (median of 11 months versus 5.6 months respectively), with fewer side effects. Serious side effects occurred in about 41% of patients on trastuzumab deruxtecan versus 31% on chemotherapy. Interstitial lung disease was noted in 11% of patients, consistent with previous research, leading to treatment discontinuation in about 5% of cases, and three deaths.
The study will continue to monitor the patients to evaluate overall survival outcomes and analyze additional secondary endpoints, including patient-reported outcomes; the authors will also undertake exploratory translational analyses to further understand the impact of these drugs.
The findings of this study have the potential to transform treatment options for metastatic breast cancer and offer new options for patients who have exhausted other endocrine and targeted therapy options.
Progression-free survival for patients with HER2-low cancer was
13.2 months 8.1 months with trastuzumab deruxtecan versus in patients who underwent chemotherapy
Belantamab Mafodotin: An Effective Addition to Multiple Myeloma Treatment
DISEASE progression and mortality rates are significantly reduced in patients with relapsed or refractory multiple myeloma when belantamab mandolin is incorporated into the treatment regimen, according to recent findings from the DREAMM-8 clinical trial.
The DREAMM-8 trial, presented at ASCO 2024, evaluated the efficacy of belantamab mafodotin combined with pomalidomide and dexamethasone (BPd), compared to the current standard regimen of pomalidomide, bortezomib, and dexamethasone (PVd). The study included 302 patients with relapsed or refractory multiple myeloma. After a median follow-up of 22 months, the trial demonstrated that the median progressionfree survival (PFS) was not reached for patients treated with BPd, whereas it was 12.7 months for those on the PVd regimen. One year into the study, 71% of patients receiving BPd remained free of disease progression compared to 51% of those receiving PVd. The overall response rate was higher in the BPd group at 77% versus 72% in the PVd group, with 40% of BPd-treated patients achieving a complete or better response compared to 16% in the PVd group.
Both treatment groups experienced high rates of side effects, with over 99% of BPd recipients and 96% of PVd recipients reporting adverse effects. Eye-related side effects, including corneal changes and blurred vision, were notably more common in the BPd group (89%) than in the PVd group (30%). These side effects were generally manageable
through dose adjustments or temporary discontinuation of belantamab mafodotin, allowing most patients to continue benefiting from the treatment.
The DREAMM-8 trial evaluated the efficacy of belantamab mafodotin combined with pomalidomide and dexamethasone
The findings from the DREAMM-8 trial demonstrate that belantamab mafodotin, combined with pomalidomide and dexamethasone is more effective than the standard PVd regimen. Lead study author Suzanne Trudel, Princess Margaret Cancer Centre, Toronto, Canada, proposed that the addition of belantamab mafodotin should be a standard treatment option for patients with multiple myeloma at first relapse and for subsequent relapses. The researchers will continue to monitor participants to determine long-term outcomes, including overall survival and the duration of response in those treated with BPd. These findings could potentially lead to a new standard of care for relapsed or refractory multiple myeloma, offering hope for better management of the disease.
Addressing Chemotherapy Toxicity Disparities
RACIAL and ethnic differences in chemotherapy toxicity have been observed but are often understudied due to low minority enrolment in clinical trials.
Trials in the USA particularly lack Black participants, which concerns racial disparities in cancer outcomes. Black patients with breast cancer face higher mortality rates and more severe toxicity. This study presented at ASCO 2024 demonstrates the successful enrolment of females with African ancestry with early-stage breast cancer to evaluate a germline predictor of taxane-induced peripheral neuropathy, and compare toxicity between two taxane drugs in this population.
Black patients with breast cancer face higher mortality rates and more severe toxicity
Research has shown that Black patients with breast cancer experience significantly more treatment-induced peripheral neuropathy (TIPN) than other races, with specific genetic differences influencing this risk. Higher rates of TIPN often lead to chemotherapy dose reductions and lower cure rates. To address this, the ECOG-ACRIN Cancer Research Group designed the EAZ171 trial to validate genetic predictors of neuropathy and determine the optimal taxane drug, focusing on side effects and potential dose reductions for Black patients with early-stage breast cancer. The trial's design and patient recruitment involved collaboration with Black patient advocates, including Indianapolis-
based ‘Pink-4-Ever – Ending Disparities’. A strong social media campaign, featuring Black females with breast cancer, was developed for recruitment. Many participants were enrolled through the National Cancer Institute’s Community Oncology Research Program (NCORP), not just from academic settings.
In the study, 249 Black females with earlystage breast cancer were treated with either weekly paclitaxel or tri-weekly docetaxel. Of these, 121 received at least one dose of paclitaxel and 118 received docetaxel.
Black patients with breast cancer treated with docetaxel experienced less TIPN and fewer dose reductions compared to those on paclitaxel. Inherited gene alterations were more common in patients with TIPN, but this was not statistically significant. Physicianreported that Grade 2–4 neuropathy rates did not differ significantly between high- and low-risk gene alteration groups. However, Grade 2–4 neuropathy was significantly higher in patients on paclitaxel by both physician reports (44% versus 29%) and patient reports (40% versus 24%). Patients on paclitaxel required more dose reductions due to peripheral neuropathy (28% versus 9%) or any cause (39% versus 25%).
The researchers plan another trial to further optimize therapy for Black patients with breast cancer.
ADRIATIC Trial: Durvalumab as Consolidation Treatment
FINDINGS from the ADRIATIC trial were presented in a plenary session at ASCO 2024.
The median OS for the durvalumab group was
59.9 months 33.4 months compared to for the placebo group
The interim results were from a Phase III study exploring the efficacy of durvalumab as a consolidation treatment for patients with limited-stage small-cell lung cancer (LS-SCLC) who had not progressed following concurrent platinum-based chemoradiotherapy (cCRT).
The ADRIATIC trial was a randomized, double-blind, placebo-controlled study. It involved 730 patients who were eligible with a WHO performance status of 0 or 1 with Stage I–III LS-SCLC. The patients were randomized to receive either durvalumab (1,500 mg) plus placebo, durvalumab (1,500 mg) plus tremelimumab (75 mg), or placebo plus placebo every 4 weeks for four cycles. Maintenance doses of durvalumab or placebo were administered every 4 weeks until disease progression or intolerable toxicity, for a maximum of 24 months. Randomization was stratified by disease stage and whether patients had received prophylactic cranial irradiation.
The interim analysis showed statistically significant improvements in the dual primary endpoints, overall survival (OS) and progression-free survival (PFS), for patients treated with durvalumab compared to placebo.
The median OS for the durvalumab group was 55.9 months compared to 33.4 months for
the placebo group (hazard ratio [HR]: 0.73; 95% CI: 0.57–0.93; P=0.0104). The 24-month OS rate was 68.0% for durvalumab versus 58.5% for placebo, and the 36-month OS rate was 56.5% versus 47.6%, respectively. The median PFS was 16.6 months for durvalumab compared to 9.2 months for placebo (HR: 0.76; 95% CI: 0.61–0.95; P=0.0161). The 18-month PFS rate was 48.8% for durvalumab versus 36.1% for placebo, and the 24-month PFS rate was 46.2% versus 34.2%.
Durvalumab was generally well tolerated. Grade 3/4 adverse events occurred in 24.3% of the durvalumab group versus 24.2% in the placebo group. Discontinuation due to adverse events was higher in the durvalumab arm (16.3% versus 10.6%), and the incidence of pneumonitis/radiation pneumonitis was also higher (38.0% versus 30.2%). The safety profile of durvalumab remained consistent with previous studies.
The ADRIATIC trial’s interim results demonstrated the potential of durvalumab as a new standard of care for patients with LS-SCLC post-cCRT. Ongoing analysis of the durvalumab plus tremelimumab arm will shed more light on the role of combination immunotherapy in this setting, offering survival benefits to patients without introducing new safety concerns.
ASCO 2024: Highlights in Breast Cancer Research
Author: *Caroline Michie1
1. Edinburgh Cancer Centre and University of Edinburgh, UK
The theme of this year’s American Society of Clinical Oncology (ASCO) Annual Meeting was ‘The Art and Science of Cancer Care: From Comfort to Cure’, with over 5,000 abstracts presented and over 200 educational sessions. The sun shone again in Chicago, USA, between May 31–June 4 for more than 40,000 attendees, reassuringly demonstrating that the appetite for in-person congresses with all the networking opportunities and other collaborative benefits brings us back to normal following the COVID-19 pandemic.
METASTATIC BREAST CANCER
First DESTINY-Breast06 Results
Perhaps the most anticipated results in the breast cancer track came from the Phase III DESTINY-Breast06 clinical trial.1 The hall was packed for the early morning session for the late-breaking results of the study of trastuzumab deruxtecan (T-DXd) versus chemotherapy of physician’s choice (TPC; capecitabine, paclitaxel, or nabpaclitaxel) as first-line cytotoxic therapy in estrogen receptor (ER)+ve HER2 low or ultra-low breast cancer, after progression on endocrine and targeted therapy in the metastatic setting.1 Positive results have almost come to be expected from trials of T-DXd, and this was no exception. A total of 886 chemotherapy-naive patients were randomized, with the most common TPC option being capecitabine (60%); 17.5% were considered HER2 ‘ultra-low’ and the median prior lines of therapy was two. Nearly 90% of patients had received prior CDK4/6 inhibitor therapy.
With a median duration of follow-up of 18 months the hazard ratio (HR) for progressionfree survival (PFS) of 0.62 (0.51–0.74; p<0.0001), median PFS (mPFS) improved from 8.1 months with TPC to 13.2 months with T-DXd in the HER2 low cohort, with a 5-month improvement representing a similar magnitude of mPFS benefit to the DESTINY-Breast04 trial.2 Subgroup analysis showed all groups benefited from T-DXd. The overall response rates were impressive, at 57.3% versus 31.2%. Rates of interstitial lung disease were slightly lower than in some prior DESTINY studies, at 11.3% for any grade, of which the majority was Grade 2 (8.3%); however, there were three deaths. No other new safety signals were seen, and rates of clinically significant cardiac impairment were low. Results from the HER2 ultra-low cohort alone were numerically consistent with the overall population. The overall survival (OS) data remains immature, with an HR of 0.81 (0.65–1.00), but 20.1% of patients in the TPC arm subsequently went on to receive T-DXd. These results confirm again the efficacy of T-DXd in this disease biology and will trigger debate on the optimal timing of use of T-DXd in this disease setting.
PostMONARCH Data
In a similar disease subtype, the postMONARCH study results were presented by Kevin Kalinsky.3 This study randomized 368 patients with estrogen receptor positive (ER+) metastatic breast cancer to fulvestrant plus either abemaciclib or placebo in patients experiencing disease progression on CDK4/6 inhibitors (59% palbociclib, 34% ribociclib, and 8% abemaciclib) and an aromatase inhibitor. Approximately 60% of participants had documented visceral metastatic disease.
These results confirm again the efficacy of T-DXd in this disease biology and will trigger debate on the optimal timing of use of T-DXd in this disease setting
This study met its primary endpoint of improving investigator-assessed PFS, with an HR of 0.73 (0.57–0.95; p=0.02), but the numerical mPFS was only 6.0 versus 5.3 months after 258 events triggered the primary analysis. The subgroup analysis showed a possible higher benefit in the patients who had received first-line palbociclib. However, the confidence intervals were wide for the other treatment groups, and this interaction was not statistically significant. In the exploratory biomarker studies, there were no signals suggesting that any specific molecular (PIK3CA/AKT1/ESR1/ PTEN altered) subgroup benefited more from this approach, but the pre-specified subgroup without visceral metastases appeared to benefit most. This study is the first to show a statistically significant benefit of fulvestrant with continuation of CDK4/6 inhibition after progression on a CDK4/6 inhibitor and AI, although the benefits are modest. In discussion of the relevance of this study, single agent fulvestrant, the comparator arm, would only infrequently be considered a guideline-recommended therapeutic strategy in 2024, and is more usually reserved for patients with co-morbidities or another reason to choose a therapy with low risk of toxicity.
Germline Mutation-Associated Metastatic Breast Cancer
Poly-ADP ribose polymerase inhibitors are already firmly established as treatment in several germline BRCA1/2-associated solid tumors, but less data is available for the role of these agents in cancers associated with other mutations associated with homologous recombination repair deficiency. The TBCRC-048 study4 was an investigatorinitiated proof-of-principle study of olaparib in 30 patients with somatic BRCA1/2 mutations (sBRCA) and 24 with germline PALB2 (gPALB2) mutations. The results of these expansion cohorts were presented by Nadine Tung, reporting that in the gPALB2 cohort, 18 confirmed responses were seen for an impressive overall response rate of 75% (80% CI: 60.2–86.3), and a clinical benefit rate at 18 weeks of 83.3% (90% CI: 65.8–94.1). The median PFS was 9.6 months (90% CI: 8.3–12.4). In the sBRCA cohort, there were 11 confirmed responses for objective response rate of 36.7% (80% CI: 24.8–50). Clinical benefit rate was 53.3% (90% CI: 37–69.2) and median PFS was 5.6 months (90% CI: 3.0–8.3).
Other highlights include patient-reported outcomes from the TROPION-15 and INAVO1206 studies, in addition to the largest study of real-world data comparing first-line CDK4/6 inhibitor therapy, PALMARES-2,7 in over 1,800 patients across 18 Italian cancer centers. There was also a small Phase II study of patients receiving tucatinib, trastuzumab, and capecitabine for metastatic HER2 positive breast cancer with leptomeningeal disease, which is the first prospective study to show clinically meaningful benefit signals (response, symptom improvement, quality of life, and survival) with systemic therapy in HER2 positive leptomeningeal disease.8
These data strongly suggest that patients with ER-low EBC should be counseled regarding the benefit of adjuvant ET, and practice guidelines should continue to recommend ET in this setting
EARLY BREAST CANCER
Predicting the Benefit of Chemotherapy in Pre-menopausal Patients
Moving to early breast cancer (EBC), further prospectively-collected data from the RxPONDER study was presented.9 This study had already reported that in pre-menopausal females, chemo-endocrine therapy (ET) had an invasive disease-free survival (iDFS) improvement compared to ET alone (HR: 0.60; 95% CI: 0.43–0.83) in patients with Oncotype Dx recurrence scores of <25. This sub-study sought to further refine which measure of pre-menopausal status best predicted benefit from the addition of chemotherapy. Patients with baseline serum anti-Müllerian hormone (AMH) levels ≥10 pg/ mL showed significant benefit from chemoET compared to patients with AMH levels <10 pg/mL, with an absolute improvement of 7.8% in 5-year iDFS. AMH levels were shown to be a superior tool for selecting
patients for chemotherapy benefit than selfreported menopause status, age, or estradiol/ luteinizing hormone/follicle-stimulating hormone levels. This simple measure could be used to more accurately select patients for the addition of adjuvant chemotherapy to ET.
Omission of Adjuvant Endocrine Therapy in Estrogen Receptor Low Early Breast Cancer
Although not a new therapy, there remains debate and some equipoise about the role of adjuvant ET in low ER (defined as ER 1–10%) EBC. The US National Cancer Database between 2018–2020 was interrogated for outcomes among an initial population of over 350,000 patients. Of these, 7,956 were identified as having Stage I–III low ER EBC and had received chemotherapy.10 Adjuvant ET was omitted in 41% of patients, and this was associated with worse overall survival. In an unadjusted analysis, omission of ET
was associated with worse OS (HR: 1.40; 95% CI: 1.19–1.65; p<0.001), with similar effects regardless of PR, HER2, or Ki67 (each interaction test p>0.3). The adjusted hazard after sensitivity analysis of ET omission on OS was 1.24 (95% CI: 1.02–1.51; p=0.03). Although retrospective and non-randomized, given the size of the study, these data strongly suggest that patients with ERlow EBC should be counseled regarding the benefit of adjuvant ET, and practice guidelines should continue to recommend ET in this setting.
Utility of Circulating Tumor DNA in High-Risk ER+ HER2 Negative
Early Breast Cancer
Important biomarker data from the monarchE trial11 of adjuvant abemaciclib in high-risk ER+ HER2 negative EBC was presented, focusing on the serum ct-DNA results. Patient characteristics and treatment effects were similar between the overall trial population and the biomarker cohort, but the biomarker group (n=910) was enriched with more patients with an invasive DFS event (27% versus 18%). At baseline, 92% of patients had no detectable circulating tumor DNA (ctDNA), but 10% subsequently did develop detectable ctDNA during the study period. Conversely, of the 8% of patients who were ctDNA positive at baseline, 59% of these remained persistently elevated, and 41% subsequently had negative results. Despite enrolling a high-risk population, it is notable that overall, the incidence of ctDNA detection was relatively low, with only 17% of patients having detectable ctDNA at any time.
Baseline ctDNA detection was associated with significantly worse outcomes, with the 4-year iDFS rate being 79% in the baseline negative cohort, versus 20% in the baseline positive group (nominal p<0.0001). In patients with baseline negative ctDNA results, only 23% experienced an iDFS event (recurrence), in contrast to 80% in the baseline positive group. The predictive value of the test was improved with serial testing, and those who remained persistently negative on
serial testing had the best outcomes, with 14% experiencing recurrence versus those who had baseline positive results that subsequently became negative (n=24; 42% iDFS recurrence rate) and those who became positive on treatment or were persistently positive (93% and 100%, respectively).
This study further strengthens the argument that the standard of care should continue to be checkpoint blockade for early TNBC starting in the neoadjuvant setting
These data suggest that ctDNA detection is highly prognostic of worse outcomes, and although to date there is no data that treatment of molecular relapse improves outcomes, ctDNA clearance may be a useful outcome measure for the evaluation of efficacy and intensification of adjuvant therapy in the future. There are several ongoing clinical trials evaluating early treatment for clinically undetectable molecular relapse, which will be awaited with great interest.
NATALEE Node Negative Cohort Results
Initial results of the NATALEE trial12 of adjuvant ribociclib in ER+ HER2 negative EBC were presented in December 2023, and an update was presented regarding the nodenegative cohort involving 613 patients. A total of 71% had received prior chemotherapy, and the discontinuation rate was 24%. After 38.7 months of follow-up, there was a reported non-significant trend to improvement (iDFS HR: 0.73 [0.412–1.368], with a 3-year iDFS rate of 93.2% versus 90.6%) in favor of the ribociclib arm. Safety data was reassuring in this curative cohort, but longer follow-up will be important to gain a better understanding of the magnitude of benefit in this setting.
Adjuvant PD-L1 Inhibition in Triple Negative Breast Cancer
Other highlights included the A-BRAVE clinical trial,13 another study investigating a PD-L1 inhibitor, on this occasion, avelumab, in 466 patients with high-risk early triple negative breast cancer. This study did not demonstrate a significant improvement in 3-year DFS (HR: 0.81 [0.61–1.09] in the overall population; 0.80 [0.58–1.10] in the post-neoadjuvant cohort), but intriguingly there was a reported 8.5% overall survival improvement (HR: 0.66 [0.45–0.97]). This study further strengthens the argument that
References
1. Curigliano G et al. Trastuzumab deruxtecan (T-DXd) vs physician’s choice of chemotherapy (TPC) in patients (pts) with hormone receptorpositive (HR+), human epidermal growth factor receptor 2 (HER2)-low or HER2ultralow metastatic breast cancer (mBC) with prior endocrine therapy (ET): primary results from DESTINY-Breast06 (DB-06). Abstract LBA1000. ASCO 2024, May 31-June 4, 2024.
2. Modi S et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022;387(1):9-20.
3. Kalinsky K et al. Abemaciclib plus fulvestrant vs fulvestrant alone for HR+, HER2- advanced breast cancer following progression on a prior CDK4/6 inhibitor plus endocrine therapy: primary outcome of the Phase 3 postMONARCH trial. Abstract LBA1001. ASCO 2024, May 31-June 4, 2024.
4. Tung NM et al. TBCRC 048 (olaparib expanded) expansion cohorts: Phase 2 study of olaparib monotherapy in patients (pts) with metastatic breast cancer (MBC) with germline (g) mutations in PALB2 or somatic (s) mutations in BRCA1 or BRCA2. Abstract 1021. ASCO 2024, May 31-June 4, 2024.
5. Pernas S et al. Datopotamab deruxtecan (Dato-DXd) vs chemotherapy (CT)
the standard of care should continue to be checkpoint blockade for early triple negative breast cancer starting in the neoadjuvant setting.
CONCLUSION
The above summary represents selected highlights and are only a small snapshot of the breadth of data presented at ASCO 2024, an undoubted key congress for professionals working in the field of breast cancer research and/or care.
in previously treated inoperable or metastatic hormone receptor-positive, HER2-negative (HR+/HER2–) breast cancer (BC): patient-reported outcomes (PROs) from the TROPION-Breast01 study. Abstract 1006. ASCO 2024, May 31-June 4, 2024.
6. Juric D et al. First-line inavolisib/ placebo + palbociclib + fulvestrant (Inavo/Pbo+Palbo+Fulv) in patients (pts) with PIK3CA-mutated, hormone receptor-positive, HER2negative locally advanced/metastatic breast cancer who relapsed during/within 12 months (mo) of adjuvant endocrine therapy completion: INAVO120 Phase III randomized trial additional analyses. Abstract 1003. ASCO 2024, May 31June 4, 2024.
7. Vernieri C et al. Comparison of antitumor efficacy of firstline palbociclib, ribociclib, or abemaciclib in patients with HR+/HER2- aBC: results of the multicenter, real-world, Italian study PALMARES-2. Abstract 1014. ASCO 2024, May 31-June 4, 2024.
8. O’Brien BJ. Tucatinib-trastuzumabcapecitabine for treatment of leptomeningeal metastasis in HER2+ breast cancer: TBCRC049 phase 2 study results. Abstract 2018. ASCO 2024, May 31-June 4, 2024.
10. Choong GMY et al. The impact of adjuvant endocrine therapy (AET) omission in ER-low (1-10%) early-stage breast cancer. Abstract 513. ASCO 2024, May 31-June 4, 2024.
11. Loi S et al. Prognostic utility of ctDNA detection in the monarchE trial of adjuvant abemaciclib plus endocrine therapy (ET) in HR+, HER2-, nodepositive, high-risk early breast cancer (EBC). Abstract LBA507. ASCO 2024, May 31-June 4, 2024.
12. Yardley DA. Baseline (BL) characteristics and efficacy endpoints for patients (pts) with node-negative (N0) HR+/ HER2− early breast cancer (EBC): NATALEE trial. Abstract 512. ASCO 2024, May 31-June 4, 2024.
13. Conte PF et al. A-BRAVE trial: A phase III randomized trial with avelumab in early triple-negative breast cancer with residual disease after neoadjuvant chemotherapy or at high risk after primary surgery and adjuvant chemotherapy. Abstract LBA500. ASCO 2024, May 31-June 4, 2024.
9. Kalinsky K et al. Correlation of serum anti-Müllerian hormone (AMH) levels on identification of premenopausal patients (pts) with hormone receptor positive (HR+), HER2-negative, node-positive breast cancer most likely to benefit from adjuvant chemotherapy in SWOG S1007 (RxPONDER). Abstract 505. ASCO 2024, May 31-June 4, 2024.
OPTIMISING patient care and survival with AI is a rapidly advancing field of medical research. During the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting, a symposium titled “Using ‘Artificial’ Intelligence to Achieve ‘Real’ Improvements in Cancer Care” explored the use of innovative AI algorithms in oncology. Experts presented breakthroughs in diagnostic and predictive AI, whilst increasing awareness of inherent bias in AI models that can perpetuate into clinical outcomes.
HOW AI IS TRANSFORMING ONCOLOGY
James Zou, Standford University, California, USA, began the session by explaining some of the AI techniques used to change the care and outcomes of patients with cancer. Two of the main uses of AI in oncology are to, firstly, diagnose, and secondly, to predict specific outcomes or trajectories. Zou explained that a standard regression or classification AI model, often referred to as predictive AI, produces a single output, such as whether a patient does or does not have cancer. In contrast, generative AI models generate richer and more flexible outputs, such as detailed descriptions of diseases and specific molecular structures (which can be helpful during drug discovery). Both predictive and generative AI have numerous applications in oncology research. Predictive AI is employed in diagnosing cancer and predicting treatment responses, whilst generative AI can be utilized in designing more inclusive clinical trials, acting as a co-pilot for clinicians, and a source of medical information for patients.
Two of the main uses of AI in oncology are to first diagnose, and secondly, to predict specific outcomes or trajectories
One example highlighted by Zou is the development of an AI algorithm called Trial Pathfinder, an AI framework designed to systematically evaluate clinical trial eligibility criteria.1 The analyses revealed that many common criteria had minimal impact on trial hazard ratios. By adopting a data-driven approach to broaden these restrictive criteria, the pool of eligible patients more than doubled, and the hazard ratio for overall survival decreased by an average of 0.05. This indicates that many patients previously deemed ineligible under the original trial criteria, often due to age, health, or gender, could potentially benefit from the trial treatments. The use of this AI model not only directly provides more treatment options for patients, but also addresses the issue of insufficient participant recruitment in clinical trials, which often leads to less conclusive results. With more patients participating in trials, research can advance more rapidly, ultimately improving patient outcomes.
An example of how AI can diagnose patients with cancer was presented by Daniel Kates-Harbeck, University Hospital LMU, Munich, Germany. Kates-Harbeck and colleagues developed the first researchgrade prognostic model for distant metastasis risk in HR+/HER2- early-stage breast cancer. Specifically, the AI model combines histopathology image data from pre-treatment breast biopsy and surgical hematoxylin and eosin slides, with clinical prognostic factors (age, tumor stage, node stage, and tumor size) to predict the risk of distant recurrence. There was a significant association with the risk of distant recurrence in the validation cohort (sub-distribution hazard ratio: 2.3; 95% CI: 2.0–2.8) and remained significant after adjusting for the clinical factors (sub-distribution hazard ratio: 2.2; 95% CI: 1.7–2.8). With this strategy, there is no need for additional tissue biopsy, therefore it may reduce diagnosis times. Kates-Harbeck noted that the future work aims to generalize this research-grade model to clinical-grade utility across diverse demographics and clinical settings.
USING AI TO MITIGATE DISPARITIES IN HIGH-RISK POPULATIONS
Alyson Moadel, Montefiore Einstein Comprehensive Cancer Center, Bronx, New York, USA, engaged the audience with an abstract presentation showcasing how AI can go beyond predicting diagnosis and outcomes. Moadel presented ‘MyEleanor’, an algorithm that aims to increase patient engagement in high-risk populations.2 She began by explaining that engagement is key to improving patient outcomes, as patient adherence increases when they have a better understanding of the medical procedures involved. For example, at an NYC cancer center serving ethnically minoritized and disadvantaged populations, 59% of patients either canceled or did not show up for their colonoscopy appointments in 2022. Barriers to colorectal cancer screening uptake can contribute to late-stage diagnosis and poor outcomes, which lead to the development of MyEleanor. This is an AI-enabled virtual care assistant that makes thousands of highly personalized phone calls each day, with the ability to detect subtle changes in a patient’s voice. MyEleanor not only increases patient engagement, but is able to detect targeted needs, triage patients, and send actionable information to healthcare professionals.
Through this project, it was revealed that the most significant barriers to screening were lack of perceived need (19%), time constraints (18%), insufficient encouragement from physicians (16%), medical mistrust (14%), concerns about findings (13%), and cost (12%). With MyEleanor, the completion rate for patients who did not show up for initial appointments nearly doubled from 10% to 19% from 2022 to 2023, and overall patient volume increased by 36% (41% of which were Hispanic and 33% were Black). This project demonstrates the potential of AI to mitigate disparities in cancer screening through increased engagement. The next phase of the project will examine the impact on patient preparation adherence, staff burden, and revenue, as well as other screening programs such as those for breast and lung cancer.
of patients either canceled or did not show up for their colonoscopy appointments in 2022 %
Another way AI can reduce disparities in oncology healthcare is by using language models to simplify medical documentation for patients, as a lack of medical understanding may prevent appointment and treatment adherence in certain individuals. Using AI to generate patient-accessible consent forms has recently been recently implemented at Lifespan, the largest healthcare system in Rhode Island, USA.3
NAVIGATING INHERENT RACIAL AND GENDER BIASES IN AI
Whilst AI can be used to mitigate disparities in healthcare, Judy Gichoya, Emory University, Atlanta, Georgia, USA, gave a highly insightful talk on the inherent bias in data used to develop AI models, and how this bias perpetuates into healthcare decisions. For example, clinical notes made by healthcare professionals, which may be racially biased, are becoming an increasingly common source of data for machine learning and AI algorithms in healthcare. Gichoya described a recent study revealing that AI models can infer patient race from clinical notes even after removing explicit racial indicators, and those models trained on race-redacted notes can still perpetuate existing biases in clinical treatment decisions.4 Gichoya advocated that increased transparency and accountability regarding bias that is implicitly embedded in data, and the real-world implications of this are vital when implementing AI into oncology.
Alexander T. Pearson, University of Chicago, Illinois, USA, further emphasized this point by highlighting that, whilst AI can offer the potential of improved performance with minimal increased time or cost, without an accurate and transparent description of AI model feature importance, there is limited understanding and therefore mitigation of inherent bias in the model.
References
1. Liu R et al. Evaluating eligibility criteria of oncology trials using real-world data and AI. Nature. 2021;592(7855):629-33.
2. Moadel A et al. AI virtual patient navigation to promote re-engagement of U.S. inner city patients nonadherent with colonoscopy appointments: a quality improvement initiative. J Clin Oncol. 2024;42(Suppl 16):100.
3. Mirza FN et al. Using ChatGPT to facilitate truly informed medical consent. NEJM AI. 2024;DOI:10.1056/ AIcs2300145.
4. Adam H et al. Write it like you see it: detectable differences in clinical notes by race lead to differential model recommendations. AIES. 2022;1:7-21.
The 2024 American Society of Clinical Oncology (ASCO) Annual Meeting showcased groundbreaking advancements in oncology, with notable sessions led by renowned experts in the field. The Meeting showcased sessions on new drugs that are transforming the landscape of cancer therapy, offering new hope to patients worldwide.
NIROGACESTAT IN DESMOID TUMORS
Mrinal Gounder, Memorial Sloan Kettering Cancer Center, New York, USA, presented nirogacestat as a newly FDA-approved treatment for desmoid tumors in November 2023. Desmoid tumors are non-cancerous but locally aggressive connective tissue growths, often occurring in the abdomen, arms, and legs, affecting about 2–4 individuals per million annually. They can cause pain, immobility, and complications like bowel obstruction, but do not metastasize and rarely cause mortality.
Gounder noted: “In the last 5–6 years, surgery is no longer the primary treatment for desmoid tumors, due to causing more adverse effects and mortality than the disease itself.” However, only about 20% of desmoid tumors can spontaneously regress/resolve in a select few patients. Gounder continued by quoting findings from a study by Colombo et al.,1 which assessed the behavior of primary sporadic desmoid fibromatosis managed by active surveillance. The primary endpoint was progression-free survival (PFS) at 3 years, with treatment-free survival (TFS) also analyzed. Results showed that 39% of patients experienced disease progression, while spontaneous regression was observed in 25% initially, and in 31%
after progression. PFS at 36 months was 54.5%, and TFS was 65.9%. Larger tumor size, extremity location, and S45F mutation were associated with shorter TFS, suggesting that active surveillance is viable but requires careful monitoring of certain risk factors.1
In the last 5–6 years, surgery is no longer the primary treatment for desmoid tumors
Gounder continued by describing the mechanism of action of the drug, highlighting one of his own studies that compared the efficacy, safety, and tolerability of nirogacestat versus placebo in patients with progressing desmoid tumors. Nirogacestat is a gamma secretase inhibitor that disrupts the dysregulated Notch signaling in desmoid tumors. In the Phase III trial, nirogacestat significantly improved PFS and quality of life (QoL) compared to placebo, with a hazard ratio of 0.29. At 2 years, 76% of nirogacestat patients were event-free compared to 44% for placebo. The drug also demonstrated higher response rates and symptom relief across various subgroups, including those with prior chemotherapy or tyrosine kinase inhibitor treatment.2
Common side effects include diarrhea, nausea, rash, and fatigue, with unique
concerns such as ovarian toxicity in women. Gounder recommended regular monitoring of hormone levels and potential fertility preservation for female patients. Other side effects like nasal congestion, skin rash, and diarrhea can be managed with dose adjustments and supportive care.
Nirogacestat is the only FDA-approved drug for the treatment of desmoid tumors and is effective in first or subsequent lines of therapy. The drug offers a significant advancement in the treatment of desmoid tumors, emphasizing improved QoL and symptom management.
FRUQUINTINIB IN METASTATIC COLORECTAL CANCER
Cathy Eng, Vanderbilt-Ingram Cancer Center, Nashville, Tennessee, USA, presented fruquintinib, a selective oral inhibitor of vascular endothelial growth factor receptors (VEGFR) 1, 2, and 3, as a new treatment for colorectal cancer (CRC), approved by the FDA in November 2023. This approval followed
previous treatments with fluoropyrimidine, oxaliplatin, irinotecan-based chemotherapy, anti-VEGF therapy, and, for RAS wild-type metastatic CRC, anti-EGFR therapy. Indicated for third-line or later settings in unresectable metastatic colorectal carcinoma, fruquintinib’s approval is based on improved overall survival (OS). The current 5-year survival rate for metastatic colorectal carcinoma patients is 15%.
Eng highlighted fruquintinib’s mechanism, which inhibits VEGFR to impact angiogenesis, proliferation, and survival. The current FDA indication is based on two prior Phase III trials. The first one was the FRESCO study, conducted in China, which demonstrated a median OS increase from 6.6 to 9.3 months;3 while another FRESCO-2 study showed a median OS improvement from 4.8 to 7.4 months, confirming significant survival benefits in heavily pre-treated patients.4 She also highlighted the health-related QoL findings from FRESCO-2, showing that fruquintinib did not negatively impact health-related QoL and improved the time to deterioration in health utility.
To highlight the potential clinical utilization of fruquitinib, Eng described a case study of one of a 56-year-old woman who presented with a history of unresectable, microsatellitestable, RAS mutant tumor type metastatic CRC, who had previously received FOLFOX+ bevacizumab, with residual Grade 2 neuropathy and FOLFRI+ bevacizumab, and who was seeking new treatment options. Her Eastern Cooperative Oncology Group (ECOG) performance status was 1, and laboratory tests were within normal limits. After consulting with the patient and advising her of different treatments and associated side effects, the patient opted for treatment with fruquitinib at 5 mg daily. However, after 3 months of treatment, the patient reported increased discomfort of her left thumb and her right heel during cycle three of Week 2. She was started on emollients and proceeded with a 1-week treatment delay. The patient is currently on cycle four and reports no residual hand-foot skin reactions. The patient decided not to decrease her dose as symptoms resided and opted to continue therapy.
BELZUTIFAN FOR ADVANCED RENAL CELL CARCINOMA
Eric Jonasch, Department of Genitourinary Medical Oncology, University of Texas MD Anderson Cancer Center, Houston, Texas, USA, presented belzutifan as a new treatment for advanced renal cell carcinoma (RCC). Belzutifan is an oral inhibitor of hypoxiainducible factor 2 alpha approved for the treatment of von Hippel-Lindau disease and RCC following prior treatment with immune checkpoint inhibitors and tyrosine kinase inhibitors.
Jonash described a case study of a 64-yearold woman with metastatic clear cell RCC who underwent nephrectomy for T3a Grade 3 clear cell carcinoma but developed new pulmonary nodules 18 months later. She was initially treated with ipilimumab and nivolumab. However, post-treatment she experienced regrowth of lung nodules and mediastinal adenopathy after 15 months. Cabozantinib
was administered as a second-line treatment, which worked initially, but after 9 months she experienced progression in the lung once again. Jonash identified belzutifan as a further treatment option for this patient. He mentioned results from the Phase III LITESPARK-005 study by Albiges et al.,5 which showed that belzutifan demonstrated significant antitumor activity in advanced clear cell renal cell carcinoma, and significantly improved PFS and objective response rate compared to everolimus, with more patients remaining progression-free at 12 and 18 months. The study showed complete responses in 3.5% of the belzutifan group versus none in the everolimus group. Additionally, belzutifan presented with a better safety profile, with fewer discontinuations in the belzutifan group versus everolimus.5
Fruquintinib did not negatively impact health-related QoL and improved the time to deterioration in health utility
Jonash went on to describe some notable adverse effects of belzutifan and everolimus, such as anemia and fatigue, which are an expected side effect of the drug; however, he also pointed out that hypoxia is a side effect that physicians need to be aware of.
To further underline this, he described another clinical case where the patient began treatment with belzutifan at 120 mg daily and was instructed to monitor their oxygen saturation. One week after treatment initiation, the patient noticed changes in their oxygen saturation; Oxygen saturation at rest dropped from a baseline of 95% to 87%, but rose above 90% with physical activity. After a short break from belzutifan, and subsequent dose reduction to 80 mg daily, the patient’s oxygen saturation returned to above 90%.
CONCLUSION
This insightful session showcased how emerging drugs like nirogacestat, fruquintinib, and belzutifan can advance treatments in oncology, offering improved PFS and QoL, and effective management of side effects for various cancers. Nirogacestat provides a novel approach in the treatment of desmoid tumors, fruquintinib extends survival in patients with metastatic CRC, and belzutifan offers a promising option for advanced RCC.
References
1. Colombo et al. A prospective observational study of active surveillance in primary desmoid fibromatosis. Clin Cancer Res. 2022;28(18):4027-32.
2. Gounder et al. Nirogacestat, a γ-secretase inhibitor for desmoid tumors. N Engl J Med. 2023;388(10):398-912.
3. Li J et al. Effect of fruquintinib vs placebo on overall survival in patients with previously treated metastatic colorectal cancer: the FRESCO randomized clinical trial. JAMA. 2018;319(24):2486–96.
4. Dasari et al. Fruquintinib versus placebo in patients with refractory metastatic colorectal cancer (FRESCO-2): an international, multicentre, randomised, double-blind, phase 3 study. Lancet. 2023;402(10395):41-53.
5. Albiges at al. LBA88 Belzutifan versus everolimus in participants (pts) with previously treated advanced clear cell renal cell carcinoma (ccRCC): randomized open-label phase III LITESPARK-005 study. Ann Onc. 2023;34(Suppl 2):S1329-30.
Abstract Reviews
These abstracts were presented at the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting and discuss burnout and professional fulfilment in the oncology and hematology field, as well as early integration of palliative care in patients newly diagnosed with advanced cancers.
Longitudinal Curriculum
to Address Wellness and Professional Development in a Hematology/ Oncology Fellowship Program
Authors: Thejal Srikumar,1 Jessica M. Stempel,1 Sarah B. Goldberg,2 Nikolai A. Podoltsev,3 David A. Braun,2 Alfred I. Lee,3 *Tara Sanft2
1. Hematology/Oncology, Yale University School of Medicine, New Haven, Connecticut, USA
2. Medical Oncology, Yale School of Medicine, New Haven, Connecticut, USA
3. Hematology, Yale University School of Medicine, New Haven, Connecticut, USA *Correspondence to tara.sanft@yale.edu
Disclosure: The authors have declared no conflict of interest.
Keywords: Burnout, curriculum, fellowship, professional fulfillment.
Burnout is widespread in medicine, with up to 60% of oncologists and 20% of oncology fellows in the USA reporting burnout.1 Currently, there are no systematic ways to address this issue in hematology/oncology (HO) fellowship programs. In contrast to burnout, professional fulfillment is defined as happiness or meaningfulness, self-worth, self-efficacy, and satisfaction at work.2 The authors implemented a longitudinal
curriculum addressing professional fulfillment in their HO fellowship program.
METHODS
Interventions to address wellness were initiated in the authors’ HO fellowship program, in the academic year (AY) 2022–2023, based on a needs assessment, including faculty-led sessions, fellow debrief sessions, and team-building activities.3 In AY 2023–2024, a new baseline needs assessment was distributed to fellows to determine topics of interest for developing a fellowship retreat and discussion throughout the year. This assessment also included three validated surveys: the Mini ReZ survey to evaluate the learning environment,4 the Patient Health Questionnaire 2 (PHQ2) to assess for depressed mood,5 and the Generalized Self-Efficacy Scale.6 Surveys were completed anonymously in person and online, and were done in July 2023, September 2023, January 2024, and February 2024. An end-of-the-year focus group was held with fellows for summative feedback. T-test and Chi-square test were used for statistical analysis.
RESULTS
Twenty-two out of 27 fellows (81.5%) completed the baseline assessment in July 2023. Topics of interest included ‘professional boundary setting’ and ‘sharing concerns and success'. Day-long, off-site fellowship retreats were designed to address the topics identified in the needs assessment, and divided into senior and first-year fellow retreats. The retreat agenda included session such as a ‘Leader’s Summit’, in which fellows visually depicted obstacles to overcome; ‘The Boundaries We Choose’, in which fellows discussed how to define boundaries in work; ‘Communicating for Improved Outcomes’, in which fellows did an exercise in active listening; and ‘Envisioning the Future’, in which fellows created vision boards of what they hoped their futures would look like. Of the 27 fellows who attended the retreats, 22 responded to post-retreat surveys, with 21 of 22 fellows indicating they found the retreat helpful (95.4%). Beyond the retreat, four didactic sessions were implemented during the AY, focusing on ‘Grief and Awe’, which included writing reflections on the topics ‘Shame Resilience’, in which fellows discussed shame in medicine; ‘Truth Rounds’,
in which senior faculty shared struggles in their careers and how they overcame them; and ‘Conflict Styles’, in which fellows selfassessed their approach to conflict. A focus group at the end-of-the-year attended by 10 fellows revealed that the curriculum was wellreceived, with representative quotes listed in Table 1. The Mini ReZ, General Efficacy, and PHQ2 survey scores did not significantly change throughout the year.
CONCLUSIONS
The development of a curriculum to address professional fulfillment, including fellowship retreats that focused on topics identified by a needs assessment, was found to be helpful among HO fellows. Objective assessments evaluating learning environment and selfefficacy did not change throughout the year, and additional surveys will be obtained to measure the ongoing effect of the curriculum. This curriculum could serve as a model for other programs, and be integrated into existing trainee resources to address HO fellow wellness and professional development of skills during training.
Longitudinal Applicability of Skills
Creating Space to Share
“There was a shared sense of - I’m not alone in feeling these things, and hearing it from those that have been quite far out of training and hearing some of those thoughts echoed was pretty validating.”
“To me, I think it added community building, and it felt that we are all related to each other, we were vulnerable.”
“I will say to me it was useful having moved from institution to institution, it was a nice way in terms of getting a sense of the universality of the medical experience where it is not just an institutiondependent thing.”
“You could argue that this [curriculum] was more important than some of the other lectures, where next year guidelines shift and trials come out, but ‘how do I be a person talking to another person’ is a pretty timeless skill.”
“I liked discussing burnout and methods to try and prevent burnout.”
“I think how open everyone was about their experiences was cool and surprising, both as trainees and faculty who participated. Many times, we think we are more secretive about experiences, and it was nice to see when a space was created, people will talk about their experiences.”
“We don't often share the things that inspire/motivate us, so it was impactful to learn these things that are important to my co-fellows.”
Table 1: Themes identified by fellows regarding the professional fulfillment curriculum.
Theme Quote
Empathic Connection
References
1. Subbiah IM et al. Wellbeing and burnout among oncology fellows compared to prior fellows and current practicing oncologists: an ASCO State of Cancer Care in America (SOCCA) trend analysis. JCO Oncology Practice. 2023;19(Suppl 11):47.
2. Jyothindran R et al. Fulfillment, burnout and resilience in emergency medicine-correlations and effects on patient and provider outcomes. PLoS One. 2020;15(10):e0240934.
3. Srikumar T et al. A multifaceted approach to wellness in a hematology/oncology fellowship program. Journal of Clinical Oncology. 2023;41(Suppl 16):11006.
4. Linzer M et al. The Mini Z Resident (Mini ReZ): psychometric assessment of a brief burnout reduction measure. J Gen Intern Med. 2023;38(2):545-8.
5. Kroenke K et al. The Patient Health Questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41(11):1284-92.
6. Schwarzer R, Jerusalem M, “Generalized self-efficacy scale,” J Weinman et al. (eds), Measures in Health Psychology: A User’s Portfolio. Causal and Control Beliefs (1995), Windsor: NFER-NELSON, pp.35-7.
Early Palliative Care Among Patients Diagnosed with Advanced Cancers Between 2010–2019 in the USA: Trends and Contribution of Provider Variation
Jason Zheng,4 Jingxuan Zhao,4 Joan Warren,5 K. Robin Yabroff,4 Xuesong Han4
1. University of Virginia School of Medicine, Charlottesville, USA
2. University of Pittsburgh School of Public Health, Virginia, USA
3. UT Southwestern Medical Center, Dallas, Texas, USA
4. American Cancer Society, Atlanta, Georgia, USA
5. American Cancer Society, Atlanta, Georgia, USA (Retired)
*Correspondence to xin.hu@virginia.edu
Disclosure: Hu received a grant from the PhRMA Foundation and St. Jude Children’s Research Hospital. Yabroff has served on the Flatiron Health Equity Advisory Board and received honoraria from the National Comprehensive Cancer Network (NCCN). All other authors declared no conflicts of interest.
Acknowledgements: The authors acknowledge the efforts of the National Cancer Institute (NCI); the Office of Research, Development and Information (ORDI), Centers for Medicare & Medicaid Services (CMS); Information Management Services (IMS); and the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEERMedicare database.
The collection of cancer incidence data used in this study was supported by the California Department of Public Health according to
California Health and Safety Code Section 103885; Centers for Disease Control and Prevention’s (CDC) National Program of Cancer Registries, under cooperative agreement 1NU58DP007156; the NCI’s Surveillance, Epidemiology and End Results Program under contract HHSN261201800032I awarded to the University of California, San Francisco, USA, contract HHSN261201800015I awarded to the University of Southern California, Los Angeles, USA, and contract HHSN261201800009I awarded to the Public Health Institute, Oakland, California, USA. The ideas and opinions expressed herein are those of the authors and do not necessarily reflect the opinions of the State of California, Department of Public Health, the NCI, or the CDC, or their contractors and subcontractors.
Keywords: Early palliative care, cancer care, provider practice variation, organization structures.
Early integration of palliative care (PC) is recommended for advanced cancers given its clinical benefits for quality of life and survival, but evidence of its use and the role of provider practice patterns and organizational characteristics in uptake is limited.1 This study examined recent trends of early PC among Medicare beneficiaries
newly diagnosed with advanced cancers, and provider- and organization-variation in the receipt of early PC.
MATERIAL AND METHODS
The authors identified patients aged ≥65.5 years newly diagnosed with advanced-stage breast, colorectal, non-small cell lung, small cell lung, pancreatic, and prostate cancers in 2010–2019 with ≥6 months survival and continuous fee-for-service coverage from the linked SEER-Medicare data. Early PC was identified by claims with corresponding diagnosis codes or hospice and palliative medicine provider specialty codes within 90 days post-diagnosis or up to the first hospice admission date (whichever came earlier).2 Treating physicians and corresponding organizations (i.e., Tax Identification Number) were assigned based on the plurality of visits with a cancer diagnosis code within 180 days surrounding cancer diagnosis date. The team described the percentage of patients receiving early PC each year overall and stratified by cancer type. To evaluate the contribution of provider variation in early palliative care use, they first conducted generalized linear probability models with
physician- and organization-fixed effects to estimate the proportion of variation in early PC receipt due to between-physicians/ organizations variation. The association between several observable physician and organization characteristics and early PC receipt was then estimated. All regression models were also controlled for patient sociodemographic and clinical characteristics.
RESULTS
Among 102,060 patients treated by 19,186 unique providers and 8,039 organizations, the percentage receiving early PC increased from 1.4% to 10.3% in 2010–2019. Although statistically significant increases were observed across cancer types, receipt in patients with prostate cancer was relatively lower compared to pancreatic, small cell lung, non-small cell lung, and breast cancers (Table 1). After adjusting for patients’ characteristics, variation in early PC use between treating physicians and organizations explained 48.2% and 32.7% of the total variation, respectively. Among observable physician and organization characteristics, treating physicians’ early PC referral in the past year (6.76 percentage points; 95% CI: 5.54–7.98)
Table 1: Percent of early palliative care receipt among patients with advanced cancers.
and treating organizations’ employment of hospice and PC specialists (3.18 percentage points; 95% CI: 2.59–3.77) were most strongly associated with early PC receipt.
CONCLUSION
Despite considerable growth in early PC receipt, utilization remained low in 2019. The large variation between providers and organizations suggests important modifiable provider behaviours and organizational characteristics in early PC use. In particular,
education to increase awareness and referral to early PC among physicians and efforts to increase hospice and palliative medicine workforce may be effective tools to promote early PC utilization.
References
1. Ferrell BR et al. Integration of palliative care into standard oncology care: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol. 2017;35(1):96-112.
2. Huo J et al. Timing, costs, and survival outcome of specialty palliative care in medicare beneficiaries with metastatic non-small-cell lung cancer. JCO Oncol Pract. 2020;16(12):e1532-42.
Congress Interview
Michael A. Postow has made significant contributions to the landscape of immunotherapy and its applications in combating melanoma. His insights and expertise are highly sought after by medical professionals and researchers alike. He spoke with AMJ during the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting on his groundbreaking work and on ASCO 2024.
Michael A. Postow
Chief of the Melanoma Service at Memorial Sloan Kettering Cancer Center, New York, USA
Q1 Could you share some insights into the groundbreaking research and development process behind FDAapproved therapies for melanoma that your team at Memorial Sloan Kettering Cancer Center (MSK) has contributed to, such as the nivolumab and ipilimumab combination?
a reality. We now need to work on improving the efficacy of these approaches and finding options for patients for whom drugs like nivolumab and ipilimumab do not work, so that everyone can benefit from our melanoma treatments.
Q2
We are only at the beginning of realizing the full potential of cellular therapy for melanoma
Immunotherapy with drugs like nivolumab and ipilimumab has been decades in the making, even long before our group at MSK was involved. The science that laid the foundation for these approaches began with early investigations into how T cells worked, and this then led to testing this approach in mice and ultimately in patients. It is remarkable to have been a part of even one small component of this story (the later phase clinical trials that showed it was very effective in melanoma), and I’m personally grateful for all of the scientists, mentors, and colleagues in the biopharmaceutical industry who helped these treatments become
Your dedication to expanding the portfolio of melanoma treatments is evident. Can you elaborate on any ongoing efforts or future directions you see in the field that excite you the most?
Tumor-infiltrating lymphocyte therapy has been the remarkable advance of 2024 regarding melanoma. This approach involves removing a tumor surgically and then expanding the lymphocytes within the tumor in a laboratory for ultimate re-infusion back into patients to treat the rest of their melanoma. While this approach is difficult and not suitable for every patient, it offers the potential for long-term benefits. While one approach, lifileucel, is now FDA
It’s important to first get to know my patients personally, their families, and what is important to them
approved, we are only at the beginning of realizing the full potential of cellular therapy for melanoma.
Q3 Building trusting relationships with patients seems to be a cornerstone of your practice. How do you approach crafting personalized treatment plans, and how do you ensure patients feel supported throughout their journey?
It’s important to first get to know my patients personally, their families, and what is important to them in life, not just about their melanoma treatment. Once I understand who a person is beyond their diagnosis, then I feel more comfortable recommending a treatment approach and helping patients through their journey. I have met some remarkable people in all walks
of life with so many varied interests; I learn so much from my patients every day.
Q4 What sessions are you most looking forward to attending whilst here at ASCO 2024, and why?
The ASCO Plenary Session is a collection of the most important updates in oncology in 2024. We are fortunate this year to have a melanoma study, called the NADINA study, represented in this session. The NADINA study demonstrated the promise of pre-surgical (neoadjuvant) treatment with the nivolumab and ipilimumab combination over surgery, followed by adjuvant immunotherapy. In combination with other neoadjuvant data, I feel this affirms the role neoadjuvant immunotherapy has in our field
and opens up many future opportunities for further exploration.
Q5 Balancing a demanding professional role with personal interests can be challenging. How do you manage your time effectively between your responsibilities at MSK and your pursuits outside of work?
I have two young children (3 and 5 years old) and a wonderful wife. Every night I’m home, I prioritize reading books to my kids at bedtime, telling them stories, and putting them to sleep. This time helps keep me grounded in the most important aspects of life and enjoying the little moments. No matter how busy life gets, I believe you can always find time for whatever is important.
Syndromes: Putting Anemia Under the Spotlight
Epidemiology of MDS
MDS occurs predominantly in the aging
Up to 90% of patients may have anemia, leading to a significantly increased risk of mortality2
Transfusion burden is associated with a short OS3 Unmet needs in MDS
Symptoms of MDS
Typical presenting symptoms of MDS are generally non-specific and usually differ, depending on the type of cytopenia4,5
Fatigue/weakness
Palpitations
Shortness of breath Pale skin
Chest pains
Burden on Quality of Life Physical Problems
Physical problems
41% of patients with MDS reported moderate or severe mobility issues.6 MDS causes a substantial and persistent functional decrement, partially due to fatigue7
36.1% of patients with MDS reported moderate or severe problems with usual activities (e.g., work, housework, or leisure activities).6 The disease may affect employment, necessitating time off or compromising career opportunities8 Role functioning
Emotional problems
37.9% of patients with MDS reported moderate or severe issues with anxiety/depression.6 Patients often find the emotional impact of MDS more problematic than the physical consequences.
Social functioning
34% of patients receiving blood transfusions felt they were burdening their family.5
Transfusion requirements may disrupt routines and take time away from family and friends8
Abbreviations: AML: acute myeloid leukemia; CCUS: clonal cytopenia of undetermined significance; del: deletion; EB: excess blasts; FISH: fluorescence in situ hybridisation; GI: gastrointestinal; IB: increased blasts; ICC: International Consensus Classification; IPSS-M: Molecular International Prognostic Scoring System; IPSS-R: Revised International Prognostic Scoring System; ITP: idiopathic thrombocytopenic purpura; LB: low blasts; LR: lower-risk; MDS: myelodysplastic syndromes; MLD: multilineage dysplasia; NOS: not otherwise specified; OS: overall survival; QoL: quality of life; RBC: red blood cell; SLD: single-lineage dysplasia; WHO: World Health Organization.
Loss of appetite
Headache Cold extremities
Other symptoms
Fever Prolonged bleeding
Mouth sores Petechiae
Classification9,13-15
MDS, hypoplastic MDS with LB
MDS with LB and isolated 5q del MOS with LB and SF381 mutation*
suspicion of cytopenia
Not included
MDS-NOS with SLD, or with MLD MDS with del(5q)
MDS with mutated SF387 5–9% MDS with IB1
MDS with fibrosis
10–19%
MDS with IB2
MDS with biallelic TP53 inactivation
MDS with EB
Not included
MDS/AML
MDS with mutated TP53
MDS/AML with mutated TP53
Two updated classifications for MDS were developed in 2022: the WH05 and the ICC for Myeloid Neoplasms and Acute Leukaemia, which are overall similar, but with some differences in diagnostic criteria and nomenclatures.9,13
The publication of this infographic was funded by Bristol Myers Squibb. Oncol AMJ. 2024;1[1]:44-45. https://doi.org/10.33590/oncolamj/WKMQ3310.
Date: 07/24
Job code: HE-US-2400517
Diagnostic workup for MDS9,10
Diagnostic workflow
History and physical exam
Peripheral blood count and peripheral blood smear
Screening tests to rule out non-malignant causes
Anemia
Exclude: GI bleeding, cardiac causes, inflammatory causes, and nutritional causes
Specialist referral and additional tests to rule out other non-malignant or malignant causes
• Bone marrow aspiration and biopsy
• Somatic mutation analysis (gene sequencing)
• Cytogenetics (karyotyping, FISH)
• Immunophenatyping (flow cytometry)
Risk stratification
Unexplained cytopenia
SCAN to visit spotlightonanemia.com
MDS Diagnosis Algorithm
The IPSS-R is the most commonly used risk stratification system in MDS, taking into account the degree of cytopenia, proportion of blasts in the bone marrow, and presence of cytogenetic abnormalities.5,16,17
Revised International Prognostic Scoring System (IPSS-R)16
of patients have LR-MDS3
Recently, the IPSS-M was developed, which integrated information from 31 gene mutations in addition to the IPSS-R components.5,17,18
Diagnosis requires a combination of clinical suspicion, laboratory tests, hematologic and morphologic analysis, and cytogenetic and molecular evaluation9,11,12
Minimal prerequisites to establish MDS diagnosis:4,11 ≥1 unexplained cytopenia +
Exclusion of other potential disorders as primary reason for dysplasia/cytopenia
The diagnosis of MDS also requires ≥1 of the following:4
1. ≥10% morphologic dysplasia (with or without an increase in blast cells) in ≥1 of the 3 lineages of hematopoietic cells
2. A blast cell count of 5–19%
3. A specific MDS-associated karyotype, such as del(5q), del(20q), +8, or −7/del(7q)
Treatment goals for anemia in LR-MDS5
Interviews
The AMJ is honored to feature three interviews with distinguished leaders across the field of cancer care.
Aparna Parikh, a prominent figure at Harvard Medical School in Boston and the Director of the Global Cancer Care Program at Massachusetts General Hospital, shares her mission to improve cancer care delivery and outcomes on a global scale with us. Nancy Davidson, the Executive Vice President for Clinical Affairs at Fred Hutchinson Cancer Center in Seattle, Washington, is a renowned expert in breast cancer research and leadership. Finally, Michael Gibson, Director of Translational Research for Esophago-Gastric Cancer at Vanderbilt-Ingram Cancer Center in Nashville, Tennessee shares his aims to develop more effective treatments for esophago-gastric cancer, a challenging and often aggressive cancer type.
Aparna Parikh
Associate Professor, Harvard Medical School, Boston; Director of the Global Cancer Care Program, Massachusetts General Hospital; Director of Colorectal Medical Oncology, Massachusetts General Hospital; Medical Director Young Adult Colorectal Cancer Center, Massachusetts General Hospital, Boston, USA
Q1What led you to pursue a career in gastrointestinal (GI) oncology?
Once I got into fellowship, and started to see a lot of GI patients, I found a tremendous affinity towards this patient population, in terms of diversity of genders, ethnicities, and ages. I also saw a tremendous unmet need in terms of opportunities to advance science. I think, unfortunately, unlike some cancer types, survival in later stage GI cancers, and even in the early stages for some GI cancers, is still quite limited. I found that it was such a privilege to connect with patients and their families; I really appreciated, valued, and recognized the importance of those
relationships during what can be just an awful time for patients. So, it was both the patient population, merged with the opportunity scientifically to hopefully make an impact on improving survival for these hard-to-treat cancers. Finally, I really enjoyed my peers. I think a lot of oncologists are special, but it takes a certain type of person to care for these complex, various sick patients, and I found an affinity for my colleagues who had gone into GI cancers.
Survival in later stage GI cancers, and even in the early stages for some GI cancers, is still quite limited
Q2The incidence of earlyonset colorectal cancer (EO-CRC) is rising globally. What do you believe is driving the increase of colorectal cases in patients under 50? Are there any unique challenges associated with the diagnosis and management of EO-CRC?
CRC is now the leading cause of cancer-related death amongst males aged 20–39 and 40–49. Last year, in the 20–39 group, it was the third leading cause, but now it's the leading cause. This trend is also seen in females as well. The concern is that this may surpass even breast cancer. I think a lot is still yet to be learned to really understand the underpinnings. We don't entirely know what is driving it yet. I think there is some confluence of early exposures, as early as perhaps in utero exposures; changes in weight over time, including in adolescence; the microbiome; and certain dietary and environmental exposures. This trend is happening across the world.
Our group has taken a lot of interest, not only in the research aspect to try to understand these exposures, but in investing in care for these patients, who present
with unique challenges. They're young; some of them are of childbearing age; some have had children, and some are wanting children. They're in the prime time of earning opportunities and careers, both professionally to develop, but also for salary purposes, too. So, this can be a really challenging time for parenting with young kids. It’s that whole spectrum of not just caring for the disease, but caring for all the other aspects of life that are directly impacted by the disease. We are actively trying to work this into our young onset program, to care for these patients holistically and comprehensively, with social worker support, guidance on fertility, and supporting the children, as a few examples. And then in parallel, our team at the Massachusetts General Hospital, Boston, USA, led by Andy Chan, along with Yin Cao from Washington University, Seattle, USA, was awarded a Cancer Grand Challenges grant, for over 25 million USD, to tackle early-onset cancers. This grant will give a particular focus to CRC, not just in the USA, but across the world. I'm leading one of the global aspects of that effort, looking at EO-CRC in India. I think it's great, because there
is investment, and an urgency in really trying to figure out this very unsettling problem.
Q3
As Medical Director for the Young Adult Colorectal Cancer Center at Massachusetts General Hospital (MGH), what is your key mission, and which goals are you currently working towards?
We are getting patients in the center that are diagnosed already, so I think the overall mission eventually would be to try to figure out who is getting EO-CRC, and why, and then screen earlier. I think that a large part of the mission is on the prevention and early detection side. However, for the immediate goals of the center, it's ensuring the best care, which is always in line with trying to achieve more cures, and maintain quality of life. We offer cutting edge approaches across the spectrum of care, including bold surgical approaches, and also studies geared toward survivors. In one of the studies our program is working on currently, we are looking at coffee. There is compelling epidemiological data that coffee can be protective on the gut, have some protective impacts in the liver, and
may actually be protective in terms of colon cancer risk reduction. We're doing a prospective clinical trial, giving an incipient of coffee, and looking at outcomes that may correlate with an improvement in recurrence for cancer.
We have another clinical trial, led by one of our other faculty members, which is looking at giving a patient more comprehensive guides, as well as coaching, through the treatment of rectal cancer. Rectal cancer is much more complex than colon cancer, as it includes multimodal therapy, different side effects, and different fertility issues. So, the goal is caring for the whole aspect of the patients, and being very thoughtful around patients whose disease is metastatic: are there paths towards curing those patients? For earlierstage patients, can we cure more, and can we prevent? And then, for patients who are undergoing treatment, can we make their whole treatment journey a little easier by providing not only the best care, but the best supportive care and survivorship care?
Q4You are an international expert in liquid biopsies, which have emerged as a powerful tool for monitoring tumor recurrence and therapeutic responses. How do you think liquid biopsies have the potential to transform treatment approaches for patients with GI cancers?
This is such an exciting time for liquid biopsies, and I think that the liquid biopsy landscape is only going to continue to grow. I'm certain that ctDNA, and potentially other blood-based analytes, are going to ultimately transform how we're caring for patients. One of the challenges
right now is that the technology is a little ahead of the therapies.
CtDNA is the most powerful prognostic biomarker we have; if ctDNA is detected after a curative intent path, the odds of that cancer coming back are incredibly high, and a better prognostic marker than many of the other prognostic markers we have. The challenge is that we don't yet have the data to know that we can do anything about that, or that earlier intervention actually matters. So, first, you need something to do. Say you have microscopic evidence of recurrence, and you don't see anything on a CT scan, it feels a little bit like a ticking time bomb, that eventually is going to manifest radiographically. But can you actually reverse that recurrence from happening? To reverse that recurrence, there are a few patients whose immune systems seem to take care of it themselves, but you may need to actually give a therapy reverse the recurrence. In many GI cancers, we have very limited therapies still. In CRC, we essentially only have one adjuvant chemotherapy, currently, that is standard of care. We offer a combination, with folinic acid, fluorouracil, and oxaliplatin (FOLFOX); 5-fluorouracil (5-FU); for recurrence prevention. And so, if you know there is recurrence, but don't have anything you can do with that, is that meaningful?
I think liquid biopsies are very empowering for patients, and it's certainly a test that I, after shared decision-making, will offer. At the moment, there's a lot of work that's happening, including some work from our group, partnering with biopharma, and working really closely with a nonprofit called
Science for America. We are trying to come up with a solution for capitalizing on all the testing that is happening, to try to offer therapies for these patients. It’s definitely a prognostic biomarker, but there's still not a lot we can do to reverse cancer recurrence, except for chemotherapy. And so, we're waiting for opportunities for better therapies to reverse recurrence.
Q5MGH has been consistently recognized as one of the best hospitals in the USA. What makes MGH a leader in medical research and patient care? How can other institutions learn from the approach taken at MGH?
This may sound like a generic answer, but it's truly the reason that I came back to MGH after being away: it's the people. The physicians that come to work at MGH provide the absolute best clinical and patient care, and people pride themselves on that. I think we work collaboratively. I'd say probably the majority of places have multidisciplinary discussions and tumor boards, but at MGH, we take it a step beyond tumor boards; for our new patients, and even many of our follow-up patients, if their care requires interfacing with surgery, as well as medical oncology, we will review all the cases with the tumor board and discuss ahead of time. Then, in one visit, the patient meets the entire care team. It’s very patient-centric, so the patient is not having to attend one appointment with a medical oncologist, one appointment with the radiation oncologist, and one appointment with the surgeon. A new patient is getting to meet with all their care team at one time, and we even sometimes do
follow-ups together as well. We're also tied to a general hospital, and being in a general hospital, we have the best cardiologists, infectious disease doctors, and interventional radiologists at our fingertips. Disciplines that can be very important for patients with cancer are excellent within the institution, and we have access to those disciplines. So, I think it's the collaboration, the people, and the access to a general hospital that we're embedded in, and, of course, the research mission as well.
Q6You have a robust clinical trial portfolio, and have been actively involved in the research of novel agents for GI cancers. Are there any projects you are currently working on that you are particularly excited about?
I think in the GI cancer space, with pancreatic cancer and colon cancer, KRAS is clearly a large driver of oncogenesis, of many GI cancers and non-GI cancers as well. Historically, it has been the nut that was impossible to crack. Now that we've made some inroads with KRAS G12C, it's really exciting to see the G12D, pan-RAS, and pan KRAS space evolve. I'm running some of these RAS-based trials on the clinical side, and partnering really closely with my lab-based colleagues to understand treatment response and resistance. I think the ability to do bench-to-bedside, and then bedside-back-to-bench research, is unique.
Besides minimal residual disease, there are emerging vaccines and antibody-drug conjugates that are coming. We also remain committed to try to figure out mechanisms to make immunotherapy work. As
we all know, immunotherapy in CRC has just not worked, except for the microsatellite instability (MSI)-high patients, and so, we are thinking about different strategies. One strategy that I'm excited to see shape out is built on the hypotheses that, when you have liver metastases, the liver microenvironment may be hindering the ability of immunotherapy to work. There may not necessarily be fantastic drugs to overcome that suppressive microenvironment, but can we use other modalities that we have in our toolbox, such as radiation, to eradicate the liver of disease, and get immunotherapy to work? It's still an early hypothesis, but it's the hypothesis that we have started to test and explore.
We published some data on a different dosing of radiation with immunotherapy, and we have another paper coming out soon, with radiation and immunotherapy, albeit a slightly different strategy than ablative radiation. This approach is to treat the liver with radiation, and then do bedside-tobench work around understanding what is happening with the tumor microenvironment when you treat that. Along those lines, there's data showing that you may have activity of immunotherapy in microsatellite stable colon cancer in earlier-stage disease rather than late-stage disease; and again, maybe that's because you don't have metastases, such as liver metastases. We’re working on some ideas, including with partners at Memorial Sloan Kettering Cancer Centre, on looking at immunotherapy in patients with early-stage microsatellite stable disease.
Q7What are the most significant changes you have seen in the field of GI oncology in recent years?
The most recent changes have been the tremendous strides we've made with biomarkers. Even though immunotherapy in MSI-high disease has transformed the landscape, GI oncology is still relatively new to this field transformation. Immunotherapy in patients with metastatic MSIhigh cancers, immunotherapy in early-stage patients, curing patients without any other surgical intervention, and therapies for BRAF V600E and HER2, have all only gained approvals in the last few years. KRAS G12C has not received approval yet, but is included in National Comprehensive Cancer Network (NCCN) guidelines.
What's most exciting to me is that we are starting to make headway around different biomarkeridentified pockets, but we have a lot of work to still do. In the early to mid-2000s, and prior to that, there was just chemo, and then antiVEGF and anti-EGFR therapy came to be. That was it. And then, all of these newer therapies, based on biomarker subgroups, skyrocketed. So that's really incredible to see, especially in patients who are MSIhigh; we're able to cure people. But, I think it's still humbling that these biomarker subsets are small, and the majority of patients don't have biomarkers. And so, what are the therapies that we can bring into the clinic to help this majority of patients? I'm grateful to be in this space, to try to work towards figuring out what those are.
Q8Beyond your clinical and translational research role, you are also passionate about global health. Can you tell us more about the work you do with the Global Cancer Care Program at MGH to address inequities in cancer care, in particular with the Program for Enhanced Training in Cancer (POETIC), your recent initiative to train African oncologists in their home countries?
This is an area that has been a longstanding interest of mine. I think one of the reasons I went into oncology was seeing the tremendous disparities of cancer care in low- and middle-income countries. There are a lot of disparities within the USA, and I'm not undermining those disparities, which are stark and alarming. Disparities are magnified when you are in low- and middle-income countries. We know that in these countries, the burden of disease is tremendous, and mortality, even for curable cancers, is just higher.
We've seen unparalleled progress and pace in high-income countries, and in the USA, we've seen steep declines in mortality for some cancers. We have early detection tests that cost 1,500 USD; we
have immunotherapies; and cervical cancer, for example, can be prevented and cured here. However, in many low- to middleincome countries, it is a cancer that still kills people, even though we have preventive and curative approaches. Because of this, we felt that it was important as a cancer center, and as a hospital, to invest in thinking about global cancer care. We have focused along the pillars of: education, research, and clinical care. On the education end, we are trying to foster bilateral learning and partnerships, including the training program POETIC, with late trainees or early oncologists who are invested in caring for patients, and staying in Africa. We hope we are bringing people that are going to be the African leaders in cancer care and providing them exposure to how we how we care and think about patients here, and some of the newer therapies, even if accessibility is still some time away. The feedback we've had is that the relationships that can be built, and the exposures to care in different models, are quite helpful. So, that's a program that continues.
We are also starting to look at very different clinical trials, which potentially have a lot of importance
and relevance to care in low- and middle-income countries, but are clinical trials that may not happen here. One such example is the idea of giving a lower dose of immunotherapy to try to bring down the cost of treatment; we know that there is some data that you don't need the doses that are currently given. If we can demonstrate prospectively that you don't need the dose that we give here, and you can get by with a lower dose with the same outcomes, it will enable cheaper access to that end, like building clinical trial capacity. But then, ensuring that downstream we actually have access to those drugs, is really important.
So, we were doing some work on capacity building for clinical trials, and partnering with colleagues that are within the Harvard ecosystem. We are also looking at other partners, such as ATOM and Harvard Law School, to see how we can help to support strategies for voluntary licensing and generics. I would say it's learning partnerships, early detection, diagnostic capacity, medicines, and clinical trials that are some of our key areas of focus. All these things keep me up at night, and I feel very lucky to be in this profession.
Nancy Davidson
Executive Vice President for Clinical Affairs, Fred Hutchinson Cancer Center, Seattle, Washington, USA; Professor of Medicine, University of Washington School of Medicine, Seattle, USA.
What led you to pursue a career as a breast cancer oncologist?
I worked in a breast cancer laboratory at the National Cancer Institute (NCI), Bethesda, Maryland, USA, during the summer after my first year in medical school. The lab studied human breast cancer cell lines, which served as remarkably good models for breast cancer in people, and even a second-year medical student could see how this bidirectional investigation could help to advance treatment for people with breast cancer. This experience catalyzed my passion about breast cancer, and my commitment to translational research.
there is a steady improvement in our understanding of cancer biology, and this understanding drives the continual development of new interventions. Second, today’s standard care is a result of yesterday’s clinical trials, and tomorrow’s standard of care will be defined by today’s clinical trials. Finally, we are not finished until access to clinical trials and new standards of care are enjoyed by all. I wanted to be part of the teams that work in all of these areas.
Q3 What do you think other research centers can learn from the approach you and your team have taken at the Fred Hutchinson Cancer Center, Seattle, Washington, USA?
We continue to make progress in cancer care on several fronts, but our results are far from perfect
Q2 You are also heavily involved in developing new standards of care for patients with cancer. What initially sparked your interest in this area?
We continue to make progress in cancer care on several fronts, but our results are far from perfect. I am constantly reminded of three things. First, thanks to an investment in basic science,
At Fred Hutch, we take pride that our center was at the forefront of the development of bone marrow transplant for cancer, and this was only made possible by extraordinary basic science, clinical investigation, and multidisciplinary teamwork. Decades of work, led by E. Donnall Thomas, led to the identification of appropriate patients, and the development
of treatments that maximized antitumor effect and minimized toxicity, especially infection and graft-versus-host disease. Bone marrow transplant is now used around the world, thanks in large part to the research carried out at Fred Hutch. We use these same principles to guide us across all our areas of investigation. The value of this approach was validated yet again by our teams, who were in the vanguard for development of cellular therapy like CAR-T, taking preclinical work into early phase trials in humans, and then commercialization through a startup company. And the principles are crosscutting; Hutch prostate cancer investigators led the discovery that males with metastatic prostate cancer have a higher likelihood of harboring germline mutations in the BRCA genes, which has implications for the treatment selection for the patient, and genetic testing/ screening/prevention strategies for unaffected family members who are found to have germline BRCA mutations through cascade testing.
Q4
You currently have more than 400 international publications to your name for your research in breast cancer. What do you believe to be the current gaps in literature, and which topics merit greater attention?
I have never been part of a publication where I came away thinking that our “mission was accomplished.” Major gaps include how to refine our strategies for risk assessment and prevention, early detection, tailoring treatment, understanding response and resistance to treatment, enhancing survivorship, and disseminating what we know. An exciting area
is how the utilization of new technology of all types can make a positive impact: for example, artificial intelligence (AI) for screening and risk assessment; circulating tumor DNA to monitor tumor burden and evolution; the use of antibody drug conjugates to refine treatment; and refinement of methods to perform surgery, or deliver radiotherapy. And I expect there are areas that we don’t even know about, which are gaps that we have yet to recognize.
Q5 Your research has specifically focused on the role of hormones in breast cancer growth. Are there any developments in this area that you are particularly excited about seeing translated into practice?
I have been so pleased to see how hormone therapy for breast cancer has evolved to be the foundational treatment for females and males of all ages who have hormone-responsive cancers. We have moved away from our belief that chemotherapy is the preferred choice for many of these individuals. I am excited about how our deeper understanding of ways to manipulate the hormonal milieu has led to the development of new agents, like the oral selective estrogen receptor degrading agents and luteinizing hormone-releasing hormone antagonists. Finally, we have learned a lot about treatment resistance and the rational use of combination therapies, allowing us to partner our hormonal therapies with cyclin-dependent kinase 4/6 inhibitors, AKT inhibitors, and more to come, with the goal of improving outcomes with more biologicallybased therapy.
Q6 In the recently published research article you co-authored, entitled ‘Genomic characterisation of hormone receptor-positive breast cancer arising in very young women’, what would you say the key findings were?
I was fortunate to be a part of this study, led by Sherene Loi, which evaluated tumors from premenopausal females who participated in a pivotal trial of optimal adjuvant endocrine therapy. We learned that tumors from females <40 years were more likely to harbor genomic features suggestive of homologous recombination deficiency, PIK3CA mutations with copy number variants, and GATA3 mutations. These poor prognostic features were most common in females <35 years, and least common in those ≥40 years, and were associated with diminished distant recurrencefree interval and survival. In our opinion, this work suggests that there are discrete genomic subtypes in hormone-responsive tumors in premenopausal females that are age-dependent, and associated with different outcomes. Perhaps this knowledge will help us to refine treatment strategies in this setting.
Q7 As an active researcher, where can we expect to see your focus lie in the coming years?
My interest in “all things breast cancer” is undiminished, and I hope to continue collaborative research initiatives of all types. These range from a new basic science study to tackle therapeutic resistance in triple negative breast cancer, by dissecting the intercellular signals shared between the cancer cells
and their neighbors; to participating in a trial of radionuclide imaging, using a novel tracer to determine responsiveness to PARP inhibitors; to large collaborative efforts, such as the studies of the Translational Breast Cancer Consortium (TBCRC), an alliance of 18 breast cancer research groups across the USA, that have united to perform early phase, hypothesis-driven, biospecimen-rich clinical trials in breast cancer. Founded in 2005, we have conducted 64 trials enrolling 6,600 patients to date, but we still have a lot to do. TBCRC investigators also contributed to a project called AURORA US, whose goal is to carry out deep molecular characterization of matched primary and metastatic breast cancer specimens, obtained from patients whose clinical course is known. The goal is to understand molecular underpinnings of metastatic breast cancer to inform new strategies for intervention, and our first findings from a retrospective study were published in 2023. A prospective study is in progress.
Q8
There has been interest from all areas of life science and healthcare towards AI. Where is there room for AI in breast cancer research, and how will the utilization of such technologies accelerate research and development?
As a novice in the field of AI, I look forward to collaborating with knowledgeable individuals who can help us harness its potential to tackle the critical obstacles in cancer research and care. I can certainly help to identify the problems, and I hope the AI experts will have potential solutions that we can study together.
Q9
What are the most significant changes you have seen in the field of breast cancer during your time as a researcher?
I am proud that breast cancer mortality in the USA has dropped by about 40% since 1990, and I like to think I have played a very small role in bringing about that change. It would not be possible to catalog all of the changes, but some key ones are the efforts of surgeons and radiation oncologists to optimize the extent of surgery and radiation needed; the recognition of the underlying genes for certain hereditary breast cancer syndromes; the development and optimization of new systemic therapies, based on our understanding of the molecular subtypes of breast cancer; the welcome focus on survivorship; and the partnership between breast cancer advocates, researchers, and care providers, which has been so powerful in sparking breast cancer awareness, and promoting an investment in research.
Michael Gibson
Director of Translational Research for Esophago-Gastric Cancer, Vanderbilt-Ingram Cancer Center, Vanderbilt University Medical Center, Nashville, Tennessee, USA
Q1 What sparked your interest in aerodigestive cancers?
I enjoy bringing together colleagues in different oncology subspecialties
This started, as it often does with oncologists, with family, or with a personal experience. My grandfather was diagnosed with small cell lung cancer in the early 1980s, when the treatments were rather limited, and somewhat toxic. I was fortunately, or unfortunately, able to see what he went through, which stuck in my mind. When I went off to college at North Carolina State University in Raleigh, USA, I knew I wanted to do something in healthcare, but I didn't know exactly what. So, I majored in biochemistry and microbiology, not having any idea what that really meant. Those majors provided me with the opportunity to work in a lab at the National Institute of Environmental Health Sciences (NIEHS) in Durham, North Carolina, with principal investigator Kenneth Korach, who was a tremendous mentor for me.
When I had to decide whether I would go to graduate school to study cancer biology, or go to medical school, I chose the latter, because I wanted to apply the science to patient care for those with cancer. I trained in internal medicine and medical oncology at the Johns Hopkins Hospital in Baltimore, Maryland, USA, and found my way into aerodigestive medicine because of my mentor there, Arlene Forastiere. I would say she's a rockstar of aerodigestive cancers. I didn't choose this
specialty per se, but I chose her as my mentor because I also enjoyed treating head and neck and esophageal cancers.
Q2 As the director of the Esophageal Cancer Program at the VanderbiltIngram Cancer Center, Nashville, Tennessee, USA, what is your current mission and focus? What can other institutions learn from the approach taken at Vanderbilt?
As mentioned, I learned from Forastiere when I was a junior faculty member at Johns Hopkins. It was a great experience, and I made some close friends and colleagues out of that initial mentoring experience. As I gained more experience over time, and across different institutions, I decided my passion lay in treating esophageal gastric cancer. I was given an opportunity by our Division Director, Jordan Berlin, and our Gastrointestinal Cancer Group Leader, Cathy Eng, to do what I really enjoy. I do think what you need to figure out is what you enjoy. It doesn't mean the job is easy, but it certainly makes it easier to come to work every day, especially if I can surround myself with a team.
The fun part of this work is being a team builder, or a project builder. I enjoy bringing together colleagues in different oncology subspecialties. For this disease, it would include thoracic surgeons, radiation oncologists, and medical oncologists, amongst others. To
get a patient through treatments for cancer requires a much broader team, which will include collaborative practice nurses, physician extenders or advanced practice providers, nutritionists, pain management care, palliative care, psychosocial, and social work. I enjoy being part of a team that has a singular focus, to help our patients with esophageal cancer, and that's the clinical part that drives me. There's also the translational or scientific portion, which can drive discoveries in the underlying treatment for these cancers. We have a connection to a number of laboratory colleagues who help us to do that.
And finally, what advice do we have for other programs? I think, if you build the infrastructure at your own institution, then additional opportunities will come up. In our case, we are able to collaborate with biotech and pharma companies to bring new therapies to our patients through clinical trials. I might add that the default for clinical trials is that it won't work. I'm not saying that medical oncologists are universally negative, of course. Even if the trial does not work, I like to collaborate with colleagues to figure out why,
because that may enable us to do the next study in a better way. Clinical trials really enable you to network and collaborate with people at other institutions.
Our program has done two things. One is working with the National Cancer Institute (NCI)’s clinical trials effort, and the Eastern Cooperative Oncology Group (ECOG). We have a couple of trials that are run through that, and are open across the country at community level, as well as at academic sites. This enables us to accrue patients a little faster, but also to offer our research to those in the community. We also have an international collaboration with Juntendo University in Tokyo, Japan. That's important because the principal investigator over there, Hajime Orita, an esophageal gastric surgeon, is a good friend of mine. We met when we were both in Baltimore, and have continued our work together. This allows us, as an American institution, to see patients with squamous cell cancer (SCC) of the esophagus, which is very rare here in the USA. As the webs and connections are built and woven together, you manage to make progress in your own institution, as well as in other ones.
Q3
Esophageal cancer is an area of your expertise. What are the unique features and challenges associated with its two main histologic types, adenocarcinoma and SCC?
I'm one of the discussants at the American Society of Clinical Oncology (ASCO) Gastrointestinal Cancers symposium, for two studies looking at immunotherapy for SCC of the esophagus. For SCC, that's 90% of all esophageal cancers in the world. The great majority of cancers, in particular outside of Western Europe and the USA, are SCC. So, I feel that any progress in SCC, even if small, is multiplied quite a lot, since there are around 600,000–700,000 cases of SCC of the esophagus worldwide each year. Other things that separate SCC from adenocarcinoma include that SCC is typically in the upper to midesophagus, and these squamous cells are the same as those that cause the majority of head and neck cancers, which is what makes the esophagus a part of the aerodigestive triad.
There are some differences in the way you manage it, and what you do for curative intent. For example,
you can cure SCC of the esophagus that is localized with definitive chemoradiotherapy, without doing surgery. On the other hand, what I think makes my field even more interesting is that the esophagus lives in two ‘worlds’. The upper world is SCC, and the lower is adenocarcinoma. Adenocarcinoma is what you see in the other tubes of the gastrointestinal tract, such as the stomach, pancreas, small bowel, and large bowel. It means that the lower part of the esophagus is not, per se, an aerodigestive cancer; it is more of a gastrointestinal cancer, and so the causes and the treatments are a little bit different. Whereas SCC is usually the result of smoking, alcohol use, and diet, adenocarcinoma is often related to reflux of acid and bile salts, which lead to a precursor lesion called Barrett's esophagus. That provides an opportunity for screening, which may not exist for SCC of the esophagus, since you have a premalignant condition. If you find it before it becomes cancer, you can potentially intervene, and therefore prevent its progression; however, that is easier said than done. Many smart people have tried to figure out how to screen, prevent, and treat
Barrett’s progression to esophageal adenocarcinoma. We haven't found the grand unified theory for that yet, but I do like the fact that I can live in two so-called ‘worlds’, aerodigestive, as well as gastrointestinal. It keeps me challenged.
Q4You recently co-authored a paper entitled, ‘A phase 2 study of neoadjuvant chemotherapy plus durvalumab in resectable locally advanced head and neck squamous cell carcinoma’. Could you tell us more about the emerging role of immune checkpoint blockade for the treatment of head and neck SCC, and how your findings have contributed to the field?
We know immunotherapy is the wave of the current, and the future. We know that immunotherapy works in a disease agnostic way, meaning on pretty much all solid tumors. Immune checkpoint inhibitors are beneficial, but the question, of course, is, how do you use it? Where do you apply it? How can it be safe? How can it improve outcomes? We collaborated on the durvalumab paper with my colleague, Jared Weiss, at the
University of North Carolina at Chapel Hill, USA, so we were a contributing institution, but not the primary institution. Nevertheless, what we tried to do is evaluate one of two ways to treat locally advanced head and neck SCC, with immunotherapy. Generally speaking, there are several ways to treat locally advanced head and neck cancer. You can do something called definitive chemoradiotherapy, where you cure it without cutting it out. This is also known as an organpreserving approach, and laryngeal cancer with voice preservation is the big paradigm there. The other approach would be to incorporate surgery in some shape or form into that collection.
Our study was looking at giving immunochemotherapy before surgery for resectable oral cavity SCC. The idea would be that the preoperative treatment would decrease the pathologic stage of the tumor, and therefore potentially increase survival for those who get chemoimmunotherapy followed by surgery. This is a Phase II study, or a signal-finding study. We don't have a comparative or control arm
for this, so we can't really say if it's better or not, but the control arm would be if there was a Phase III trial of chemotherapy followed by surgery. The intervention of this Phase III single arm study is chemoimmunotherapy followed by surgery. What we found out is that there was an impressive reduction in the staging of these cancers at surgery. In fact, in just a couple of patients, when they were operated on, there was no leftover living cancer in the specimen. The other component of this trial was looking at whether we could modulate the postoperative or adjuvant approach, because all patients with oral cavity cancer that is lymph node positive or at a higher T stage, will get at least adjuvant radiation, or adjuvant radiation plus chemotherapy. We designed this so that if the patients had a certain pathologic response, we could give either less radiation, or radiation plus chemotherapy postoperatively. I think we achieved that.
The other way you could look at immunotherapy for the treatment of head and neck cancer is in the definitive chemoradiation setting. This study was in patients who had surgery as part of their curative intent; but again, there are organ-preserving approaches where you give definitive upfront chemoradiotherapy and you don't operate, but you still cure them. What if we add immunotherapy to the chemoradiation? It appears that in that setting, where you give chemoradiation plus immunotherapy, it doesn't really work. There are some thoughts that maybe radiation suppresses the local immune environment, and blunts the ability of the immunotherapy to kill the cancer.
Q5
A number of biomarkers currently guide treatment decisions for patients with esophageal and gastric cancers. Have there been any recent advances in biomarker identification with the potential to shift the treatment landscape? Are there any research areas that merit greater attention?
The main advantage in the treatment of adenocarcinoma of the esophagus is that we have at least four predictive biomarker targets: HER2, CLDN18.2, FGF receptor β, and PD-L1. What we're trying to figure out is not only whether they work, but also how they work. The challenge is, how do you sequence them and combine them if you have a tumor that has several markers at the same time? I think for now, this is one of the main challenges, especially if you have more than one biomarker expressed in adenocarcinoma of the esophagus.
Q6
There has been interest from all areas of life sciences and healthcare towards artificial intelligence (AI). Do you think there is room for AI in your field, and do you believe AI will accelerate research and development?
I'm a huge novice when it comes to AI, but I do have a couple of things I can say. I have played around with ChatGPT (OpenAI, San Francisco, California, USA). One of our faculty here, Douglas Johnson, put a paper together where he pulled different specific experts, and asked us to provide three different types of questions. One was a yes/no question, one was a multiple choice question, and the other was an open question, like what clinical
trials are available for esophageal cancer. I was very impressed with how correct ChatGPT was in answering these questions.
What I don't know about AI is how it can help me sort through data, like a needle in a haystack. When doing genomic studies, you get so much data, it's hard to get a correlation from one particular part of it. I'd like it to help me with that. I also think we could put in a couple of patient variables for a particular patient we're seeing, and draw up which clinical trial options exist. I wonder if AI could tell me what the next research questions are, and how I should go about answering them; although, if that's the case, I think a lot of us would be looking for other positions. I do think it's going to be a useful thing. To that end, Vanderbilt did put together our own AI that has appropriate firewalls and connections, since we may put some unassociated patient data in there, although nothing identifying, based on the Health Insurance Portability and Accountability Act (HIPAA).
Q7 Where can we see your research and clinical focus lie in the coming years?
I would like to be able to do three things. The first is that, by doing smaller clinical trials in several institutions, we might be able to answer questions more quickly than a big pharma study, because it's very hard for academic centers to do a large Phase III study. If we have specific questions that might not be answerable, for example, microbiome or circulating tumor DNA, that we can do on a smaller scale to collect the data we need, we might be able to answer why it works or doesn't, and then move
We know immunotherapy is the wave of the current, and the future
that forward to a larger venue. So, signal-finding studies at academic institutions will be important. Secondly, I think the identification of new biomarkers is critical. There are many types of biomarkers, some of which are clearly impacting patient care, such as HER2 or PDL1, but there are also biomarkers that can tell you whether a patient has completely responded for curative intent, whether they've recurred and when, and when to start subsequent therapies down the road. Finally, I think doing trials across borders may become more and more important, because underserved areas deserve research and therapies that are available everywhere else, and if we could somehow unify studies, so that we have unified treatment approaches across the world, perhaps that would lead to some more efficiency in further studies and treatment options.
Wearable Devices for Vital Sign Monitoring in Hematology and Oncology Patients: An Integrative Review of Implementation Barriers and Detection Performance
Current hospital vital sign monitoring for hematology and oncology patients relies on intermittent checks, potentially delaying detection of complications. Wearable devices offer continuous monitoring, promising earlier intervention. However, integration of wearable devices requires addressing user acceptance concerns. This integrative review aims to identify and address implementation barriers hindering the successful implementation of wearable devices for vital sign monitoring amongst hematology and oncology patients in acute hospital settings, and evaluate their complication detection performance. Databases such as PubMed, Cochrane, ProQuest, and IEEE Xplore, grey literature from Google Scholar, and handsearching were used to identify articles describing oncology or hematology patients above 18 years old undergoing treatment in a hospital or in-patient setting that used wearable devices for vital sign monitoring, and published from January 1, 2013–September 5, 2023. Eighteen articles fulfilled the eligibility criteria. Whittemore and Knafl's framework guided the review. The selected articles underwent quantitative and qualitative analysis guided by the Unified Theory of Acceptance and Use of Technology framework. High adherence rates inflated user acceptance due to methodological inconsistencies. Challenges in implementation encompassed technical aspects, user-related factors, and compatibility with healthcare system workflow. While wearable devices demonstrated moderate-to-high accuracy in detecting complications, integration with non-wearable device measurements was common. Future directions include understanding healthcare professionals' perspectives, establishing standardized procedures, developing targeted training to optimize integration into clinical workflows, and exploring the feasibility of transitioning to exclusively wearable device data for reliable complication detection. Further research is needed to address implementation barriers and optimize their use in hematology and oncology care.
Key Points
1. Wearable devices offer continuous vital sign monitoring for hospitalized hematology and oncology patients, potentially enabling earlier detection of associated complications. While studies suggest that patients generally accept wearable devices, adherence rates might be inflated due to methodological inconsistencies.
2. Challenges remain in integrating these devices into clinical workflow. These include user comfort, data compatibility with electronic medical records, healthcare professionals' acceptance, and ensuring data accuracy.
3. Further research is needed to standardize protocols for using wearable devices in this setting, explore their effectiveness for monitoring a wider range of common complications, and improve data analysis for clinical reliance on this information.
INTRODUCTION
Traditional vital sign monitoring in acute hospital settings relies on sporadic checks, posing significant challenges for hematological and oncological patients. This monitoring gap leads to delayed identification and treatment of complications like infections, neutropenic fever, sepsis, and cytokine release syndrome (CRS). These complications are more prevalent in immunocompromised patients receiving treatments like chemotherapy, radiation therapy, chimeric antigen receptor T cell (CAR-T) therapy, or stem cell transplants.1-4
Recent advancements in wearable technology can fill this gap by providing real-time, continuous monitoring of vital signs. This enables earlier detection and intervention for complications, thereby improving patient outcomes.5 These devices come in various forms, including adhesive patches that adhere to the skin (e.g., TempTraq®, Blue Spark Technologies Inc., Westlake, Ohio, USA; VitalPatch®, VitalConnect, San Jose, California, USA), biosensors that can be worn on the wrist, bicep, or other areas of the body (e.g., Fitbit, Google, Mountain View, California, USA; Everion, Biovotion AG, Zürich, Switzerland; and Garmin, Garmin Ltd., Olathe, Kansas, USA), and even smartwatches with advanced health monitoring capabilities (e.g., Apple Watch, Apple, Cupertino, California, USA; Microsoft Band, Microsoft, Redmond, Washington, USA). However, successful integration of wearable devices
into the clinical workflow requires overcoming challenges like connectivity issues, alarm fatigue, user acceptance, and sifting through the constant stream of data generated by these devices. Determining what information is clinically relevant and establishing efficient workflows for clinical staff to review these reports are crucial hurdles that need to be addressed.5,6
Several literature reviews have explored the potential applications of wearable devices in an oncology or hematology context, focusing on physical activity or solely on patient adherence.7-9 However, a comprehensive assessment of their specific role in vital sign monitoring, and its impact on hematology and oncology patients, remains elusive. These reviews often overlook the unique challenges faced by this patient population and the applicability of the Unified Theory of Acceptance and Use of Technology (UTAUT) model to successfully integrate wearable devices in this context. Hence, this integrative review aims to identify and address implementation barriers hindering the successful implementation of wearable electronic devices for vital signs monitoring in hematology and oncology patients in acute hospital settings and evaluate their complication detection performance. The findings from this review will guide healthcare professionals, administrators, and policymakers on the optimal use of wearable devices in oncology and hematology in the acute care setting.
METHODS
This integrative review was performed following a five-step framework by Whittmore and Knafl: 1) problem identification, 2) literature search, 3) data evaluation, 4) data analysis, and 5) presentation.10 This integrative review aligns with the guidelines established in the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement.11
Literature Search
A preliminary search of PubMed clinical queries and the Cochrane Database of Systematic Reviews (CDSR) was first conducted using search terms such as “oncology,” “haematology,” “wearable”, and “hospital” or “in-patient”, but no reviews on this specific topic were identified. The gaps in similar systematic reviews were evaluated previously. Adhering to the Peer Review of Electronic Search Strategies (PRESS) checklist, text, and index terms from retrieved articles were refined and applied to all databases and grey literature.12 Published studies between January 1, 2013–September 5, 2023 were searched across accessible electronic databases, namely, PubMed, Cochrane, ProQuest, and IEEE Xplore. Sources of the unpublished studies or grey literature included Google Scholar. Lastly, a manual search was also performed to find key journals related to hematology or oncology, and wearable devices (i.e., Journal of Haematology & Oncology, Cancers Journal [MDPI], Cancer [ACS Journals], Journal of Clinical Oncology, Blood Journal, Journal of Haematology, The Lancet Oncology, JAMA Oncology, BMC Cancer, Supportive Care in Cancer Journal).
Study Selection
After the database search, all the identified records were uploaded to endnote x20, and duplicate articles were removed. Articles were included if they described oncology or hematology patients above 18 years old undergoing treatment in a hospital or in-
patient setting. The wearable device must have been used on real-life hematology or oncology patients for vital sign monitoring. Potential uses of the wearable device, prototypes, and wearable devices not used for vital sign monitoring (e.g., point-of-care testing, cancer detection, physical activity monitoring, sleep quality monitoring) were excluded. Studies conducted exclusively in outpatient settings (e.g., used at home or clinic) were excluded. However, studies involving both in-patient and out-patient use were eligible. Only journal articles published in English between January 1, 2013–September 5, 2023 with full-text available were included. A pilot test was performed by the two reviewers on 10 articles to refine the eligibility criteria. Both reviewers independently screened the titles and abstracts, followed by the full texts, against the eligibility criteria. Disagreements between the reviewers at each stage of the selection process were resolved by reaching a consensus.
Quality Assessment
The Critical Appraisal Skills Programme (CASP) tool and the strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist were used to assess the quality of the included studies.13,14
Data Abstraction
Qualitative data from patient, caregiver, and healthcare professional perspectives on wearable devices and quantitative data on accuracy performance were collected using a data collection form jointly developed by both reviewers, adapted from the JBI methodology guidance for mixed methods review.15 The two independent reviewers pilot-tested the form on five randomly selected articles, and amendments were made before its use. The two reviewers independently charted the data using microsoft excel and discrepancies were resolved through discussions.
Data Analysis
The UTAUT framework guided qualitative data analysis, allowing themes to emerge inductively. This framework comprehensively explores factors influencing wearable technology adoption in hematology and oncology care, including performance expectancy, effort expectancy, social influence, and facilitating conditions.16 Insights into potential barriers and facilitators for integrating wearable devices into clinical practice are revealed.16 Quantitative data was analysed deductively using descriptive statistics. Key findings from both analyses will be presented using tables and figures.
RESULTS
Study Selection
A total of 2,142 articles were identified from four electronic databases, grey literature, and handsearching. After removing 326 duplicate articles using endnote x20, the title and abstracts of 1,816 articles were screened for eligibility. A total of 1,735 articles were excluded as they involved trials of prototypes, did not involve vital signs monitoring, were not conducted in an inpatient setting, or were performed amongst the pediatric population.
This refined the pool to 81 articles, from which full texts were examined against the eligibility criteria. Subsequently, 60 articles were excluded for reasons such as non-primary studies; involving pediatric populations; or live presentations, meeting abstracts, and protocols without specific wearable device details or results. Consequently, 18 articles met the inclusion criteria for the final analysis. The detailed selection process is illustrated in the prisma flow diagram (Supplementary 1).
Study Characteristics
The included studies were primarily observational (n=14), conducted in nonAsian settings (n=14), and featured modest sample sizes (all <105 participants) (Supplementary 2). While the CASP checklist
indicated moderate to high overall quality (Supplementary 3), the strobe checklist (Supplementary 4) revealed areas for improvement in reporting completeness. Notably, limitations in addressing potential bias, justifying sample size, and managing missing data were identified in some studies, potentially impacting the robustness and generalisability of their findings (Supplementary 3; Supplementary 4).
Wearable Device Characteristics
Wearable devices used in the 18 articles may be categorized as adhesive patches, nonadhesive biosensors, and smartwatches. Adhesive patches are distinguished by their adhesive form factor (Healthdot®, Philips, Amsterdam, the Netherlands; TempTraq; and Vitalpatch), whereas non-adhesive biosensors are primarily tailored for health monitoring purposes and lack adhesive properties (Current Health Inc., Edinburgh, UK; Everion; ViPCare SmartBand, Gadgle Creative Technology Co. Ltd., Changhua, Taiwan; Biopatch™ or BioHarness™, Zephyr, San Jose, California, USA; Fitbit Alta HR; Garmin vivosmart® 4; Fitbit Charge 2, and Garmin vivofit®). Smartwatches provide supplementary functionalities beyond health monitoring, including communication features and integration with a synchronized smartphone (Apple Watch, Microsoft Band 2). These wearable devices exhibit variations in features such as data accuracy, battery life, skin irritation risk, ease of use, comfort, monitored parameters, integration with electronic medical records (EMR), cost, and monitoring frequency (Table 1).
Adhesive patches, while user-friendly with extended battery life that requires periodic replacement, tend to have lower data accuracy and have the highest likelihood of causing skin irritation.17-21 Typically employed for short-term monitoring of a single parameter, they represent a cost-effective option and are used frequently for patients undergoing chemotherapy, stem cell transplant, or blood transfusion (Table 1).17-22 Notably, TempTraq is a Food and Drug Administration (FDA)-cleared
Class II medical device,18 while Biopatch is FDA-approved for electrocardiogram sensing.23
Non-adhesive biosensors, a pricier and less user-friendly alternative that requires daily recharging, provide enhanced data accuracy with a reduced risk of skin irritation. Similar to smartwatches, non-adhesive biosensors are used for long-term monitoring of multiple parameters such as post-cancer surgery, stem cell transplant, CAR-T therapy, chemotherapy, and end-of-life care.24-31
Smartwatches, albeit the most expensive and complex to operate, offer extensive functionalities and data integration with EMR. Their interactive interfaces facilitate the administration of pain score questionnaires,
frequently used for patients with sickle cell anemia.32-34 Apple Watch has FDA clearance for detecting atrial fibrillation.35
Currently, only a limited number of devices (Zephyr Biopatch or BioHarness, Fitbit Charge 2, Garmin Vivo, and Apple Watch) offer simultaneous measurement of all five vital signs routinely monitored in hospitals: blood pressure, heart rate, oxygen saturation, temperature, and respiratory rate.
Adapted Unified Theory of Acceptance and Use of Technology Framework
The UTAUT framework posits that four key constructs (performance expectancy, effort expectancy, social influence, and facilitating
Table 1: Recommended wearable devices for hematology/oncology patients by treatment or complications (based on included articles).
Monitoring, Accuracy, Comfort, Integration with Clinical Care Systems Wearable Biosensors or Smartwatches
Ease Of Use
Biosensors
Table 2: Unified Theory of Acceptance and Use of Technology (UTAUT) to explain the successful implementation of wearables.
Factors
Performance and Trust
Patient Empowerment
Patient Perspective
User-related
● Patient’s expectations
● Self-monitoring
Barriers
● Retrospective data analysis limits immediate grasp of benefits
● Anxiety from continuous monitoring
● Caregiver assistance
● Inadequate Training
● Comfort and Wearability
● Limited Technology Literacy
Access and Resource
● Device Complexity
● Limited battery life
● Limited Access to Devices
● Connectivity
● Skin irritation
● Poor device adhesion
● Limited water resistance
● Age
● Increasing symptom burden
● Dependence on smartphones for patientreported symptom entry and Bluetooth connectivity
Recommendation
● Demonstrate tangible benefits to patients
● Future research should focus on real-time detection and intervention
● Minimize false alarms with more refinement of algorithms and data analysis systems
● Reassurance from medical team
● Provide comprehensive training for patients and caregivers to ensure effective device utilization.
● Simplify the user interfaces, minimize patient’s navigation thereby eliminating or significantly reducing the need for training
● Enable customisation to accomodate to patient’s capabilities
● Do not use skin barrier products such as Cavilon to reduce skin irritation
● Develop disposable wearable devices with improved skin compatibility and water resistance
● Easily accessible bedside table charging
● Institution provided paired bedside tablet or smartphone
● Wirelessly send data instead of extraction from internal memory
Technical
Organisational Perspective
● Data Accuracy
● Data Management
Healthcare System and Workflow
● Integration with Clinical Care
● Compatibility issues with electronic health records mandating manual data extraction
● Frequent data download visits due to low data storage
● Data corruption
● Data synchronisation issues
conditions) directly influence behavioral intention and use (Table 2; Supplementary 5).
Performance expectancy refers to the perceived usefulness and benefits of wearable devices for both patients and healthcare professionals. While retrospective data analysis limits the immediate perception of benefits, anxiety from continuous monitoring and technical challenges further diminish the perceived value.17,26 Skin
● Ideally use wearable data transfer (direct access) method by de Arriba-Pérez et al. (2016) (raw data that can deploy open-source algorithm)
● Automate data extraction and analysis using artificial intelligence to reduce manual workload
● Develop new protocols for incorporating wearable data in clinical workflows
● Healthcare provider training
● Future research should focus on:
• Healthcare professionals’ perspective, perceptions and attitudes, exploring how wearable devices can be integrated into existing healthcare workflows
• Assessing the effectiveness of different training and education programs in promoting the adoption and use of wearable devices by healthcare professionals
irritation, poor device adhesion, limited water resistance, and inadequate battery life, contribute to discomfort, prompting some patients to discontinue use.17,19,26,30,31 Intriguingly, despite the presumed higher technological literacy of younger patients with blood disorders, adhesive patches prevail due to shorter-term monitoring needs.
Older patients with malignancies, with a median age exceeding 53 years, grapple
with device operation due to debilitating symptoms, often necessitating caregiver assistance, highlighting the importance of social influence.29,31
Caregivers, despite often being older than 65 years, exhibit proficiency in device operation after proper training. Training for patients and caregivers was noticeably absent in most studies, with only a few providing details on such initiatives.25,31,36
Effort expectancy pertains to the perceived ease of use and convenience, which is intertwined with the facilitating conditions within the healthcare system and workflow. Compatibility issues with EMR necessitating manual data extraction, frequent data download visits due to low data storage, data corruption, inadequate battery life, lack of integration into existing clinical protocols, limited data transparency due to reliance on proprietary platforms, dependence on smartphones for patient-reported symptom entry, and bluetooth connectivity, all contribute to a higher perceived effort.21,25,26 Healthcare professionals often display resistance due to data synchronization problems, lack of training, and difficulties in managing large volumes of data.21,26 Only one article offered perspectives from healthcare professionals on their experience with wearable devices.19 Despite these challenges, articles that reported patient adherence rates surpassed 70% (n=4; Supplementary 2). However, adherence definitions were heterogeneous (Supplementary 2).
Wearable Device Monitoring
Wearable devices monitor patient’s vital signs for complications such as pain, post-operative events, CRS, infection or sepsis, neutropenia, death events, and chronic, psychophysical fatigue in descending order (Supplementary 6).
Wearable Device Performance
Despite limited area-under-curve and accuracy reports (n=9), wearable devices
demonstrated moderate-to-high accuracy (supplementary 6), surpassing intermittent monitoring methods.18,22,28 Van Der Stam et al.21 also found comparable performance to intensive-care-unit monitoring (Supplementary 6). However, wearable device data were often integrated with non-wearable measurements such as patient-reported outcomes and laboratory biomarkers (n=11). Studies that utilized feature selection showed that patientreported outcome measurements were superior predictors of pain, death, and post-operative adverse events than wearable device measurements (Supplementary 6).17,24,31-34
Interestingly, while wearable devices demonstrated superior accuracy in in-patient settings, adherence rates were paradoxically higher among out-patient cohorts (Supplementary 6).27 This discrepancy suggests potential areas for improvement, particularly in enhancing adherence among in-patients, which could consequently lead to further improvements in accuracy levels. Consistent with study definitions, temperature changes remained the primary indicator for CRS, infection, sepsis, and neutropenia (Supplementary 6). Minor variations existed within definitions for the same complication, such as fever threshold for infection and sepsis (Supplementary 6). Despite inherent subjectivity, pain and fatigue were translated into objective, predictable parameters through AI and heart rate analysis.
DISCUSSION
Factors Influencing the Implementation of Wearable Devices
Considerations for user acceptance
High adherence rates across studies might overestimate true acceptance due to methodological inconsistencies. Conducting semi-structured interviews is advocated to elicit a more nuanced and balanced assessment of acceptance.37 However, none of
the studies utilised this method of assessing user acceptance of vital sign wearables. Frequent trial visits and Likert Scale surveys introduce potential bias.18,19,27,37 Echoing observations from Sprogis et al.,37 focusing on withdrawal reasons for user comfort can lead to reporting bias. Similarly, relying solely on adherence rates, with heterogeneous definitions across studies (Supplementary 2) limits reliable comparisons and true understanding of acceptance.38
Task-Technology Fit
Applying the Task-Technology-Fit model (alignment of device and task demands),39 key wearable features were analyzed from the included articles and tailored to patients’ conditions and treatment (Table 3), resulting in a decision tree (Figure 1) for optimal device selection.
Overcoming Implementation Barriers
Beyond device selection, the Task-
Examples HealthDot, TempTraq, VitalPatch
Technology-Fit model guides us towards alleviating implementation barriers (Table 2; Supplementary 5). Given the limitations of retrospective data analysis, future studies should explore real-time feedback systems that will facilitate earlier medical intervention, thereby enhancing patients’ perceived usefulness, and bolstering performance and trust.40 Jacobsen et al.27 demonstrated that treatment success and failure can also be tracked by wearable devices, thereby enhancing healthcare professionals’ perceived usefulness.
Mitigating patient anxiety associated with wearable devices firstly requires continuous refinement of algorithms and data analysis systems to progressively minimize false alarms, fostering trust, and reducing unnecessary distress.41,42 Secondly, proactive reassurance from the medical team is crucial. Patients need to be confident that unexpected device signals will trigger appropriate clinical
Current Health Inc, Everion, ViPCare Gadgletech Zephyr Biopatch/ BioHarness, Fitbit Alta HR, Garmin Vivosmart 4, Fitbit Charge 2, Garmin Vivofit
Microsoft Band 2
Table 3: Wearable device characteristics.
Stem Cell Transplant
CAR-T therapy
escalation and that their concerns will be promptly addressed.41 Training patients and caregivers on device usage can also enhance perceived usefulness and effort expectancy.43 Alternatively, simplifying user interfaces and minimizing navigation can obviate the need for training, particularly advantageous for patients with high symptom burden or low technological literacy.44,45 Skin irritation concerns intuitively suggest the use of skin barrier products, Yet Tonino et al.19 Admonished Cavilon™ as it exacerbates irritation.
To reduce effort expectancy, non-adhesive biosensors and smartwatches should offer bedside charging options and given smartphone dependence, institutional provision of tablets or smartphones should
be considered.46 Presently, the use of warehouse data transfer (indirect access) introduces vulnerabilities, risking data modifications or loss through an intermediary (smartphone application).47 Ideally, embracing wearable data transfer (direct access) would eliminate delays, providing real-time access to raw sensor data and enabling transparent deployment of open-source algorithms without relying on an intermediary device (smartphone). However, practical challenges, such as energy consumption and limited support, hinder its execution.47 Considering the impracticality of adopting wearable data transfer (direct access), the more viable alternative is wearable data transfer (indirect access), where data from wearable devices are transferred to third-party systems
Figure 1: Decision tree for
CAR-T: chimeric antigen receptor T cell.
through an application in an intermediate smartphone. This approach, while not as ideal as direct access, overcomes the practical challenges associated with energy consumption and limited support.47
To further reduce manual workload, data extraction and analysis can be automated with AI.48 Although not explicitly stated, the absence of automatic data extraction may be due to concerns with data security and privacy.49 Therefore, data extraction methods must comply with regulatory standards.50
Limited data storage plagued Jacobsen et al.26 due to their reliance on local storage, while cloud-based storage solutions offered ample storage and enhanced security in other studies.19,20,32,51
Hilty et al.52 identified a notable scarcity of standard operating procedures and healthcare professional training pertaining to the integration of wearable devices into clinical workflows and proposed methods to teach and assess clinical competencies in this aspect.
Performance and Limitations of Wearable Device Monitoring
Although in-patient studies demonstrated high accuracy, Jacobsen et al.26 identified adherence barriers, particularly high symptom burden. Similar to Cheong et al.,53 assessing the diagnostic accuracy of wearable devices remains challenging due to the absence of true positive, false positive, true negative and false negative values; variations in reference tests; and definitions of hematological and oncological complications (Supplementary 6).54 Moreover, only TempTraq is medical-grade, and limited FDA clearances raise concerns about clinical dependability.18,23,35,55
Traditionally, vital signs such as temperature, heart rate, and blood pressure have been recognized as pivotal indicators of CRS, and infection or sepsis.56,57 However, due to the wearable device's limited capability to measure solely temperature,
only temperature measurements were employed for detecting these complications alongside non-wearable measurements. This constraint prompts a critical inquiry; whether the reliance on a singular parameter signifies a limitation, thereby suggesting a potential imperative to integrate additional physiological measurements from wearable devices to augment accuracy, or alternatively, a single vital sign may suffice. Subsequent research should delve into comparing the effectiveness of using only temperature versus a combination of vital signs for comprehensive detection of hematological or oncological complications.
Complications commonly experienced by hematology and oncology patients, such as nausea or vomiting, graft-versus-host disease, chemotherapy-induced peripheral neuropathy, neurotoxicity, anemia, and bleeding, remained unexamined. While measuring subjective symptoms like rash and diarrhea presents difficulties, encouraging developments exist. BioIntelliSense, Denver, Colorado, USA, demonstrates the potential for tracking vomiting, while Mantovani et al.60 shows promise in monitoring chemotherapyinduced peripheral neuropathy through gait and balance analysis from wearable devices.59,60 This opens the door for ongoing clinical assessments and trend analysis, paving the way for artificial intelligence-based monitoring.61
Nonetheless, the included articles predominantly relied on non-wearable measurements, particularly for subjective complications like pain and fatigue. Despite existing literature associating heart rate variability and blood pressure to pain aided by machine learning, and establishing links between heart rate variability and respiratory rate with fatigue, patients’ self-assessment remains the gold standard.62-64 The included articles used visual analogue scale for self-reported pain assessment.65 However, assessing non-communicative patients and accounting for memory, cognitive, and social desirability biases pose challenges.65,66 Therefore, transitioning pain assessment
to measurable parameters, especially for hematology and oncology patients with high symptom burden, or nearing the end of life, who may be non-communicative, still needs to be explored.67 Further research is essential before completely replacing non-wearable measurements with solely wearable device data, particularly for developing artificial intelligence analysis models.62
Future Directions
Implementing wearable devices in hematology and oncology requires a multipronged approach. Tailored device selection based on individual needs, standardized procedures, and comprehensive training are key. Research must address implementation challenges, expand complication detection, and develop real-time feedback systems. Transitioning to objective pain and fatigue assessment using wearable device data and understanding healthcare professional perspectives are crucial next steps. Additionally, future studies should explore the cost-effectiveness of implementing wearable devices in these settings, considering not only device costs but also potential savings from earlier intervention and reduced hospital stays.
References
1. Hoffman R et al. (eds.), Hematology: basic principles and practice (2022) 8th edition, Elsevier.
2. Los-Arcos I et al. Recommendations for screening, monitoring, prevention, and prophylaxis of infections in adult and pediatric patients receiving CAR T-cell therapy: a position paper. Infection, 2021; 49(2):215-31.
3. Maschmeyer, G et al. Infections associated with immunotherapeutic and molecular targeted agents in hematology and oncology. A position paper by the European Conference on Infections in Leukemia (ECIL). Leukemia. 2019;33(4):844-62.
4. Braga C et al. Clinical implications of febrile neutropenia guidelines in the cancer patient population. J Oncol Pract, 2019;15(1):25.
5. Joshi M et al. Wearable sensors
Limitations
The generalizability of the findings may be limited due to study characteristics. Restricted access to subscription-based databases may have imposed limitations on data acquisition.
CONCLUSION
High patient adherence suggests general acceptance of wearable devices in hematology and oncology care, but methodological variations across studies warrant caution in interpretation. Tailoring device selection to patient conditions and treatments is recommended. Challenges in implementation, including technical and user-related issues, underscore the need for further research and targeted interventions. While wearable devices demonstrate high accuracy, challenges in direct accuracy comparisons hinder comprehensive assessment. The predominant use of nonwearable measurements, aided by AI, highlights the complexity of transitioning to solely wearable device-based assessments. Complications common among these patients are underexplored, indicating a need for future investigation.
to improve detection of patient deterioration. Expert Rev Med Devices. 2019;16(2):145-54.
6. Rosman L et al. When smartwatches contribute to health anxiety in patients with atrial fibrillation. Cardiovasc Digit Health J. 2020;1(1):9.
7. Chow R et al. The use of wearable devices in oncology patients: a systematic review. Oncologist. 2024;9(4):e419-30.
8. Kos M et al. The association between wearable activity monitor metrics and performance status in oncology: a systematic review. Supp Care Cancer. 2021;29(11): 7085–99.
9. Beauchamp U et al. The use of wearables in clinical trials during cancer treatment: systematic review. JMIR Mhealth Uhealth. 2020;8(11): e22006.
10. Whittemore R, Knafl K. The integrative review: updated methodology. J Adv Nurs. 2005;52(5):546-53.
11. Liberati A et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. 2009;151(4): W-65.
12. McGowan J et al. PRESS peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40-6.
13. Critical Appraisal Skills Programme. CASP cohort study checklist. https:// casp-uk.net/checklists/casp-cohortstudies-checklist-fillable.pdf. Last accessed:1st September 2023.
14. Cuschieri S. The STROBE guidelines. Saudi J Anaesth. 2019;13(Suppl 1):S31.
15. Pearson A et al. Methodology for JBI mixed methods systematic reviews. Joanna Briggs Institute Rev Man. 2014; 1:5-34.
16. Binyamin SS, Hoque MR. Understanding the drivers of wearable health monitoring technology: an extension of the unified theory of acceptance and use of technology. Sustain Sci. 2020;12(22):9605.
17. Buchan C et al. Early warning of infection in patients undergoing hematopoietic stem cell transplantation using heart rate variability and serum biomarkers. Transplant Cell Ther. 2022;28(3):166-e1.
18. Dambrosio N et al. Continuous temperature monitoring for earlier fever detection in neutropenic patients: patient's acceptance and comparison with standard of care. Biol Blood Marrow Transplant. 2018;24(3): S108-9.
19. Tonino R et al. Remote patient monitoring in adults receiving transfusion or infusion for hematological disorders using the VitalPatch and accelerateIQ monitoring system: quantitative feasibility study. JMIR Hum Factors. 2019;6(4):e15103.
20. Van Der Stam J et al. Accuracy of vital parameters measured by a wearable patch following major abdominal cancer surgery. Eur J Surg Oncol. 2022;48(4):917-23.
21. TJ et al. A wearable patch based remote early warning score (REWS) in major abdominal cancer surgery patients. Eur J Surg Oncol. 2023;49(1):278-84.
22. Flora C et al. High-frequency temperature monitoring for early detection of febrile adverse events in patients with cancer. Cancer Cell. 2021;39(9):1167-8.
23. Lo J et al. Measuring mental workload with low-cost and wearable sensors: Insights into the accuracy, obtrusiveness, and research usability of three instruments. J Cogn Eng Decis Mak. 2017;11(4):323–36.
24. Barber E et al. Feasibility and prediction of adverse events in a postoperative monitoring program of patient-reported outcomes and a wearable device among gynecologic oncology patients. JCO Clin Cancer Inform. 2022;6(1): e2100167.
25. Slade A et al. Feasibility of wearable activity trackers in cystectomy patients to monitor for postoperative complications. Curr Urol. 2021;15(4):209.
26. Jacobsen M et al. Feasibility of wearable-based remote monitoring in patients during intensive treatment for aggressive hematologic malignancies. JCO Clin Cancer Inform. 2022;6:e2100126.
27. Jacobsen M et al. Wearable based monitoring and self-supervised contrastive learning detect clinical
complications during treatment of hematologic malignancies. NPJ Digit Med. 2023;6(1):105.
28. Rajeeve et al. Early detection of CRS after CAR-T therapy using wearable monitoring devices: Preliminary results in relapsed/refractory multiple myeloma (RRMM). JCO. 2021;41(16):e13626.
29. Shih et al. Measurement of cancerrelated fatigue based on heart rate variability: observational study. J Med Internet Res. 2023;23(7):e25791.
30. Sugiyama Y et al. Effectiveness of continuous monitoring by activity tracker of patients undergoing chemotherapy for urothelial carcinoma. Cancer Treat Res Commun. 2020;25:100245.
31. Liu J et al. Evaluating the potential of machine learning and wearable devices in end-of-life care in predicting 7-day death events among patients with terminal cancer: cohort study. J Med Internet Res. 2023;25:e47366.
32. Johnson A et al. Use of mobile health apps and wearable technology to assess changes and predict pain during treatment of acute pain in sickle cell disease: feasibility study. JMIR Mhealth Uhealth. 2019;7(12):e13671.
33. Stojancic R et al. Predicting pain in people with sickle cell disease in the day hospital using the commercial wearable apple watch: feasibility study. JMIR Form Res. 2023;7:e45355.
34. Vuong C et al. Monitoring and predicting pain in patients living with sickle cell disease using the apple watch-inpatient and outpatient. Blood. 2022;140(Suppl 1):2578-9.
35. Raja J et al. Apple Watch, wearables, and heart rhythm: where do we stand? Ann Transl Med. 2019;7(17):417
36. Oliveira et al. Biometrics and quality of life of lymphoma patients: a longitudinal mixed-model approach. Expert Systems. 2020;38(4):e12640.
37. Sprogis S et al. Patient acceptability of wearable vital sign monitoring technologies in the acute care setting: systematic review. J Clin Nurs. 2019;28(15-16):2732-44.
38. Chan A et al. Reporting adherence, validity and physical activity measures of wearable activity trackers in medical research: A systematic review. Int J Med Inform. 2022;160:104696.
39. Spies R et al. A scoping review of the application of the task-technology fit theory. Responsible design, implementation and use of Information and communication technology. 2020; 12066:397-408.
40. Chau K et al. Smart technology for healthcare: exploring the antecedents of adoption intention of healthcare wearable technology. Health Psychol Res. 2019;7(1):8099.
41. Areia C et al. The impact of wearable continuous vital sign monitoring on deterioration detection and clinical outcomes in hospitalised patients: a systematic review and meta-analysis. Crit Care. 2021;25(1):351.
42. Fernandes C et al. Detecting false alarms by analyzing alarm-context information: algorithm development and validation. JMIR Med Inform. 2020;8(5):e15407.
43. Almathami H et al. Barriers and facilitators that influence telemedicinebased, real-time, online consultation at patients' homes: systematic literature review. J Med Internet Res. 2020;22(2):e16407.
44. Guisado-Fernández E, et al. Factors influencing the adoption of smart health technologies for people with dementia and their informal caregivers: scoping review and design framework. JMIR Aging. 201;2(1):e12192.
45. Lewis J et al. Designing wearable technology for an aging population. ergonomics in design. 2017;25(3):4-10.
46. Vink S et al. An exploration of the association between inpatient access to tablets and patient satisfaction with hospital care. Perspect Health Inf Manag. 2019;16(Fall):1i.
47. de Arriba-Pérez F et al. Collection and processing of data from wrist wearable devices in heterogeneous and multipleuser scenarios. Sensors (Basel). 2016;16(9):1538.
48. Nurmi J, Lohan E. Systematic review on machine-learning algorithms used in wearable-based eHealth data analysis. IEEE Access. 2021;9:112221-35.
49. Dinh-Le C et al. Wearable health technology and electronic health record integration: scoping review and future directions. JMIR Mhealth Uhealth. 2019;7(9):e12861.
50. Barua A et al. Security and privacy threats for bluetooth low energy in iot and wearable devices: A comprehensive survey. IEEE Open Journal of the Communications Society. 2022;3:251281.
51. Vijayan V et al. Review of wearable devices and data collection considerations for connected health. Sensors (Basel). 2021;21(16):5589.
52. Hilty D et al. Sensor, wearable, and remote patient monitoring competencies for clinical care and training: scoping
review. J Technol Behav Sci. 2021;6(2):252-77.
53. Cheong S et al. Wearable technology for early detection of COVID-19: a systematic scoping review. Prev Med. 2022; 162:107170.
54. Lee DW et al. ASTCT consensusgrading for Cytokine Release Syndrome and neurologic toxicity associated with Immune Effector Cells. Biol Blood Marrow Transplant. 2019;25(4);625-38.
55. Radin J et al. The hopes and hazards of using personal health technologies in the diagnosis and prognosis of infections. Lancet Digit Health. 2021;3(7):e455-61.
56. Shimabukuro-Vornhagen A et al. Cytokine release syndrome. J Immunother Cancer. 2018;6(1):56.
57. Mitra A, Ashraf K. Sepsis prediction and vital signs ranking in intensive care unit patients. arXiv preprint arXiv:1812.06686. 2018.
58. Mitra A, Ashraf K. Sepsis prediction
and vital signs ranking in intensive care unit patients. arXiv preprint: https://doi. org/10.48550/arXiv.1812.06686
59. Islam R et al. Automatic detection and prediction of cybersickness severity using deep neural networks from user’s physiological signals. 2020 IEEE International Symposium on Mixed and Augmented Reality (ISMAR) Proceedings preprint: http://dx.doi.org/10.13140/ RG.2.2.18275.99366
60. Mantovani E et al. Wearables, sensors, and smart devices for the detection and monitoring of chemotherapy-induced peripheral neurotoxicity: Systematic review and directions for future research. J Peripher Nerv Syst. 2022;27(4):23858.
61. Liao Y et al. The future of wearable technologies and remote monitoring in health care. Am Soc Clin Oncol Educ Book. 2019;39:115-21.
62. Leroux A, et al. Wearable devices:
current status and opportunities in pain assessment and management. Digit Biomark. 2021;5(1):89-102.
63. Yang F et al. Improving pain management in patients with sickle cell disease from physiological measures using machine learning techniques. Smart Health (Amst). 2018;7-8:48-59.
64. Luo H et al. Assessment of fatigue using wearable sensors: a pilot study. Digit Biomark. 2020;4(Suppl 1):59-72.
65. Gélinas C. Pain assessment in the critically ill adult: Recent evidence and new trends. Intensive Crit Care Nurs. 2016;34:1-11.
66. Booker S, Haedtke C. Assessing pain in nonverbal older adults. Nursing. 2016;46(5):66-9.
67. Ebert R et al. Hematologic malignancies patients face high symptom burden and are lately referred to palliative consultation: analysis of a single center experience. Am J Hosp Palliat Care. 2023;40(7):761-4.
Recall Laterality and Bilaterality: Possible New Screening Mammography Quality Metrics
Authors: *Samson Munn,1 Virginia Huynh Kim,1,2 Joanna Huijia Chen,1,3 Sean Maldonado Ramirez,1,4 Michelle Kim,1 Paul Koscheski,1 Babak N. Kalantari,1 Gregory Eckel,1 Albert Lee1
1. Department of Radiology, Harbor-UCLA Medical Center, Torrance, California, USA
2. Department of Radiology, Kaiser Permanente Medical Center, San Leandro, California, USA
3. Bay Imaging Consultants Medical Group, Walnut Creek, California, USA
4. Department of Radiology, Holy Cross Health, Fort Lauderdale, Florida, USA *Correspondence to samsonmunn@pm.me
Disclosure: Munn has a patent issued for a method and system for evaluating the performance of a reader of screening mammograms (patent 11,037,086). The authors declare no other conflicts of interest.
Received: 26.02.2024
Accepted: 13.06.2024
Keywords: Audit, breast cancer, Breast Imaging-Reporting and Data System (BI-RADS), mammography, Mammography Quality Standards Act (MQSA), screening quality.
Purpose: Current screening mammography quality metrics are important and helpful, but do not address all quality concerns. An individual screening mammography reader may be systematically insensitive to findings present in the breast of one side, laterality bias, evidenced by left versus right difference in advised immediate recalls. Current metrics are not designed to detect laterality bias. Whether a reader exhibits laterality bias, or what an appropriate ratio/range of bilateral versus unilateral recalls should be, have never been discussed in medical literature.
Methods: As a trainee quality project, five attending (‘consultant’ in Europe) radiologists’ screening mammography reports over 2 years at an academically affiliated, public hospital were tallied with regard to laterality of recommended recall, and with respect to unilateral versus bilateral recalls advised. The chi-square (χ²) statistic was applied to reports advising unilateral recall.
Findings: No group laterality bias was discovered. One radiologist (the most experienced) evidenced a consistent laterality bias over 2 years (p=0.07) against left-breast findings. Of reports recommending recall, the radiologists’ single-year range for recall regarding both breasts was 10.2–23.3%; for both years combined, the individual radiologists ranged from 13.6–17.9%. The group, 2-year mean recommending bilateral recall was 16.5%.
Conclusion: A radiologist may exhibit laterality bias, favoring detection of findings in one
breast over the other, a concern never before considered. Audit to discern such bias leads simultaneously to assessment of bilateral recall bias. Possible causes of these biases are discussed, and research regarding them as possible quality metrics is encouraged.
Key Points
1. Laterality bias: There is no known, prior medical literature regarding whether a reader of screening mammograms might render interpretations with bias toward detection of findings on one side (left versus right). In a simple audit of mammogram reports made by five radiologists over 2 years, a strong, unexpected likelihood that one of them exhibited laterality bias was discovered.
2. Bilaterality bias: In screening mammogram reports that recommend recall of patients for further assessment, a tendency for those recommendations to be of both breasts rather than simply one may be termed bilaterality bias. Laterality and bilaterality biases may coexist.
3. Screening mammography quality metrics: How far a reader's unilateral recall recommendations may appropriately diverge from 50–50 (reflecting laterality bias), and how small the fraction of recall recommendations for further assessment of both breasts should be (reflecting bilaterality bias), have the potential to become meaningful, practical, and easily audited new quality metrics in screening mammography.
INTRODUCTION
Quality is important in breast imaging, and there exist a number of excellent screening mammography quality metrics to audit readers and mammography programs.1,2 Even commercially available software programs used in mammography reporting include the capability to apply metrics.3 Although highly useful, current metrics do not account for all performance variations, nor does any single metric assess the entire screening episode.4 Thus, there may be potential benefit in additional quality metrics.
Often, a screening mammogram report includes a recommendation for the patient to return for additional imaging. These are termed 'recall' or 'call-back' examinations. One commonly utilized metric of quality is the recall rate: the proportion of screening mammogram reports that are positive. The recall rate in the Breast Imaging Reporting and Data System (BI-RADS)5 is calculated as the total of BI-RADS 0, 3, 4 and 5 reports divided by the number of screening exams reported.6,7 However, as a practical matter, screening mammograms are essentially never
given BI-RADS categorizations of 3, 4 or 5; so, that recall rate effectively becomes reflected by BI-RADS 0 categorizations, which refer to recommendations to obtain additional imaging or prior exams with which to compare soon.
Two potential metrics had years earlier been conceived by one of the authors: A) whether a screening mammogram reader might be biased in terms of laterality, and B) among recalls advised, whether the unilateral versus bilateral proportion is appropriate (herein termed bilaterality bias). There is no Englishlanguage medical literature regarding what portion of screening recalls should be bilateral, nor how much unilateral recalls may diverge with quality from 50–50, left–right. If such biases were to exist, their early detection could be beneficial toward identifying the underlying cause and its remediation, as quality improvement measures.
Therefore, as a trainee quality preliminary project, radiology residents simply tallied these in the authors’ department, as reflected in BI-RADS 0 reports. The aim of the tally was to discover if such bias existed in the authors’ department of radiology.
METHODS
A simple, observational, retrospective tally was done of bilateral, screening mammogram BI-RADS 0 interpretations made by five attending radiologists at the authors’ academically affiliated, public (county), general hospital, from September 1st 2015–August 31st 2016, and from September 1st 2016–August 31st 2017: total reports, number advising recall, unilateral recalls advised for each breast, and bilateral recalls advised. The chi-square (χ²) statistic was applied to unilateral recall reports, regarding left versus right breasts. The χ² statistic is appropriate to assess whether the difference from exactly 50% is one which may reasonably be expected simply randomly; in other words, how often such difference would likely be due to genuine bias (of some sort) versus simple, statistical randomness. All mammograms of the tallied reports had been screening, bilateral, and digital, and had included two routine complementary views per breast (mediolateral oblique and craniocaudal); none had included tomosynthesis. Since report validity was not being audited, mammogram images were not accessed, viewed nor correlated with the reports. The hospital is large (550 beds) and has its own, fully accredited, radiologist training program, and also trains one ‘fellow’ (already a board-certified radiologist) per year in the subspecialty of breast imaging, including mammography. There were five consultant, specialist radiologists who trained the residents and fellow in breast imaging. One radiologist had over 40 years of experience in breast imaging, including some years heading the Breast Imaging Division of the Department of Radiology; since that experience began before breast imaging fellowships were common, that radiologist was not fellowship-trained. The remaining four radiologists were all fellowship-trained in breast imaging, one 6 months, two 12 months, and one 17 months, and their postfellowship breast imaging experience varied from 2–9 years prior to the audit period. Each radiologist met all the requirements of the Mammography Quality Standards Act8
before, during, and immediately after the audit period, including having “interpreted or multi-read at least 960 mammographic examinations” (screening plus diagnostic) each 24 months. Finally, mammography at the hospital was accredited by the American College of Radiology (ACR), including with regard to the five consultant, specialist mammography radiologists.
Although not required, informed consent was obtained from the four radiologists alive when this work was done, and from the next-of-kin of the one radiologist who had since died. Informed consent and ethical approval at the authors’ hospital were not required because this work was a simple retrospective tally exclusively of report categorizations, was a means for radiologist trainees to satisfy a training program requirement in quality assessment and/or improvement, did not entail an intervention nor clinical trial, did not entail patients themselves nor access to their mammogram images, did not assess the clinical accuracy of mammogram reports, did not record patient-identifying data, and did not meet the criteria of the official USA governmental definition of “human studies research”,9 at a minimum because it was not intended to be “generalizable” (i.e., to be disseminated) when it was conducted. Since it was, by definition, not human studies research, human ‘subjects’ were therefore not involved. For such simple radiology residency trainee projects that do not involve patients nor their images, and in which data are not recorded in identifiable fashion, institutional review board submission and ethical approval are generally not required in USA radiology training programs.
RESULTS
Over the 2 years, a total of 4,771 screening mammogram reports were audited. The data regarding reports by the radiologists as a group are in Table 1. Group sidedness disparity was not significant: the lowest group p-value Years 1, 2, and 1+2 was >0.40. Of interpretations recommending recall, the
Total Number of Screening Mammogram Reports Screening reports advising recall (recall rate)
Screening Reports Advising Recall (Recall Rate) (%) Of Screening Reports Advising Recall, Those for One Breast (%) Of Screening Reports Advising Unilateral Recall, Those for the Right Breast (%)
Of Screening Reports Advising Unilateral Recall, Those for the Left Breast (%)
Mean (Median) Number of Screening Mammogram Reports Per Radiologist, Per Year
p = 0.61 Years 1+2 4,771
2-year group mean recommending bilateral recall was 16.5%. The results regarding the individual radiologists’ reports are in Table 2 Regarding four of the radiologists, the lowest (most significant) single-year p-value was 0.42; it was likewise high (i.e., insignificant) for the combined 2 years at 0.60. In contrast, the unilateral recall reports of the remaining radiologist (#3 in Table 2) disproportionately concerned the right breast (p=0.07), suggesting unilateral bias. This radiologist was the most experienced, interpreted the largest number of exams each year, and had the lowest overall recall rate. Of reports advising recall, the radiologists’ individual, bilateral recall ranges were 13.2–23.3% (13.3–23.3% excluding the one radiologist with apparent laterality bias), 10.2–22.5%, and 13.6–17.9%, for Years 1, 2, and 1+2, respectively. The whole-group, 2-year mean recommending bilateral recall was 16.5% (16.1% excluding the one radiologist with apparent laterality bias).
DISCUSSION
The exclusive intent of this tally was practical and simple: to discover by solely counting screening mammography reports if there might exist laterality bias in screening mammogram reports in the authors’ radiology department. Thus, patient images, patient outcomes, report validity, finding-type, and radiologist confidence levels were not considered. This audit’s nature was preliminary: to gather data; there was no intervention intended nor employed.
For any group of exams interpreted, over any substantial period of time, it is unlikely that left versus right findings will lead to recall precisely 50.00% equally, left versus right; there will nearly always be a small, arithmetic side-discrepancy. Overall, the laterality data did not reveal a concern until drilling down to individual readers.
A consistent bias against one side in recall was evidenced by just one of the five
radiologists: 79.0% likely (by χ²) not to be random for Year 1, 81.0% for Year 2, and 93.0% for Years 1+2. The bias was against the same side (left) each year. This radiologist also had the smallest recall fraction (15.49%), fully one-quarter lower than the radiologist with the next lowest recall portion (20.68%). It is tempting to speculate that part of the gap in recall fraction reflected left-sided findings that went undetected by the radiologist of concern.
None of the other four radiologists had disparity likelihoods as great. The χ² statistic indicated that the highest single-year likelihood that any one of their observed disparities was genuine bias was just 58%. The highest 2-year value was merely 40%. Furthermore, by chance in this small group, it so happened that each of these other four radiologists demonstrated a small discrepancy favoring one side one year, and the other side the other year, unlike the radiologist of concern.
Many studies have demonstrated a higher frequency of breast cancer on the left, while others not. Attempts to explain left-sided predominance have consistently failed. If genuine, such predominance may apply only in certain racial or ethnic groups, and the extent is, in any event, slight.10 Furthermore, the laterality bias detected in the concerning radiologist was against the left side.
Certainly, based simply on this single radiologist in the authors’ small volume practice, they do not propose that many radiologists share the same bias. On the other hand, it is possible that a small percentage of radiologists may; if so, quality improvement warrants identifying who they are in audit. Moreover, this early finding may be the basis to evaluate the matter: to research a large number of radiologists in a high-volume practice or group of practices.
An exhaustive, English-language, literature search failed to discover any discussion regarding what portion of screening recalls should be bilateral, nor how much unilateral
recalls may appropriately diverge from 50–50, left–right, nor if there may exist laterality bias in any particular radiologist or group of radiologists. Only one, merely tangentially related study was found.11 The authors’ intention was to discover if the “excess of left-sided breast cancers” is due to detection being more common on the left by radiologists. In contradistinction to the current work, that study was experimental in design, cancer-enriched test cases were shown to eight radiologists (three not mammogram readers at the time), imagecorrelation was done to assess report validity, recalls were based only on microcalcifications (excluding masses, asymmetries, and areas of architectural distortion), and the bilateral recall fraction was not reported nor could it be gleaned from the reported data.
That study “did not detect any left- or right-sided bias in perceptual detection of microcalcifications in the reader group.” It is unclear whether that was in reference to the reader group as a whole or to individuals within the group.
Laterality bias would not necessarily be expected to be detected by current metrics. A laterality bias necessary to place an individual outside the benchmarks of existing quality metrics would have to be great. Even if the fraction of radiologists who exhibit laterality bias is small, not affecting group statistics significantly, detection of individuals would be helpful toward increasing their awareness and subsequent quality. Focusing on individuals would allow bias to be discovered when earlier or mild, raising consciousness. Once detected, the cause may be investigated, discerned, and remediated.
To the authors’ knowledge, visual acuity and visual field detection are not routinely tested in radiologists in most (if not all) countries. It is tempting to speculate whether there might have been a visual field deficit or perhaps decreased range of cervical motion related to degenerative change. Many factors may conceivably affect laterality bias, including (but not limited to) display arrangement,
reflections, background lighting (apart from reflections), hanging protocol, reader position in relation to others and to displays, visual field deficits, unilateral chronic neck pain, and decreased range of neck motion.
In the authors’ small-volume, high-positivity or high recall-rate practice, they found the portion of screening bilateral recalls to be 16.5% (16.1% excluding the radiologist with possible laterality bias). The authors speculate that less confident radiologists may display a higher percentage than others; they did not assess radiologist confidence level. Since there may be a relationship between experience and confidence, more experienced radiologists might be expected also to display a lower bilateral percentage; that was not the case in this small-volume audit. Also, a higher bilateral percentage may be appropriate in a practice in which patients more often have had no prior mammogram, or the prior mammogram had been long ago. The authors propose that a range should be established, anticipating that that range might include 16%; for example, perhaps it may prove to be 10–20%.
Limitations of this analysis include the small number of radiologists considered and the relatively small volume practice. A study with a very large number of radiologists could help to confirm the existence of laterality bias in other radiologists and to set benchmarks for the proposed metrics.
A study with very large numbers of mammograms and of radiologists would also increase statistical power. In that regard, an alpha of 0.05 is usually utilized in medical statistics as the threshold of significance: if the p-value is less than the chosen alpha, the result is arbitrarily labelled ‘significant’. As professional, medical statisticians remind us, “Many current research articles specify an alpha of 0.05 for their significance level. It cannot be stated strongly enough that there is nothing special, mathematical, or certain about picking an alpha of 0.05.”12 Setting the alpha at 0.05, albeit common, is wholly arbitrary. True findings may exist at a p-value
of 0.08, and false findings may exist at a p-value of 0.02. Hence, the value of research to be done based on this preliminary, concerning finding, with a larger group of radiologists reading a larger volume of mammograms, to increase statistical power.
Exclusion of BI-RADS 3, 4, and 5 categorizations may perhaps seem a limitation of this audit, but it was not. As a matter of practice on quality and operational grounds, potentially BI-RADS 3, 4, and 5 findings at screening mammography were (and still are) preliminarily categorized as BIRADS 0; all such cases were given BI-RADS categorization 0, and were included in the BI-RADS 0 reports tallied.
Unilateral screening mammograms are often interpreted with a different hanging protocol from bilateral exams. In order not to introduce the extraneous variable of hanging protocol, unilateral mammograms were excluded from this study. It could prove informative to compare unilateral left versus right exams since their hanging protocols would presumably be the same. For instance, perhaps there is no laterality bias in the setting of viewing just one breast; that is, perhaps laterality bias only appears when comparing breasts side-by-side.
The authors' recall fractions were higher than those generally reported as desirable, typically approximately 5–12%.6,13 The vast majority of the authors’ practice reflects poor patients, underinsured or altogether uninsured, and mostly immigrants who may not trust governmental institutions like the authors’, may not speak English, and are new or relatively new to healthcare in the USA. For those and related reasons, a strikingly high portion of the authors’ patients have had no prior mammogram; or, if they have, it often was not in recent years, not obtainable, and/ or of poor quality. When women had no prior mammogram or the most recent mammogram was more than 3 years old, one study found screening recall rates were 67% higher.14 Since comparison to prior exams of quality, particularly those over the past several
years, often obviates recall, the high average recall amongst the authors’ five radiologists is understandable. Furthermore, in a large, multicenter report, four of thirteen sites had recall rates with mammograms done, including tomosynthesis, that were well above the recommended rates for digital mammography without tomosynthesis.15 The Breast Cancer Surveillance Consortium reports that 10% of their 359 radiologists had recall rates over 18%, with some approaching 30%,12 whose patients may face similar impediments to those faced by the authors.
There is no substantive limit to the generalizability of this discovery. Implementation of a tally process regarding laterality and bilaterality would not be envisioned to be difficult, costly, or very timeconsuming. The impact of this observation could be substantial, particularly perhaps in detecting an outlier-performing radiologist in a large group of radiologists, yet remains to be determined.
References
1. Feig SA. Auditing and benchmarks in screening and diagnostic mammography. Radiol Clin North Am. 2007:45(5):791-800.
2. Sprague BL et al. National performance benchmarks for modern diagnostic digital mammography: update from the Breast Cancer Surveillance Consortium. Radiology. 2017;283(1):59-69.
3. PenRad Technologies, Inc. PenRad Mammography Information System. Available at http://www.penrad. comcastbiz.net/pdfs/mainsales_new_ address_2715.pdf. Last accessed: 20 June 2024.
4. Sprague BL et al. New mammography screening performance metrics based on the entire screening episode. Cancer. 2020;126(14):3289-96.
5. Sickles EA et al., “ACR BI-RADS® Mammography,” D’Orsi CJ et al (eds.), ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System (2013), Reston: American College of Radiology; 39-48.
CONCLUSION
Laterality bias may exist in a radiologist who interprets screening mammograms, reflected by rate of advising left versus right immediate recall. The portion of reports recommending recall that is bilateral may simultaneously be assessed. Laterality and bilaterality biases could conceivably occur in the same reader. The authors do not, based simply on their small volume audit, propose what these values should, with high quality, be. How far unilateral recall recommendations may, with high quality, diverge from 50–50, left–right, and what a high-quality range of bilateral (versus unilateral) recalls is or should be, both have the potential to become valuable, quality metrics in screening mammography. These concerns have never before been discussed, let alone addressed. The authors call for them to be evaluated further.
6. Lee CS et al. Assessing the recall rate for screening mammography: comparing the Medicare Hospital Compare dataset with the National Mammography database. AJR Am J Roentgenol. 2018;211(1):127-32.
7. D’Orsi CJ. The clinically relevant breast imaging audit. J Breast Imaging. 2020;2(1):2-6.
8. FDA. Mammography Quality Standards Act Regulations. Available at: https://www.fda.gov/radiationemitting-products/regulations-mqsa/ mammography-quality-standards-actregulations. Last accessed: 20 June 2024.
9. U.S. Department of Health and Human Services. Code of Federal Regulations, Title 45. Available at: https://www. hhs.gov/ohrp/regulations-and-policy/ regulations/45-cfr-46/revised-commonrule-regulatory-text/index.html. Last accessed: 20 June 2024.
10. Hennessey S et al. Bilateral symmetry of breast tissue composition by magnetic resonance in young women and adults. Cancer Causes Control. 2014;25(4): 491-7.
11. Tan SY et al. Comparison of readers' detection of right-sided and left-sided breast cancers and microcalcifications. J Med Imaging Radiat Oncol. 2011;55(4):353-61.
12. Tenny S, Abdelgawad I, Statistical Significance [Internet] (2023) Treasure Island: StatPearls Publishing. Available at: https://www.ncbi.nlm.nih.gov/books/ NBK459346/. Last accessed: June 2024.
13. Lehman CD et al. National performance benchmarks for modern screening digital mammography: update from the Breast Cancer Surveillance Consortium. Radiology. 2017;283(1):49-58.
14. Yankaskas BC et al. Association of recall rates with sensitivity and positive predictive values of screening mammography. AJR Am J Roentgenol. 2001;177(3):543-9.
15. Friedewald SM et al. Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA. 2014;311(24):2499-507.