7 minute read
Genuair®-has it ‘clicked’ yet?





The ONLY pre lled inhaler with visual and audible feedback for confirmed dose delivery1-4

Genuair - a simple to use inhaler for patients with COPD4



Abbreviated Prescribing Information
Eklira® Genuair® 322 micrograms inhalation powder. Please consult the Summary of Product Characteristics (SPC) for the full prescribing information. Presentation: Inhalation powder in a white inhaler with an integral dose indicator and a green dosage button. Each delivered dose contains 375 µg aclidinium bromide equivalent to 322 µg of aclidinium. Also, contains lactose. Use: Maintenance bronchodilator treatment to relieve symptoms in adult patients with chronic obstructive pulmonary disease (COPD). Dosage: For inhalation use. Recommended dose is one inhalation of 322 micrograms aclidinium twice daily. Patients should be instructed on how to administer the product correctly as the Genuair inhaler may work di erently from inhalers used previously. It is important to instruct the patients to read the Instructions for Use in the pack. No dose adjustments are required for elderly patients, or those with renal or hepatic impairment. No relevant use in children and adolescents.


Contraindications: Hypersensitivity to aclidinium bromide or to any of the excipients. Warnings and Precautions: Stop use if paradoxical bronchospasm occurs and consider other treatments. Do not use for the relief of acute episodes of bronchospasm. Use with caution in patients with myocardial infarction in the previous 6 months, unstable angina, newly diagnosed arrhythmia within the previous 3 months, or hospitalisation within the previous 12 months for heart failure functional classes III and IV. Dry mouth, observed with anticholinergic treatment, may be associated with dental caries in the long term. Use with caution in patients with symptomatic prostatic hyperplasia or bladder-neck obstruction or with narrow-angle glaucoma. Do not use in patients with rare hereditary problems of galactose intolerance, total lactose de ciency or glucose-galactose malabsorption. Interactions: Do not administer with other anticholinergic-containing medicinal products. No other interactions expected. Please consult the SPC for more details. Fertility, pregnancy and lactation: No data on use in pregnancy. Risk to newborns/infants cannot be excluded. Consider risk-bene t before using during lactation. Unlikely to a ect fertility at the recommended dose. Side-e ects: Common (1-10%): Sinusitis, nasopharyngitis, headache, cough, diarrhoea, nausea. Uncommon (0.1-1%): Dizziness, blurred vision, tachycardia, palpitations, dysphonia, dry mouth, stomatitis, rash, pruritus, urinary retention. Rare (0.01-0.1%): hypersensitivity. Not known: angioedema, anaphylactic reaction. Pack sizes: Carton containing 1 inhaler with 60 unit doses. Legal category: POM Marketing








Authorisation Number: EU/1/12/778/002 Marketing Authorisation holder: AstraZeneca AB, SE151 85 Södertälje, Sweden. Marketed by: A. Menarini Pharmaceuticals Ireland Ltd., Castlecourt, Monkstown Farm, Monkstown, Glenageary, Co. Dublin A96 T924. Further information is available on request to A. Menarini Pharmaceuticals Ireland Ltd. or may be found in the SPC. Last updated: February 2020
This medicinal product is subject to additional monitoring. This will allow quick identi cation of new safety information. Healthcare professionals are asked to report any suspected adverse reactions to: HPRA Pharmacovigilance, Earlsfort Terrace, IRL - Dublin 2, Tel: +353 1 6764971, Fax: +353 1 6762517, Website: www.hpra.ie, e-mail: medsafety@ hpra.ie. Adverse events should also be reported to A. Menarini Pharmaceuticals Ireland Ltd. Phone no: 01 284 6744.
Date of item: November 2020. IR-BRI-10-2020
Abbreviated Prescribing Information Brimica® Genuair® 340 micrograms/12 micrograms inhalation powder. Please consult the Summary of Product Characteristics (SPC) for the full prescribing information. Presentation: Inhalation powder in a white inhaler with an integral dose indicator and an orange dosage button. Each delivered dose contains 396 µg aclidinium bromide (equivalent to 340 µg of aclidinium) and 11.8 micrograms of formoterol fumarate dihydrate. Also, contains lactose. Use: Maintenance bronchodilator treatment to relieve symptoms in adult patients with chronic obstructive pulmonary disease (COPD). Dosage: For inhalation use. Recommended dose is one inhalation of 340 µg/12 µg twice daily. Patients should be instructed on how to administer the product correctly as the Genuair inhaler may work di erently from inhalers used previously. It is important to instruct the patients to read the Instructions for Use in the pack. No dose adjustments are required for elderly patients, or those with renal or hepatic impairment. No relevant use in children and adolescents. Contraindications: Hypersensitivity to the active substances or to any of the excipients. Warnings and Precautions: Do not use in asthma. Stop use if paradoxical bronchospasm occurs and consider other treatments. Do not use for the relief of acute episodes of bronchospasm. Use with caution in patients with myocardial infarction in the previous 6 months, unstable angina, newly diagnosed arrhythmia within the previous 3 months, or hospitalisation within the previous 12 months for heart failure functional classes III and IV. Discontinue if increases in pulse rate, blood pressure or changes in ECG occur. Use with caution in patients with a history of or known prolongation of the QTc interval or treated with products a ecting the QTc interval. Use with caution in patients with severe cardiovascular disorders, convulsive disorders, thyrotoxicosis and phaeochromocytoma. Hypokalaemia may occur, is usually transient and supplementation not needed. In patients with severe COPD, hypokalaemia may be potentiated by hypoxia and concomitant treatment. Use with caution in patients with symptomatic prostatic hyperplasia, urinary retention or with narrow-angle glaucoma. Dry mouth, observed with anticholinergic treatment, may be associated with dental caries in the long term. Do not use in patients with rare hereditary problems of galactose intolerance, the Lapp lactase de ciency or glucose-galactose malabsorption. Interactions: Do not administer with other anticholinergic and/or long-acting β2-adrenergic agonist containing medicinal products. Caution in use with methylxanthine derivatives, steroids, non-potassium-sparing diuretics, β-adrenergic blockers or medicinal products known to prolong the QTc interval. Please consult the SPC for more details. Fertility, pregnancy and lactation: No data on use in pregnancy. Consider risk-bene t before using during lactation. Unlikely to a ect fertility at the recommended dose. Sidee ects: Common (1-10%): Nasopharyngitis, urinary tract infection, sinusitis tooth abscess, insomnia, anxiety, headache, dizziness, tremor, cough, diarrhoea, nausea, dry mouth, myalgia, muscle spasms, peripheral oedema, increased blood creatine phosphokinase. Uncommon (0.1- 1%): Hypokalaemia, hyperglycaemia, agitation, dysgeusia, blurred vision, tachycardia, electrocardiogram QTc prolonged, palpitations, angina pectoris, dysphonia, throat irritation, stomatitis, rash, pruritus, urinary retention, increased blood pressure. Rare (0.01-0.1%): Hypersensitivity, bronchospasm, including paradoxical. Not known: anaphylactic reaction, angioedema. Pack sizes: Carton containing 1 inhaler with 60 unit doses. Legal category: POM Marketing Authorisation Number: EU/1/14/963/001 Marketing
Authorisation holder: AstraZeneca AB, SE-151 85 Södertälje, Sweden. Marketed by: A. Menarini Pharmaceuticals Ireland Ltd., Castlecourt, Monkstown Farm, Monkstown, Glenageary, Co. Dublin A96 T924. Further information is available on request to A. Menarini Pharmaceuticals Ireland Ltd. or may be found in the SPC. Last updated: October 2019 higher eosinophil count was associated with development of COPD.
This medicinal product is subject to additional monitoring. This will allow quick identi cation of new safety information. Healthcare professionals are asked to report any suspected adverse reactions via HPRA Pharmacovigilance, Earlsfort Terrace, IRL - Dublin 2; Tel: +353 1 6764971; Fax: +353 1 6762517. Website: www.hpra.ie; E-mail: medsafety@ hpra.ie. Adverse events should also be reported to A. Menarini Pharmaceuticals Ireland Ltd. Phone no: 01 284 6744.

Follow-up pharmacological treatment
Patients should be routinely reassessed to determine if their treatment is effectively managing their symptoms and reducing exacerbations. It is always important to assess the patient’s inhaler technique and adherence, as well as non-pharmacological approaches such as smoking cessation or pulmonary rehabilitation before making any adjustments to pharmacological treatment. In some cases it may be appropriate to simply switch inhaler device or molecules within the same class rather than escalating/ de-escalating treatment. Other causes of symptoms should also be considered and investigated as appropriate.
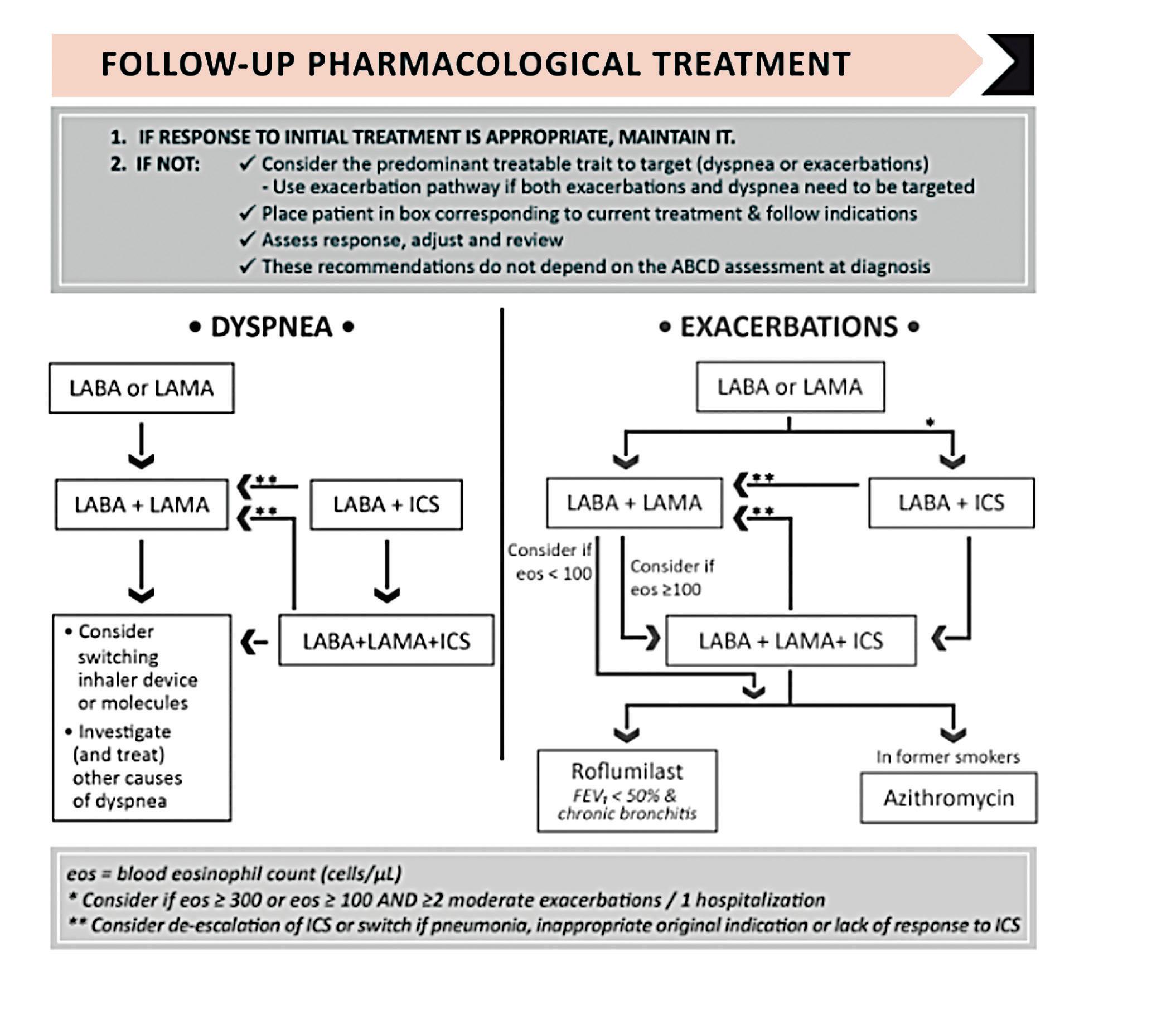
Follow-up treatment of COPD is not based on the patient’s ABCD group, but rather what their predominant symptoms are if not well controlled. GOLD proposes two different treatment algorithms depending on whether the patient’s predominant issue is dyspnoea or exacerbations (in the case where both dyspnoea and exacerbations are an issue, follow the exacerbations pathway) (Figure 4).
The first algorithm is for patients in whom breathlessness or exercise limitation is the predominant symptom. If the patient is on long-acting bronchodilator monotherapy, the use of two bronchodilators is recommended. If this doesn’t improve symptoms, the patient should be stepped down again to monotherapy. For patients who are already on a combination LABA/ICS, consider if the initial indication for ICS was appropriate. If ICS is appropriate, then a LAMA can be added in to start triple therapy. If, however, the initial indication for ICS was inappropriate then the patient should be switched to LABA/LAMA.
For patients in whom exacerbations are the predominant issue, the second algorithm should be followed. For patients on monotherapy with a LABA or LAMA consider escalating to combination therapy with either a LABA/LAMA or LABA/ICS. LABA/ICS may be preferred for patients with (i) a history of asthma, (ii) eosinophils ≥300 with one or more exacerbations a year, or (iii) eosinophils ≥100 with more than two moderate exacerbations/ one hospitalisation.
In patients who develop further exacerbations on LABA/LAMA treatment, blood eosinophil counts should be performed to predict likelihood of beneficial response to the addition of ICS. Patients with eosinophils ≥100 should be escalated to triple therapy of LABA/LAMA/ICS. Patients with eosinophil counts <100 should be considered for the addition of roflumilast or a macrolide antibiotic. These medications should also be considered in patients still having exacerbations on triple therapy.

Newer studies have shown that regular use of some antibiotics (eg, azithromycin 500mg three times per week or erythromycin 250mg twice daily) can reduce the rate of exacerbations for one year in exacerbationprone patients. This benefit is less in active smokers, however. The safety profile of antibiotics such as azithromycin should also be considered before starting treatment as its use is associated with QTc prolongation and an increased incidence of bacterial resistance.
Roflumilast is a PDE4 inhibitor that reduces the number of exacerbations requiring systemic corticosteroids. It should be considered as an additional treatment in patients with an FEV<50 per cent predicted and chronic bronchitis, especially if they have had at least one exacerbation needing hospital admission as it is reported the benefits are greater in patients with a history of exacerbations requiring admission.
Non-pharmacological treatment
It is crucial at all stages of COPD treatment to consider non-pharmacological management (such as smoking cessation and encouragement of regular exercise and a balanced diet). The recommendations for this remain largely unchanged in the latest GOLD guidelines.
Pulmonary rehabilitation is the most effective therapeutic strategy to improve shortness of breath, exercise tolerance, and general health status of patients with COPD and is recommended for all patients with symptoms or at risk of exacerbations. New data included in the 2022 GOLD guidelines highlights the importance of rehabilitation shortly after a hospital admission for an exacerbation of COPD. There is a significantly lower mortality risk for those who start rehabilitation early versus patients who start rehabilitation late or not at all following hospital admission. There is also new guidance with regards to tele-rehabilitation, which shows that it is safe and has similar benefits to in-person programmes. Vaccinations remain an important part of treatment of COPD. The 2022 GOLD guidelines include a new recommendation that all patients should receive Covid-19 vaccines in line with national guidance. It is also important to ensure patients are up-to-date with vaccinations such as influenza, pneumococcus, and Tdap (for adults not vaccinated in adolescence).
Reference
Global Initiative for Chronic Obstructive Lung Disease (2022).
2022 GOLD Reports. https://goldcopd. org/2022-gold-reports-2/.