10 minute read
Allergic rhinitis in focus


AUTHOR: Dr Iseult Sheehan, Clinical Director, Allergy Ireland (www.allergy-ireland.ie)
Case Report
A 15-year-old boy is brought to our clinic by his mother in July, referred by his GP. He has had significant allergic rhinitis symptoms since early childhood. The symptoms are mainly present from May to August.
His main symptoms include rhinorrhoea, sneezing, nasal congestion associated with pruritis to his nose, palate, and occasionally his arms and legs. He also experiences features of allergic conjunctivitis with itchy, watery eyes, and swelling intermittently.
He has recently been experiencing asthma and eczema flare-ups on high pollen count days.
His symptoms are preventing him from sleeping. In addition, he has just completed his Junior Certificate exams. His ability to concentrate and study was hindered and his exam performance was reduced compared to his mock exams.
His parents are very concerned about his Leaving Certificate exams in three years. He is a motivated student with ambitions to attend university. He has
Allergic rhinitis (AR) is a common condition with a global impact. In Ireland, at least onein-five people suffer with AR.1 The economic impact is striking. The European Union recently estimated that the indirect cost of undertreated AR on work productivity may cost between €30-50 billion per year.2 been taking multiple antihistamines daily, which he thinks might be contributing to his fatigue. He is also using an intranasal corticosteroid.
The symptoms of AR are often considered to be trivial and as such AR is underdiagnosed and undertreated. However, the burden of this disease is significant with a reduced qualityof-life for these individuals. It has been shown to affect cognitive and psychomotor function and patients describe the impact on sleep as considerably debilitating.
Examination
The boy appeared tired with dark rings under his eyes. He was visibly mouth breathing.
Flexible nasoendoscopy confirmed rhinitis with significantly oedematous turbinates bilaterally. There was increased mucus and visible mucosal pallor. There were no polyps and no septal deviation. Chest and eye examination was normal.
Skin prick testing was performed, which confirmed a strong sensitisation to grass pollen.
Management
Allergen avoidance measures were discussed and daily saline irrigation of the nasal cavity advised. Given the severity of the symptoms, a short course of topical intranasal corticosteroid drops (Betamethasone) was used followed by the commencement of a combination intranasal corticosteroid and antihistamine spray. Topical mast-cell stabiliser (sodium cromoglycate) eye drops were advised. His symptoms improved and at a review in August he was almost symptom free.
Follow-up
The following year he was commenced on a similar plan from early April. However, on review in early June his symptoms were persistent. A trial of a leukotriene receptor antagonist was commenced, which significantly improved symptom control.
Following the pollen season, he was commenced on sub-lingual grass pollen immunotherapy and tolerated it well. He continued to take immunotherapy daily and the April prior to his exams he recommenced the medication plan as before. His exams went well and he remained asymptomatic throughout. He will continue to take immunotherapy to complete a threeyear treatment plan. As a result, it is expected that he will require less medications to control his allergic rhinitis in the future.
While struggling with AR symptoms, the ability to participate in social and sporting activities is reduced and missed days at work are a feature.
In addition, AR has a worrying impact on a child’s education. Missed or unproductive days at school are common. This becomes particularly apparent during hay fever season, which coincides with exam time. A UK study of teenagers found that there was a reduction in exam performance for those with seasonal AR compared with other times of the year.3 This is most relevant for Leaving Certificate students and those in university.
Epidemiology
It is estimated that AR affects at least
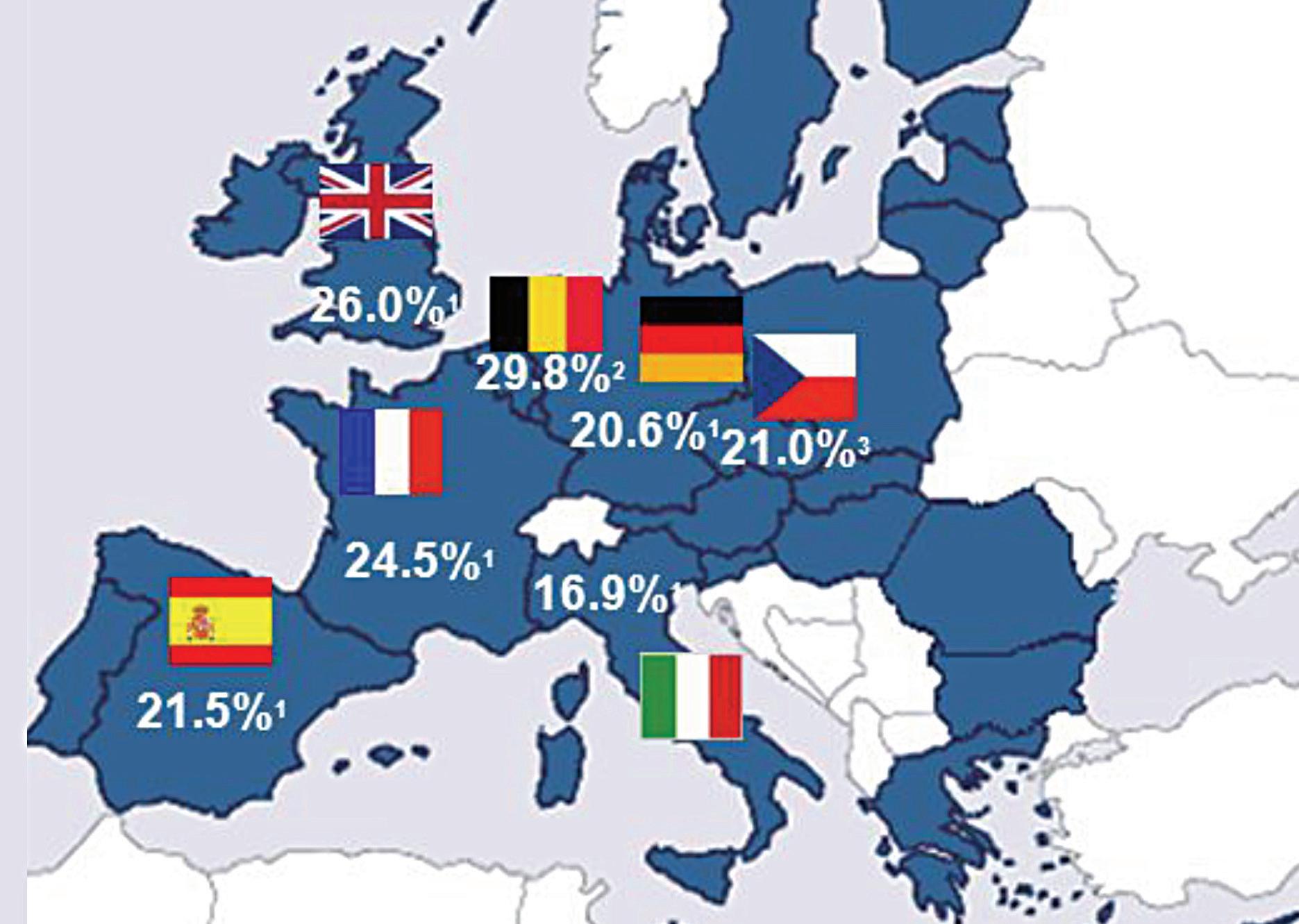
400 million people worldwide and the prevalence within Europe is between 17and-29 per cent.1 The UK has a prevalence of 26 per cent1 and Ireland is likely to be similar to this.
AR will often begin early in life, but prevalence increases with age. The International Study of Asthma and Allergies in Childhood (ISAAC, 2006) phase 3 study demonstrated this, showing a 5 per cent prevalence in those aged three years, an 8.5 per cent prevalence in those aged six-to-seven years, and a 14.6 per cent prevalence in those aged 13-to-14 years.4
What is most concerning is that the prevalence of AR is increasing globally; as was corroborated by this ISAAC study, which found an increase in prevalence of AR from 13-to-19 per cent over an eight-year period in a cohort of 13-to14 year olds.4 A smaller study in Cork demonstrated an increase in prevalence from 7.6 per cent to 10.6 per cent over a five-year period in a cohort of six-to-nine year olds. 5
Nature versus nurture
The cause for this rising prevalence is unclear, although risk factors may include overuse of antibiotics, exposure to air pollution, maternal/passive smoking, and climatic factors among other theories.6
Certainly, environmental exposures are key to understanding the rising prevalence of allergies. The ‘hygiene hypothesis’ was proposed as an explanation whereby the more sterile Western lifestyle was reducing infections and resulting in less type 1 immune responses. More recently, there is a better insight into the development of allergen tolerance with the microbiome during early life being an essential component. Antibiotic use will disrupt this, among other environmental factors.

Exposure to irritants such as cigarette smoke and air pollution, particularly diesel exhaust fumes, has been shown to contribute to and exacerbate AR.
In addition, global warming is seen to be playing a role in Ireland, with milder weather resulting in prolongation of pollen and spore seasons. This is confounded by the introduction of new pollens such as ragweed, which would usually be a common allergen in North America and continental Europe.
Nevertheless, AR appears to be the consequence of environmental exposures in those with a genetic vulnerability. Indeed, genetic predisposition or atopy accounts for at least 50 per cent of AR cases,7 and genetic studies have demonstrated that multiple susceptible loci can contribute to AR alone.8
Multimorbid AR
Multimorbid AR is whereby AR and asthma or atopic dermatitis co-exist. Interestingly, a differing variety of genetically susceptible loci are attributable to multimorbid AR, for example, IL-5 and IL-33 for those with AR and asthma. 8
AR is a risk factor for asthma. In fact 90 per cent of asthmatics have AR and 30-to40 per cent of those with AR have asthma.9
A ‘united airways’ disease approach to management is the more favoured approach in recent years. Moreover, the treatment of nasal inflammation in asthmatics has been shown to improve outcomes. This highlights the importance of assessing for both asthma and rhinitis in these patients.

AR can also be associated with comorbid dermatological conditions, such as atopic dermatitis and urticaria, upon exposure to an allergen. Interestingly, the treatment of AR can very often result in improvements in these dermatological conditions.
Presentation
AR is an IgE-mediated inflammatory reaction following exposure to an allergen. This results in inflammation of the nasal lining and/or conjunctiva. The symptoms characteristically include rhinorrhoea, nasal obstruction, sneezing, and nasal itching.

Additionally, symptoms will often include an itchy palate and irritated, watery itchy eyes with associated periocular oedema or dark rings under the eyes (allergic shiners).
Patients can experience fatigue, snoring, mouth breathing due to nasal obstruction, and a feeling of heaviness in the head or a ‘fuzzy’ head. If the sinuses are affected the patient may experience sinus pressure and headaches and a post-nasal drip.

120mg and 180mg Film-coated tablets
A NEW generation antihistamine offering non-drowsy, long-lasting relief from allergy symptoms
















Abbreviated Prescribing Information


Telfast 120 and 180 mg film-coated tablets
Each tablet contains 120 or 180 mg fexofenadine hydrochloride.
Presentation: Telfast 120 mg: Peach, capsule-shaped, film-coated tablet with 012 on one side and a scripted e on the other side. Telfast 180 mg: Peach, capsule-shaped, film-coated tablet with 018 on one side and a scripted e on the other side. Indications for Telfast 120 mg: Telfast 120 mg is indicated in adults and children 12 years and older for the relief of symptoms associated with seasonal allergic rhinitis. Indications for Telfast 180 mg: Telfast 180 mg is indicated in adults and children 12 years and older for the relief of symptoms associated with chronic idiopathic urticaria. Dosage: Adults and children aged 12 years and over: One tablet once daily before a meal. Not recommended for children under 12 years. Studies in special risk groups (elderly, renally or hepatically impaired patients) indicate that it is not necessary to adjust the dose of fexofenadine hydrochloride in these patients.
Method of administration: Oral. Contraindications: Hypersensitivity to the active substance or any of the excipients. Warnings and precautions: There is limited data in the elderly and renally or hepatically impaired patients. Fexofenadine hydrochloride should be administered with care in these special groups. Patients with a history of or ongoing cardiovascular disease should be warned that, antihistamines as a medicine class, have been associated with the adverse reactions tachycardia and palpitations. Interactions: Fexofenadine does not undergo hepatic biotransformation and therefore will not interact with other medicinal products through hepatic mechanisms. Coadministration of fexofenadine hydrochloride with erythromycin or ketoconazole has been found to result in a 2–3 times increase in the level of fexofenadine in plasma. The changes were not accompanied by any effects on the QT interval and were not associated with any increase in adverse reactions compared to the medicinal products given singly. Animal studies have shown that the increase in plasma levels of fexofenadine observed after coadministration of erythromycin or ketoconazole, appears to be due to an increase in gastrointestinal absorption and either a decrease in biliary excretion or gastrointestinal secretion, respectively. No interaction between fexofenadine and omeprazole was observed. However, the administration of an antacid containing aluminium and magnesium hydroxide gels 15 minutes prior to fexofenadine hydrochloride caused a reduction in bioavailability, most likely due to binding in the gastrointestinal tract. It is advisable to leave 2 hours between administration of fexofenadine hydrochloride and aluminium and magnesium hydroxide containing antacids. Fertility, pregnancy and lactation: Fexofenadine hydrochloride should not be used during pregnancy unless clearly necessary. Fexofenadine hydrochloride is not recommended for mothers breast-feeding their babies. No human data on the effect of fexofenadine hydrochloride on fertility are available. In mice, there was no effect on fertility with fexofenadine hydrochloride treatment. Driving and operation of machinery: On the basis of the pharmacodynamic profile and reported adverse reactions it is unlikely that fexofenadine hydrochloride tablets will produce an effect on the ability to drive or use machines. In objective tests, Telfast has been shown to have no significant effects on central nervous system function. This means that patients may drive or perform tasks that require concentration. However, it is advisable to check the individual response before driving or performing complicated tasks. Undesirable effects: Headache, drowsiness, dizziness, nausea. Refer to Summary of Product Characteristics for other undesirable effects. Pack size: 30 tablets. Marketing authorisation holder: Opella Healthcare, 82 Avenue Raspail 94250, Gentilly, France SAS T/A Sanofi. Marketing authorisation number: PA23180/003/002-003. Medicinal product subject to medical prescription. A copy of the SPC is available on request or visit www.clonmelhealthcare.ie. Last revision date: March 2022.
Compression of the olfactory nerve due to oedema within the nasal cavity can result in an altered sense of smell and/or taste.
Pathophysiology
There are two phases which are paramount to the development of an allergy. Phase one occurs when an atopic individual is first exposed to the allergen. The allergen is taken up by antigen-presenting cells, particularly dendritic cells (DC), and is processed into peptide fragments. The DC will move through the lymphatics towards the lymph node where it will present this peptide fragment to a naïve T-cell.
The naïve T-cell becomes activated to express cytokines, particularly IL-4, which drives the differentiation of these cells to Th2 helper cells. An environment rich in cytokines IL-4 and IL-13 is created and is responsible for inducing IgE production from B-cells. Additionally, IL-5 is responsible for eosinophil recruitment and activation. The cytokine profile is vital as it determines a Th2 immune response.
In the meantime, T-cell dependent activation of B-cells stimulates further cytokine production, particularly IL-4, and promotes irreversible immunoglobulin class switching to allergen-specific IgE antibodies.
Allergen-specific IgE will attach to mast cells and basophils. This is referred to as primary sensitisation. In addition, memory B-cells are generated and a small number of memory T-cells remain.
Phase two occurs on subsequent exposure to this allergen. The allergen binds to the sensitised mast cells, triggering degranulation of the mast cell; releasing pre-stored and newly synthesised inflammatory mediators such as histamine, leukotrienes, and prostaglandins. These contribute to vascular permeability, eosinophil infiltration, and increased mucus production.
Furthermore, with repetitive allergen exposure, nasal priming occurs. This appears to cause an accumulation of effector cells in the nasal mucosa and results in a hyper-responsiveness to the allergen and prolongation of symptoms. In addition, there appears to be a neural component to this hyper-responsiveness. Changes to the sensory nerves of the nose have been demonstrated in those with AR. In addition, innate immune responses can be initiated in the nasal epithelium by allergens directly compromising the epithelium and resulting in the release of alarmins such as IL-33, further activating the inflammatory response.

Classification of AR
AR can be divided into seasonal and perennial based on allergen triggers. Seasonal rhinitis includes sensitisation to grass, tree, or weed pollen, and fungal spores. Whereas perennial rhinitis is commonly triggered by house dust mite or animal dander. This classification system is effective at giving a likely diagnosis of the trigger, which assists with recommending appropriate avoidance measures.
However, a new classification system focusing on the functional ability of the patient, including the frequency and severity of symptoms, has become a much more effective tool for making treatment decisions. This guideline was developed by Allergic Rhinitis and the Impact on Asthma (ARIA) in collaboration with the World Health Organisation (WHO).9
Diagnosis of AR
The diagnosis of AR is generally based on clinical symptoms. However, skin-prick allergy testing or specific IgE blood testing can be used to confirm the allergen trigger.
In addition, it is vital to examine the nose whereby you will often see bulky oedematous turbinates with visible increased mucus production (Images 3 and 4). Pallor of the mucosal lining is often present, particularly in longstanding cases. Occasionally, the mucosa will lose its smooth appearance and instead will have ridges and pitting from chronic allergic challenge. Pre-polypoid tissue can occasionally be present.

Non-pharmacological management
Allergen avoidance should be discussed. Nevertheless, avoidance alone is generally not sufficient to manage symptoms. In cases where the allergen trigger is animal dander, avoidance is effective if the animal is removed from the home.
Smoking cessation should be advised always. Smoking can be associated with chronic nasal symptoms and may even be associated with the development of polyposis. Passive smoking or ‘vaping’ appear to carry similar risk.
Saline irrigation is an effective way to directly cleanse the nasal cavity with the resultant reduction of mucus, inflammatory mediators, and bacterial burden. It has also been shown to improve mucociliary function.
Pharmacological management
In patients with mild intermittent symptoms an antihistamine is