Beyond the Magic 8 Ball:
Choosing the Right Supply Chain Partner
Healthcare leaders share the questions, red flags, and best practices that separate strong partnerships from risky ones.

Healthcare leaders share the questions, red flags, and best practices that separate strong partnerships from risky ones.
HealthTrust Performance Group solves the toughest challenges by leveraging our decades of senior level healthcare experience to optimize clinical and operational performance while providing unmatched savings. Its a difference only HealthTrust can make.

Health: Bridging the Research Gap
Cleveland Clinic advances women’s health through tailored care for women in their midlife.
Medical Gaslighting
A disparity of trust between clinicians and patients.
The Journal of Healthcare Contracting is published bi-monthly by Share Moving Media
350 Town Center Ave, Ste. 201 Suwanee, GA 30024
Phone: 770/263-5262 FAX: 770/236-8023 e-mail: info@jhconline.com www.jhconline.com
John Pritchard jpritchard@sharemovingmedia.com
OF BUSINESS DEVELOPMENT Anna McCormick amccormick@sharemovingmedia.com
The Journal of Healthcare Contracting (ISSN 1548-4165) is published bi-monthly by
2025 by Share Moving Media All rights reserved.
Please note: The acceptance of
Beyond the Magic 8 Ball: Choosing the Right Supply Chain Partner
Healthcare leaders share the questions, red flags, and best practices that separate strong partnerships from risky ones.
The State of Rural Healthcare
The challenges facing rural healthcare and potential policy solutions.
Why can’t supply chain’s relationship with clinicians be like playing Tetris?

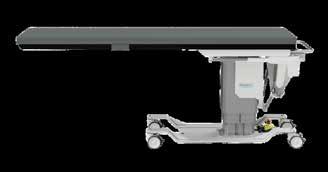
Burnout and changing workforce dynamics put pressure on Ambulatory Surgery Centers.
BY PETE MERCER
Staffing shortages are one of the most prevalent challenges facing the healthcare industry, and ambulatory surgery centers are no exception. As ASCs continue to grow in popularity due to convenience and cost-effectiveness, so does the demand for skilled teams to take care of patients. Healthcare can be sort of a revolving door when it comes to employees, and it’s not easy to keep facilities staffed in those kinds of conditions.
In the following story, Erin Boers, VP, HR Services at MedHQ, and Mayte Rechani, Executive Director at MedHQ, discussed navigating staffing challenges for ASCs, the toll of burnout in a healthcare environment and how to improve employee engagement. MedHQ is a provider of healthcare advisory and administrative solutions, including HR and staffing, to ASCs and other organization types.
Like every other healthcare setting, there have been numerous shifts for the ASC workforce in recent years. The world has changed so much since 2020, especially for healthcare workers. The pandemic alone created a seismic change in how the public viewed the healthcare industry, both positive and negative, and the fallout from that has completely transformed the landscape of the industry.
One of the most significant components of that fallout is the staffing shortage. The National Library of Medicine published a study showing that more than one-third of nurses will reach retirement age in the next 10 to 15 years, while the National Council of State Boards of Nursing reported in 2023 that 100,000 nurses left the profession altogether during the pandemic due to stress, burnout, and retirement.
There are very serious ramifications for these shifts, creating vacuums in patient care settings that are either being left open or filled by overworked employees, which further perpetuates the issue. This also extends to ambulatory surgery centers.
As more and more patients are migrating towards ASCs for safe, efficient and cost-effective care, the need for more staff becomes greater. “They are busier than ever, increasing the need for staff,”
Rechani said. ““Surgeons are transitioning their surgeries from the acute care setting to ASCs, where they have more autonomy and can help reduce costs.”
With the influx of new patients, employees at ASCs are seeking more stability within the ASC system. While the traditional challenges of working in a hospital are largely absent in this environment, ASCs still come with their own. “There is an increased demand for flexibility,” Boers said. “Employees are seeking more predictable schedules, better work-life balance, and flexible benefits. There’s also a noticeable shortage of skilled nurses and surgical techs, driving up competition with hospitals and other healthcare facilities.”
Burnout is pervasive, no matter what kind of setting employees are working in. Burnout in a traditional hospital setting received lots of attention and recognition as a problem during the height of the pandemic, but healthcare workers have experienced burnout for years. This is what leads to employees leaving the healthcare industry in droves, further perpetuating the staffing shortages that are creating so many of these problems.
That’s no different for outpatient clinics. Staff at ASCs experience burnout in a different way, according to Rechani. “While they may not work weekends and normal workday schedules, they rarely have any time off due to the ASC staffing shortages. ASCs are looking at different alternatives to have shifts covered, but if they are not utilizing a good agency partner, they will not be covered. In these cases, procedures may be cancelled at the last minute.”
Even though the ASC setting allows for employees to work regular hours, these facilities are designed to be lean operations with high standards of performance in a fast-paced environment. An environment like this is a perfect breeding ground for burnout, so it’s important to understand how to actively fight against the things that contribute to fatigue.
“At MedHQ, we work with ASC leadership to implement proactive measures, including regulator engagement and check-ins, mental health and EAP programs, workload management tools, and leadership training focused on empathetic management,” Boers said.
to improve the messaging and showcase what drives the heart behind the work. This gives the incoming (or even existing) employees something concrete that they can grab onto.
“While ASCs’ branding is paramount to attracting top talent, ASCs are not always clear with their messaging,” Rechani said. “What exactly are they offering new talent? What is the culture at the ASC? Younger talent right now is looking for any employer to be a ‘good fit’ for them – they’re prioritizing their mental health over an easy work schedule, while the more seasoned talent is prioritizing work schedules and mental health.”
“ There is an increased demand for flexibility. Employees are seeking more predictable schedules, better work-life balance, and flexible benefits. There’s also a noticeable shortage of skilled nurses and surgical techs, driving up competition with hospitals and other healthcare facilities.”
Company culture plays a significant role in the retention of the workforce, keeping them engaged with their work and the mission and vision of the company. When the culture is aligned with the values of the organization, it’s easier to engage the team with their work. This is essential, because the comfort and safety of the patient is at stake. Engaged employees mean that patients are taken care of.
Part of the challenge is creating an attractive environment to new employees. Defining the culture, as well as the mission and values of the organization, helps
It’s all about telling the story of why the organization was started, where it’s come from, and where it’s going in the future. Tapping into that story gives employees something to believe in for the important work that they’re doing.
Boers said, “Employer branding and culture are critical in today’s talent market. ASCs have a compelling story to tell: high-quality care, a focused specialty setting, less bureaucracy, and better worklife balance than many hospital environments. However, these advantages must be clearly communicated. A strong brand and culture not only attract talent – they help retain it.”
Cleveland Clinic advances women’s health through tailored care for women in their midlife.
BY JENNA HUGHES
Women’s health issues, especially for patients age 40 and older, have for many years been misunderstood and under researched. As a result, many women are not aware of the health changes and symptoms that can come with aging and midlife.
“Much of women’s health has been understudied historically. There are many conditions that are female specific or that disproportionately impact women, or that impact women differently than men, and many of these issues have not been well studied,” said Dr. Pelin Batur, Department of Subspecialty Care for Women’s Health, within the Ob/Gyn & Women’s Health Institute at Cleveland Clinic.
To address the growing healthcare gap for middle-aged women, Cleveland Clinic launched the Women’s Comprehensive Health and Research Center, with the help of Maria Shriver, a well-known
journalist, women’s health advocate, founder of the Women’s Alzheimer’s Movement at Cleveland Clinic and the center’s Chief Visionary and Strategic Advisor, to empower women to navigate their personal health journey with confidence and clarity.
The Center specifically focuses on women as they move through their 40s, 50s, 60s and beyond in facing health changes head on and feeling their best.
“It seemed like for women in midlife and beyond, healthcare fell off the map,” said Dr. Batur. “We knew that this was a critical group needing focused care.”

Since its launch in 2024, the Women’s Comprehensive Health and Research Center has served more than 10,000 patients, scheduled more than 19,000 appointments and hosted more than 1,000 virtual shared medical appointments focused on menopause.
The one-year anniversary of the Women’s Comprehensive Health and Research Center was celebrated at Cleveland Clinic’s inaugural Women’s Health Forum in June 2025, which brought together national leaders in healthcare, research and advocacy and served as both a celebration of progress and a call to action for the future of women’s health.
Women’s health issues such as menopause have a significant impact on an individual’s well-being, sleep, mental health and entire body.
“The lack of research around women’s midlife health is problematic because nearly 6,000 women each day go into menopause, and at that time in their life see a lot of changes in their health and their body,” said Dr. Batur. “In fact, 78% of women 55 and older have a chronic
disease that they are dealing with, and the healthcare industry has not done a great job in studying these individuals and finding how to best take care of them.”
Menopause is a normal part of aging for women – not a disorder or disease – according to the National Institute on Aging. Some women have mild or no menopausal symptoms, but for others, the menopausal transition can bring various symptoms, including hot flashes, night sweats, trouble sleeping, joint and muscle discomfort, pain during intimacy, moodiness and irritability, forgetfulness, difficultly concentrating, or a combination of these.
Menopause symptoms can be managed through a variety of interventions including hormone therapy, medication and lifestyle adjustments. Treating menopause therefore requires a treatment plan that is tailored to each patient’s individual needs.
“The long-term Women’s Health Initiative Study came out to help answer the specific question of if all women should be on hormone prevention for treatment of menopause symptoms –the answer is that clinicians must weigh the pros and cons of the therapy for each individual patient,” said Dr. Batur. “For many years in the healthcare industry clinicians advised women against hormones, but the study proved it is more complicated than that, and women didn’t want to keep suffering through symptoms, they wanted solutions.”
The Women’s Comprehensive Health and Research Center attempts to bring an ‘in-between’ perspective to the treatment of women’s health issues by focusing on each individual patient’s potential to benefit from hormone therapy and other treatments.
“Hormone therapy is not poison, and it’s also not the fountain of youth,” said Dr. Batur. “The truth is that its somewhere in between, and we can only help women by educating our patients and clinicians and getting each individual the care that they need.”
In response to female patients’ ongoing health concerns, Cleveland Clinic’s Women’s Comprehensive Health and Research Center chose to focus on a unique approach to care with four pillars: Connectivity, Access, Research, and Education.
a variety of different types of healthcare providers in one place.
“Our women’s behavioral health team, sleep neurologist, our hormone specialists, and our primary care doctors meet on a regular basis now to connect, teach each other, and figure out how best to serve our patients,” said Dr. Batur.
The healthcare programs available to women at the Center were built with accessibility for the average patient in mind – addressing economic barriers to care, acknowledging patient’s day-to-day personal responsibilities and keeping in mind scheduling and time concerns.
Beyond menopause, the Center can create a plan to manage patient concerns including Alzheimer’s disease, breast pain, cancer risk assessment and genetic screening, diabetes, irregular periods, osteoporosis, pelvic pain and much more.
“What we really want to do is connect (Connectivity Pillar) clinicians so that they are not looking at patients through their own specialty silo only. The Access Pillar explores how we bring access close to the patient with virtual visits and longer appointments,” said Dr. Batur. “Research is answering the questions that patients have for the clinic, and Education empowers patients to make informed decision and educate colleagues about the importance of women’s health.”
Clinicians at Cleveland Clinic work together on complex women’s health issues to address the whole person and form a personalized treatment plan. The Center is built around allowing women to access
“Virtual care options are now available in 20 states across the U.S. to understand a patient’s preventative and health needs,” said Dr. Batur. “These services are accessible to everyone no matter the socioeconomic status or where throughout the nation they are coming from.”
The first step for patients who want to make an appointment at the Women’s Comprehensive Health and Research Center is to call and talk to a trained navigator at the Welcome Center.
Trained navigators meet with the facility’s doctors on a regular basis to communicate, so that when a patient calls, they can talk candidly about their health concerns to someone who understands them.
Once a patient reaches out, a navigator then schedules an evaluation to begin building them a personalized care plan.
Beyond menopause, the Center can create a plan to manage patient concerns including Alzheimer’s disease, breast pain, cancer risk assessment and genetic screening, diabetes, irregular periods, osteoporosis, pelvic pain and much more.
90-minute virtual shared medical appointments, with real experts leading the conversation, to provide women with credible health information and everything they need to know about their health concern or diagnosis.
“These appointments are generally shared with five 15 other women, with the opportunity throughout for questions
Right now, the clinicians at the Women’s Comprehensive Health and Research Center plan to go forward by acknowledging the interconnected nature of women’s health and addressing health issues throughout the lifespan by expanding its services in the next four to five years.
Nearly two-thirds of Americans living with Alzheimer’s are women, according to the Alzheimer’s Association. Women are at the center of the Alzheimer’s crisis, but their experiences have long been overlooked in research. Cleveland Clinic aims to address these gaps through the first-ofits-kind Women’s Alzheimer’s Movement Prevention and Research Center. This program is designed to address women’s individualized risk for Alzheimer’s and is available through the Women’s Comprehensive Health and Research Center.
“We formed the Women’s Comprehensive Health and Research Center to really listen to and understand the voice of our patients who had felt as though physicians weren’t listening and doctors weren’t talking to each other, and to shed light on hormone therapy, as many people were misinformed about it as a treatment option.”
Cleveland Clinic is also revolutionizing the approach to patient appointments by addressing patient concerns through
that the patient themselves may not have asked,” said Dr. Batur. “This ensures that clinicians are providing patients with all the education they need so they can make informed decisions.”
The Cleveland Clinic Women’s Health Forum in June 2025 aimed to shed light on women’s health issues – with panel discussions on menopause, wellness, aging, and work-life balance, fireside chats, a conversation with a female author, a video series launch, and more led by Cleveland Clinic specialists and influential women executives.
“We learned that women have been craving this type of event, and the energy at the Forum was palpable,” said Dr. Batur. “Women want to see change and advancements on these topics. They weren’t aware that these types of services, such as the Women’s Comprehensive Health and Research Center, were available and they
were enthusiastic about getting connected. This is why we’re here, and why we’re planning to host another Forum for next year.”
Takeaways of the conference included the advancement of women’s health innovation, showcasing the latest research on women’s health and fostering collaboration – but most importantly it was a space where women felt seen and supported, according to Dr. Batur.
“We started the Center focusing on midlife and beyond because it was an area of need,” said Dr. Batur. “Eventually our goal is to make this Center about serving women across the lifespan.”
For example, a woman’s care during pregnancy can impact cardiovascular disease in midlife, or how healthy blood vessels are at midlife can impact dementia risk in a woman’s later years of life.
“We need to be aware of how to take care of a variety of female patients in early life, diagnose and treat them, so that we can prevent issues like high blood pressure, brain health issues and whether a woman will age into wellness or disease,” said Dr. Batur. “We do a good job of care throughout the lifespan at Cleveland Clinic already and need to build on this going forward.”
Right now, the clinicians at the Women’s Comprehensive Health and Research Center plan to go forward by acknowledging the interconnected nature of women’s health and addressing health issues throughout the lifespan by expanding its services in the next four to five years.
“I’m proud to work in a place where colleagues feel passionate about this type of care for women,” said Dr. Batur. “We are able to reach more women and spend face to face time with them, and I know that we each truly care about managing each patient’s health holistically.”











Cardinal Health™ Lab Distribution: Products and Services
With labs navigating challenges like financial pressures, staffing shortages and unpredictable supply cycles, the need for stronger supply chain resilience and reliability has never been greater. But, finding a distributor who helps build trust, equity and convenience can be difficult and frustrating.
Cardinal Health provides customized solutions designed to help labs overcome these daily obstacles with confidence.
With a rich history of distribution excellence and decades of lab expertise, we are committed to providing value-added services and regularly advise our lab customers on the right mix for their facility.
Cardinal Health™ Lab Briefings webinar series
A monthly ASCLS P.A.C.E.® and Florida-accredited webinar series that supports lab professionals' career growth through continuing education and expert-led insights into the latest industry trends.
Cardinal Health™ OptiFreight® Logistics
Comprehensive and reliable shipping solutions to optimize the flow of your packages and help you ship them at the best total value.
Cardinal Health™ Reserved Inventory Program
The first-of-its-kind program enables customers to reserve dedicated quantities of respiratory testing products for supply assurance all season long.
Cardinal Health™ Strategic Stock Solution
Customer-owned inventory managed by Cardinal Health.
Cardinal Health™ Wavemark™ Lab Supply Solution
This digitally automated solution provides workflow optimization, product traceability, real-time data analytics and actionable insights on product supply within your laboratory.
Cold chain and hazardous material handling
Proper treatment of sensitive products, stored at a distribution center near your facility.
Data-driven insights
Standardization and formulary tools to enhance facility purchasing power.
FourKites enhanced shipment visibility
Real-time shipment milestones to provide customers with visibility to shipments in-transit, fueling predictive analytics and machine learning.
Kinaxis™ advanced planning and visibility
Machine learning and advanced inventory planning analytics to build greater connectivity with carriers and help optimize product availability amid disruption.
Kitting solutions
An effective combination of products, packaging, instructions and compliant labeling to accommodate your specialized kitting requirements, from blood and urine collection kits to tissue biopsy and direct-to-consumer kitting.
Leasing services
Dedicated leasing and diagnostic specialist teams provide customized payment options that meet your capital financing needs.
Product availability biweekly tracking and communication
Stay informed with regular Cardinal Health™ Brand and select national brand product availability updates delivered right to your email.
assurance program (QAP)
Access to a team of specialists with expertise in developing the optimal QAP for your facility, overseeing select order renewals and creating standardized or custom shipping cycles to best fit your standing order requirements.
A dedicated inventory team providing ongoing reviews of available product, proactive supplier constraint mitigation, monitoring of CDC reporting and historical data to anticipate seasonal spikes and moderating demand by geographic regions.
Tried-and-true sequestered lots provide elevated management of sequestered, one-lot and dated materials to help reduce costs and drive operational efficiencies, minimizing recalibration requirements due to multiple lot switches.
Supply chain assessments
A no-cost assessment that provides strategic supply chain recommendations tailored to your facility’s needs.
We’re more than just box movers — we're a preferred laboratory distributor and service provider of top healthcare providers, and we have been for decades.* With a rich history of distribution excellence, 200 experienced lab professionals and a broad portfolio of clinically equivalent Cardinal Health™ Brand Products, you can count on us for financial savings, operational efficiencies and supply continuity.
Transparency without the hidden costs or fees. One point of contact. Deep supplier relationships. Always-on service. That’s the Cardinal Health way.
For more information, scan the QR code to connect with a lab expert or visit cardinalhealth.com/labdistribution
A disparity of trust between clinicians and patients.
BY PETE MERCER
In healthcare, one size does not fit all. Each patient has a unique and dynamic health background that often requires a tailored approach to addressing their health concerns. While there is an overall foundational approach to treatment options, it needs to be a good fit for the patient. Otherwise, they might be getting treatments that are not necessary, effective, or even worse, could cause further harm to the patient.
A recent report published by the ECRI found that “dismissing patient and caregiver concerns” is at the top of the list of the most significant threats to patient safety in 2025. In a media release regarding the report, ECRI says that “time and resource constraints make it increasingly difficult for some clinicians to provide empathetic care that addresses patient and caregiver concerns, potentially leading to missed and delayed diagnoses.”
This is indicative of a larger problem – a lack of trust between clinicians and patients. ECRI is referring to this phenomenon as medical gaslighting, a term that the American Journal of Medicine has defined as “an act that invalidates a patient’s genuine clinical concern without proper medical evaluation.”
In the following story, Shannon Davila, MSN, RN, CPPS, CIC, CPHQ, FAPIC, executive director of total systems safety at ECRI, and Marcus Schabacker, MD, PhD, president and CEO of ECRI, discuss what medical gaslighting is and how it impacts clinicians and patients alike.
An important thing to understand about medical gaslighting is that the traditional
definition of gaslighting (i.e. manipulating someone in such a way that they begin to question their own sanity) does not apply to medical gaslighting. In a medical gaslighting case, patients feel that their health concerns are not being validated or addressed by their clinicians.

It is also important to understand that this is not a new experience. For years, patients have complained about feeling dismissed or not heard when it comes to their own health concerns. In recent years, there have been a couple of high-profile cases where celebrities have experienced medical gaslighting. After Serena Williams had a baby in 2017, she
experienced shortness of breath and alerted medical staff to the issue. They did not believe her at first, but a CT scan revealed pulmonary embolism.
Sharon Stone has also recently been more candid about her experience with a ruptured vertebral artery in 2001. In her case, the doctors missed it on the first scan, so they assumed there was nothing wrong with her. After getting a second opinion, Stone had to undergo a procedure to get it fixed.
In both cases, the situation could have resulted in more serious injury or even possible death if they had not advocated for themselves over and over again. Celebrity cases like these go a long way in raising awareness for this issue. In the Hippocratic Oath, young and upcoming doctors swear to “do no harm” – the reality is that most healthcare professionals take that creed very seriously.
Davila said, “We wanted to be sensitive when we brought this issue up because healthcare is such a complex environment – doctors, nurses, and others are being asked to do so much with limited resources every day. Most people, the majority of healthcare workers, do not go to work saying, ‘I’m going to ignore or disregard a patient.’ No one has that
intent. They always want to do the best for their patients.”
So, what is happening here? Without a doubt, healthcare workers face an enormous amount of pressure on a daily basis. They can only commit a certain amount of time to each patient, which creates this tension between caring for each patient and maintaining productivity goals. Additionally, cognitive bias can also lead to patients feeling as though they are being dismissed. The ECRI report found that, whether they know it or not, many clinicians have “biases that reflexively attribute symptoms to issues like mental illness, age, or weight,” which can greatly influence diagnostic decisions.
As an example for what this can look like, Davila said that if a clinician in an emergency department at a hospital sees five patients and they are all diagnosed with the flu, the sixth patient that comes in with a fever and a cough, it’ s possible that that patient would be diagnosed with the flu as well.
Whether they know it or not, providers walk into each interaction with a patient with some sort of bias that is informed by circumstances that may or may not be related to the specific patient they are seeing. “You have to really think independently for each patient. Cognitive bias might be different than medical gaslighting, but it’s still not processing the information in a really critical and thoughtful way so that you can make the right diagnosis,” Davila said.
The patient-clinician relationship
Inevitably, this scenario will have an impact on the patient-clinician relationship. The most significant casualty in
this medical gaslighting scenario is trust. Overcoming that barrier of distrust in the patient-clinician relationship is very difficult when the patient feels like they have been dismissed. With all of the health issues that many adults in America are facing right now, it’s really important to have a clear and open dialogue about what the patient is experiencing. If the patient does not feel comfortable sharing that information, it’s detrimental to the entire healthcare ecosystem.
Davila said, “A patient only has to feel like they have been dismissed once by someone. If you arere having a conversation with anyone and you feel like they are being disrespectful or not hearing you, you are probably not going to feel comfortable communicating with t with that person.”
Once this starts to impact the patientclinician relationship, it can become quite difficult to rebuild that trust. At some point, the patient could begin to withhold important information about their symptoms or their overall health. From there, any diagnosis that the clinician is going to give might be looked at with some measure of skepticism. If they do not feel that they can trust the clinicians, why would they trust the diagnosis?
That’s even assuming that the diagnosis is correct – if the clinician is given the full scope of health or they are not listening to the concerns of the patient, it becomes much easier and much more common to misdiagnose.
“From a clinical standpoint, it really opens up the opportunity for diagnostic errors,” Davila said. “If patients do not feel comfortable sharing about things like depression and anxiety – or in the case of Serena Williams, a physical chest
pain – then you are going start seeing that the providers are not getting the information that they need to adequately make those diagnoses.”
Davila and her team found that by putting medical gaslighting as a top safety concern, they had multiple people share that they had also experienced medical gaslighting at some point. While they knew it was important to use this as an opportunity to educate providers about this issue, it was not the only goal of the report.
“We know nobody wants to be perceived as dismissing patient’s concerns. We saw an opportunity to educate health providers, but this was not just about education – we also wanted to acknowledge the patients and families. We know this is happening and we really wanted to help their voices be heard,” Davila said.
With a clearer picture of the scope of medical gaslighting, how can healthcare organizations put structures in place to fix this? ECRI president and CEO Marcus Schabacker said that the first step to rectifying any of the systemic flaws that perpetuate adverse events like medical gaslighting and cognitive bias is to create an environment where the staff feel safe to report errors, near misses, and system vulnerabilities. He calls this a ‘just culture.’
“Just culture is a model of accountability – one that applies not only to individuals, but also to the organization itself,” he said. “It recognizes that while individuals are responsible for their choices, the organization is responsible for shaping those choices. In a just culture, clinicians are held responsible
for their actions. At the same time, the organization is accountable for designing systems that support safe, effective care and for responding to failures with learning, not punishment.”
When staff members feel safe to report any issues, it will help healthcare organizations to build robust data that gives a better picture of any vulnerabilities and risks. From there, the data can be analyzed to identify the challenges and create proactive prevention measures to mitigate those challenges.
According to Schabacker, leaders have to model transparency, reinforce safety as a core value, and ensure that policies and workflows reflect the realities of the clinical practice to reinforce the accountability between clinical staff and clinical leadership. If it’s going to work, leadership has to set the tone for the rest of the organization.
On the other side of the equation, frontline clinicians need to know that speaking up about risks or mistakes is not just safe, but an expectation. “Together, this dual accountability creates the foundation for total systems safety: a healthcare environment where safety is embedded, trust is reinforced, and learning is continuous.”
Ensuring the safety of the patient is paramount to improving the quality of the clinician-patient relationship and eradicating medical gaslighting. Developing a systems approach is essential for healthcare organizations that are aiming to achieve safe, high performing, and efficient patient care, rooted in the understanding
that healthcare is a complex, adaptive, sociotechnical system.
“Outcomes are shaped not just by individual actions, but by the design of the system itself: its physical environment, tasks and processes, tools and technologies, organization, and people, as well as the external environments,” Schabacker said. “A systems-based approach seeks to identify and redesign the system components that influence outcomes in a manner that facilitates safe, effective, and efficient care.”
also require a unified front to ensure that everyone is aligned with the mission and vision of the leadership team.
Without that unified approach, these strategies often result in greater fragmentation, which is another significant barrier to patient safety. If your organization is implementing siloed safety measures, it is much more difficult to scale these operations or align them with other departments in the organization.
Obviously, this does not create a sustainable, system-wide change for providers.
“A strong safety culture is one where safety is not just a priority, but a core value embedded in every decision and process. Cultivating this culture requires more than training, slogans, or frameworks.”
Improving patient safety protocols requires an all-hands-on-deck, uniform approach to overcome these challenges. According to Schabacker, shifting towards an integrated, system-wide strategy is the most effective way to improve patient safety, like embedding safety deep into the organizational culture, aligning incentives, and using shared frameworks to guide improvement at each stage of the journey.
Building a strong safety culture is a big step towards improving patient safety, simply by making it a priority across the board. He said, “A strong safety culture is one where safety is not just a priority, but a core value embedded in every decision and process. Cultivating this culture requires more than training, slogans, or frameworks. It involves redesigning systems to support safe behaviors, aligning policies with values, and modeling safety leadership at every level.” Implementing a culture that’s focused on safety will
By leveraging unification and standardization, healthcare leaders are able to establish a firm foundation of safety that reflects the goals and vision of the entire organization, making it easier to create meaningful change. However, the main caveat here is that leadership needs to be willing to accept the hard truth about the state of patient safety today.
As organizations like ECRI continue to shed light on these issues, it will continue to bring awareness to things like medical gaslighting. But it requires the leadership teams to make challenging decisions in order for anything to change.
“As long as boards, CEOs and senior executives continue to accept the alarmingly high rates of preventable harm in healthcare today as collateral damage, things will not change. We also need patients and the general public to become more aware and more vocal about the need to make healthcare safer.”

Distributors and self-distributing health systems now have complete transparency of their Dukal products’ from purchase order to delivery.
Product Assigned at the Factory Level
Product Tracking at the Item Level
Compatible Excel Reporting
Automated Communication
Worldwide Tracking

Scan
> Learn more at dukal.info/insight
Currently, 6 in 10 Americans live with at least one chronic condition and 4 in 10 manage two or more. These diseases account for 8 in 10 of the leading causes of death nationwide. Contributing risk factors include physical inactivity, poor nutrition, tobacco use and excessive alcohol consumption.1,2
If a patient receives a chronic disease diagnosis, ongoing monitoring and treatment require continued lab testing throughout the rest of the patient’s life. These conditions present a growing strain on our health system and providers are looking for efficiencies in every area of their process.
Chronic disease costs the American medical system over $1 trillion annually — and is estimated to cost $47 trillion globally by 2030. 2



Cardinal Health provides our distribution customers with robust capital equipment support to help increase lab capacity and diminish the strain of chronic disease. With Cardinal Health, you receive end-to-end support with single-source access to top manufacturers, expert consultation in equipment choice and assay menu expansion, extensive leasing options and access to a team of specialists that helps optimize your quality assurance program (QAP).





No matter which equipment you choose, you’ll be connected to a community of over 200 Cardinal Health Lab experts who are here to serve you.
To connect with an expert and discuss available instruments and financing options, scan the QR code or visit cardinalhealth.com/labcapitalequipment
References: 1. CDC. About chronic diseases. Centers for Disease Control and Prevention. Published October 4, 2024. Accessed March 13, 2025. https://www.cdc.gov/chronic-disease/about/index.html 2. Hacker K. The burden of chronic disease. Mayo Clin Proc Innov Qual Outcomes. 2024;8(1):112-119. doi: https://doi.org/10.1016/j.mayocpiqo.2023.08.005
2025 Cardinal Health. All Rights Reserved. CARDINAL HEALTH and the Cardinal Health LOGO are trademarks of Cardinal Health and may be registered in the US and/or in other countries. All other trademarks are the property of their respective owners. Patent cardinalhealth.com/patents. Lit. No. 2LAB25-3607981-01 (09/2025)
Healthcare leaders share the questions, red flags, and best practices that separate strong partnerships from risky ones.
BY R. DANA BARLOW
Choosing a third-party business partner shouldn’t boil down to healthcare supply chain leaders shaking a Magic 8 Ball – regardless of whether their questions about the contracting process generate “reply hazy, try again.”
After all, supply chain bills itself as the contracting experts within a healthcare organization – and rightly so. Through education, training and continual professional development, they (should) possess savvy, if not suitable, negotiation skills as well as communication and customer service skills that build bridges between buyers and suppliers of any product or service.
Together, the bridge building, sourcing, contract negotiating, service delivering (should) represent the modus operandi of all supply chain leaders “without a doubt.”
Naturally, the success of supply chain and its customers and business partners extend well beyond the chance, random musings of a novelty toy/paperweight –“you may rely on it.”
But building a successful partnership with a manufacturer, distributor, GPO, consultant, or service provider requires a structured process: a wellplanned introductory meeting, thorough internal vetting, and careful contract negotiations with close attention to terms and conditions.
The Journal of Healthcare Contracting checked with a quartet of seasoned supply chain leaders, well-versed in customer and supplier relations, service levels and contract management. They shared a baker’s dozen worth of key questions all supply chain professionals should ask before selecting any thirdparty business partner.
the requirements. On the other hand, a service firm such as an auditor or consultant will require a more hands-on approach as you will be tracking milestones, recommendations and possibly implementation. You will want to know their current clients and if their strategic approach is aligned with the organization.” Bryant has logged time with hospitals, hospital systems, GPOs, manufacturers and a service provider throughout her career.
Steve Downey, vice president and chief supply chain and support services officer at Cleveland Clinic, concurs that the content of deeper conversations with prospective business partners should home in on their specialties.
We ought to be fully aware of the cost-to-serve and the full end-to-end supply chain implications for that product or service that we’re contracting for. My team is making sure that all these freight elements are in place.
They acknowledge that a standard list of general questions can be helpful, but a specialized list of probing questions geared toward the business of seeking business will be more insightful and useful.
“Business type will drive what key factors come into play,” Pamela L. Bryant, senior vice president and chief supply chain officer, Parkland Health, Dallas, told JHC. “If you are working with a distributor or GPO, that partner is really focused on driving operational improvement for your organization. It is managed with [key performance indicators] and the responsiveness of the partner. This type of partnership should not take an enormous amount of time once you have established
“For distributors, questions focus on operational execution (e.g., [OnTime, In-Full] performance, ability to deliver consistently at scale, and how they handle supply disruption), which is easier to measure since metrics are hard and quantifiable,” Downey indicated. “For GPOs, they’re more nuanced since performance depends on member compliance, which they cannot fully control. Questions should probe how they drive engagement, influence members and manage compliance risks. Given our size and scale, we tend to look for GPOs to be partners on many fronts versus national agreements. For services, innovation and strategic alignment are critical. Key questions focus on whether they
will evolve with us, invest in ideation and take our ideas forward rather than remain stagnant. We also look for operational excellence, cost improvement and aligned focus.”
At Minneapolis-based Allina Health, Tom Lubotsky, vice president and chief supply chain officer,, concentrates on value as defined by the experience, service and quality the company brings to the table.
“We want to make sure we’re clear on the benefits, whether it has to do with the outcomes of quality, the experience around using that product or service or the service level requirements and how these performance metrics stand out in comparison to their competitors,” he noted. “We’re also going to focus on assurance and reliability – products or services always being there at the right time, the right place and in the right amount. Things like on-time and in-full are part of our true north metric.”
Lubotsky also homes in on a supplier’s business continuity plan. “I’m interested in their standards of resilience,” he added, “as well as understanding their background in terms of longevity and sustainability.”
Integration and openness remain key elements for Doug Pytlinski, senior vice president, supply chain, AdventHealth, Altamonte Springs, Florida.
For Pytlinski, issues around integration and openness focus on three key elements.
“How does this type of partner affect our operational control and risk profile? What internal dependencies will this partner create or expose? How transparent is this partner type’s business model?” he said.
Driving measurable savings. Building resiliency. Advancing innovation.
Premierʼs pharmacy programs go beyond contracts. With 25 - 30% greater contract coverage than competitors and a rapidly expanding technology and automation portfolio, we deliver unmatched opportunities to reduce spend, optimize margin and strengthen your pharmacy supply chain.
Market-Leading Portfolio
• 3,800+ contracted brand products and 110 suppliers.
• 60 value-add programs.
• 80% of Acute COT portfolio has Retail COT pricing.
� Premier-exclusive DSH Class of Trade: 8,116 NDCs, 95 suppliers, up to 20% savings.
Technology and Automation Expansion
Seven new categories and 25 new suppliers in 2025-2026, including those that offer drug diversion monitoring, central fill and mail order automation, revenue cycle management, IV automation, and PBM services.
Specialty and Oncology Focus Intersectta™ GPO with 110 drugs, 17 contracted suppliers and five exclusive contracts delivering average 10.7% savings.
Resiliency Leadership
Growing ProvideGx® committed drug shortage program and expanding PremierProRx® private label portfolio.
Compounding and 503B Optimization
11 contracted suppliers, 1,000+ products, ~22% savings, 503B site evaluations, product crosswalks and member collaboratives.
See how Premier delivers more ways to protect your supply chain — and your bottom line.




Blatant pitfalls, traps to avoid Pytlinski points to four key elements that must be addressed in any business relationship that can affect management and oversight. They include “overvaluing cost savings alone, committing to long-term contracts without early-out clauses or performance gates, assuming ‘big name’ equals best fit or best performance, and failing to establish a single point of ownership internally to manage the partnership,” he said.
Cleveland Clinic’s Downey warns against several issues that can pose challenges.
Cultural misalignment can undermine trust and collaboration. Unclear expectations around performance, timelines or responsibilities. Placing too much emphasis on price alone, rather than total value and failing to establish and align on key performance indicators upfront.”
best partner for your organization. Ask open-ended questions to get a better idea of how the partner would react in certain situations; this allows you to weed out the ‘fluff’ that will be included in the printed presentation.”
Even as some elements can be reasonably discoverable and rather quickly, others can be tucked into corners, contractual language or may not emerge until after the contract is signed.
Allina’s Lubotsky cites reliability in both product and service as paramount. “It’s how responsive you are, how attentive you are to what’s going on with the delivery of the service and whether it is falling short of expectations. If you want to reduce the risk of losing our business, then you just prove yourself to be more reliable,” he noted.





“Partners that promise ‘quick wins’ or easy integration without considering whether your internal data and technology capabilities can actually support it,” he noted. “Entering into a one-sided relationship where value or accountability is not shared equally is another.




“As we are all looking for ways to reduce cost, just selecting on price is not a great idea,” Parkland’s Bryant said. “In addition, just because a firm is large and well-known does not mean they are the





















Lubotsky zeroes in on freight, which tends to be a thorny issue for many supply chain leaders about where suppliers are willing to ship products and for what fees, as well as invoice accuracy to facilitate three-way matches.














































































































































































































“It’s all in the attentiveness and execution,” he said, “how fast and how well do they resolve issues. In the case of freight, these costs can add up quickly if you are not paying attention to the mode of delivery, managing expectations of when the product is really needed, and its frequency of delivery. We ought to be fully aware of the cost-to-serve and the full end-to-end supply chain implications for that product or service that we’re contracting for. My team is making sure that all these freight elements are in place. But if you’re not careful, these kinds of freight expectations can get overlooked and become costly.”



Lubotsky stresses one issue he hasn’t singled out.



















“Notice that I haven’t mentioned price,” he said. “The supplier can certainly be excluded if their price and benchmark against the industry is way off. Assuming price is competitive, then other key elements of resiliency and

















For over 140 years, Owens & Minor has navigated the ever-changing world of healthcare. We balance technology and a human touch with end-to-end expertise to help you deliver high-quality patient care. Together, we keep care moving* .
500+ product launches in 2024 | Automation and robotics | Cloud-based solutions
freight management can make the difference in choosing the right supplier.”
Four below-the-surface issues bother Pytlinski.
First is not clarifying post-sale support and escalation paths. “The partner’s ‘A team’ might disappear after the contract is signed,” he indicated.
Second, vendor lock-in or proprietary systems. “Partners that make it hard to exit or switch later (e.g., proprietary platforms, bundled contracts) can limit agility,” he noted.
Third, failing to test the partner’s responsiveness before signing. “Long response times during the sales phase may indicate future customer service issues,” he observed.
Finally, data ownership and access must be determined. “Some vendors restrict your access to usage or performance data, which can cripple insights and control,” he said.
“It will be important to fully explain your full scope of work,” Bryant advised. “Do not leave any small task to interpretation as they can spiral into larger pitfalls. Avoid providing unrealistic timelines based on your operation. Allow the partner to provide guidance but take notice if your partner agrees too quickly to the unrealistic timeline as that will probably result in change orders.”
Downey cautions against six red flags that should serve as notable warnings.
1. Overly simplified promises such as ‘We’ve integrated with xxx before, it’s easy.’ “In reality, integrations are rarely as seamless as advertised,” he said.
2. Partnerships that become static, with little emphasis on continuous improvement. “This risk often surfaces later, when one side is forced to continually push for progress.”
3. Inadequate business continuity planning, such as lacking disaster recovery or contingency measures, which increases exposure to risk.
4. Reliance on subcontractors without transparency or ongoing legal disputes with them.
5. High turnover or weak tenure within the partner’s leadership or key team members, which can destabilize the relationship.
6. Unbalanced contract terms, such as agreements that are too long without protective clauses or too short to allow for meaningful strategic initiatives, according to Downey.
Successful business partnerships are fueled by leaders and pros who clicked as well as processes that interfaced or integrated as smoothly as possible, acknowledging that hurdles and speedbumps arise. Supply chain leaders share nearly 20 bankable tips.
` Start with a shared vision and strategy in the focus area, supported by transparency on what works well and what doesn’t, according to Downey.
` “Document clear guidelines and expectations directly in the contract,” he recommended.
` “Build a collaborative relationship anchored in shared mission and goals and have those relationships up and down both organizations.
` “Continuously address deficiencies while proactively introducing new opportunities that create mutual value.
` “Implement structured governance with well-defined KPIs, including business reviews, key stakeholders and any measures clearly defined with clear data sources.
` “Ensure mutual benefit through gainsharing models and incentive alignment.
` “Define clear escalation pathways to resolve challenges quickly.”
Pytlinski emphasizes four worth implementing.
` Assign a cross-functional internal team to engage with the partner from Day 1. “This ensures the partnership isn’t siloed or overly dependent on one leader.”
` Start with a pilot or phase 1 Implementation. “A phased launch allows time to build trust, tweak the approach and scale effectively.”
` Involve the partner in outcome definition and incentive structures to build joint accountability into the relationship.
` Celebrate early wins together as this builds morale and momentum that can carry through challenges, he added.
“Understanding what differentiates your partner from their competitor allows you to leverage that skill to improve your overall operation,” Bryant advised. “It is important to go into the partnership with a win-win approach. Both sides should see value, which will drive both sides to perform. If your organization is consistently growing and evolving, be sure your partner has capacity to manage that growth. This is important as you do not want to delay your growth or have to introduce another partner to cover the additional growth. Use technology wisely and appropriately.”
Lubotsky singled out an unnamed supplier handling between $30 million to $40 million in annual business that is integrated with their health system, working directly with the appropriate business unit



leaders to provide an anticipatory as well as satisfactory level of service.
“The continuity of that relationship management is what makes them stand out and keeps them with us as a strong partner. They are accessible and transparent; they know of problems that they are trying to solve and make sure that we are informed of issues that we may not even know about. They’re forthright, and they allow us to engage with them in a corrective fashion before anything becomes a bigger problem,” he described. “They’ve got a management team that has set up the right cadence and rhythm of working with our management team and their transparency is what distinctively makes them stand out.”
we needed from this partner, and it became pretty mundane for them. However, when the pandemic came along, we really needed this partner to support us in a different way. The partner was not willing to do so as they had not positioned us as a strategic customer.
“As you can imagine, during the pandemic there was not time to argue,” she continued. “We needed to act, so we engaged with a different partner who was willing to support us in a different way. As the pandemic subsided the previous partner wanted to resume business, but we rejected that request and grew the business with the partner that had supported us when we needed it the most. The relationship
“ I have learned may lessons over the years but one of the most important has been the importance of relationships. A previous partner saw my organization as transactional and treated us as such. It was fairly consistent what we needed from this partner, and it became pretty mundane for them.”
Just as healthcare provider organizations can crow about successful ventures with suppliers who operate like true business partners, they also can lament the business relationships that soured and went awry for various reasons or never even started due to foresight.
“I have learned may lessons over the years but one of the most important has been the importance of relationships,” Bryant noted. “A previous partner saw my organization as transactional and treated us as such. It was fairly consistent what
we have with this partner is still strong and growing through collaboration and consistent communication.”
Lubotsky recalls a relationship with an unnamed service provider that deteriorated when they decided to change how they serviced the organization, which created more work for the customer.
“When you buy into a service company, you agree to the deliverable, which is what I expect you to do, but they changed the way that they did things and it really created more downstream work for us and an unreliable level of service that we had
not bargained for,” he noted. He used that experience to emphasize focusing on contract management skills.
“That’s why you need to carefully understand and negotiate terms and conditions, including exit clauses based on performance,” he continued. “It can get complicated. But the issue here was that they changed the way they delivered the service and that became untenable for us in terms of meeting our own internal dimensions of control and management to deliver care. So, we had to make a switch. We simply couldn’t work with them anymore and had to move forward.”
AdventHealth learned to assess how a partner reacts when they’re wrong, not just when they’re pitching, according to Pytlinski. “Crisis moments reveal cultural alignment more than pre-sales polish,” he said.
The provider organization also avoided a vendor who was unwilling to give them client access for reference calls. “If transparency is lacking before the contract, it will be worse after,” he warned.
The organization let go of a “good-onpaper” partner that couldn’t adapt to its internal speed and culture. “Even technically sound solutions fail when the execution tempo doesn’t match,” he indicated.
Finally, Pytlinski advises not to be seduced by slick presentations or bigbrand names. “Dig into who will actually execute and how,” he added.
“Trust your instincts,” Downey recommended. “If a partner seems to be overselling or approaching problems the wrong way, it’s often a sign the partnership isn’t the right fit. A partnership cannot succeed if the third party is focused only on their own goals rather than shared success.”
Healthcare-grade chairs.
Commercial disinfectants.
Breakroom snacks.
Keep your practice running smoothly through flu season and beyond with corner-to-corner solutions from the waiting room to the back o ce so you can focus on your patients.

GPO member savings for the best pricing available.

How supply chain solutions can take administrative load off frontline staff in the non-acute care setting, enabling clinicians to spend more time on patient care and less on managing supplies.
As care continues to migrate away from hospitals and patient volumes rise across non-acute settings, the demands placed on clinical staff have grown exponentially.
While health systems often invest heavily in acute care supply chain infrastructure, the same attention is rarely given to nonacute sites. “It’s fragmentation at scale,” said Dan Young, Sr. Manager, Supply
Chain Services & Sales for Henry Schein. “A system might have 1,200 distributed sites but doesn’t have the scale to justify big investments in internal resources or expensive systems.”
In physician practices, urgent care centers, and other non-acute care settings, clinicians are often pulled into tasks that have little to do with patient care: receiving packages, breaking down boxes, or
searching storerooms for missing items. These seemingly minor tasks add up quickly, draining valuable time and creating inefficiencies that ripple through the entire care experience.
“Clinicians go to school and are licensed to be patient-centric,” Young said. “But because everyone’s running so lean, support services are often limited. That can lead to clinicians being asked to handle ordering, restocking, and other tasks that aren’t core to patient care. None of that time is spent with patients.” Young said. The consequences are significant: longer wait times, exam rooms tied up



As care expands beyond the hospital walls, inefficiency follows often in the form of clinical staff performing supply chain tasks From ordering and receiving to stock counts and troubleshooting backorders, this misalignment drains time, productivity, and resources
Henry Schein helps health systems reclaim that time. As a trusted distribution partner and strategic advisor, we bring the tools, technology, and expertise to streamline non-acute supply chain operations—reducing costs, improving visibility, and allowing clinicians to focus on what matters most: patient care.
With the right partnership, your non-acute network runs smarter, faster, and more efficiently

Discover where inefficiency hides and how to fix it.
Scan to download Fixing the Gaps in the Non-Acute
Supply Chain: 6 Strategies to Uncover Hidden Costs
Building a Smarter, Better, Faster, Supply Chain, Together!
Visit us nline t henryscheinmedical.com/optimize
Sponsored Henry Schein
while staff may be hunting for supplies, ordering products or managing inventory.
“If you’ve got a system with 200 sites, and a clinician is spending an hour a week on these tasks per site, that’s 200 hours a week—five FTEs—dedicated to non-patient activity,” Young explained. “It becomes much more than just a product issue. It’s a process issue.” It is paramount to understand the inefficiency this is driving today, so it can be addressed, and you can focus on being more profitable tomorrow.
These responsibilities not only create delays for patients but also add stress to an already demanding workload. “In our experience—talking to providers and walking their facilities—we’ve found one of the biggest drivers of clinical staff dissatisfaction is having to manage supply chain activities,” Young said.
Patients feel the downstream effect: instead of being greeted promptly or engaged meaningfully, they’re left waiting while staff troubleshoot supply problems. Over time,
this erodes both patient experience and productivity—fewer patients seen, less revenue generated, and greater staff burnout.
Young stressed that Henry Schein is not approaching these challenges from a transactional standpoint. “We want to understand our customers’ business objectives—whether it’s dealing with staffing shortages, making their practice more attractive to private equity, or improving revenue— and further align on where we can support them in achieving their goal. We want them to view us not as just a distributor, but as a strategic partner who can help eliminate the hidden cost of inefficient supply.”
Although supply chain technologies have their place in the non-acute space, their cost often outweighs the benefit for smaller or decentralized sites. “Our approach is to first address customers’ supply chain processes before evaluating technology,” Young said. “That allows us to fix the root cause. Once the right processes are in place, we can determine what type of technology adds value.”
` Inefficient supply chain tasks pull clinicians away from patients, creating delays, stress, and lost revenue.
` Streamlined processes and practical tools often provide more value than expensive, complex technology.
` Non-acute care settings need customized supply chain solutions tailored to their distributed, resource-limited environments.
He added, “Cookie-cutter models don’t work in this space. Every non-acute location operates like a mini business with its own nuances. The solution must be nuanced as well.”
Instead of pushing one-size-fitsall systems, Henry Schein focuses on optimizing processes and implementing practical technology to streamline ordering, approvals, and replenishment. “Any solution must be anchored to the customer’s business objectives,” Young emphasized. “It’s not about the flashiest technology—it’s about putting nurses back in front of patients and achieving sustainable, measurable savings.”
Henry Schein is uniquely positioned to help customers identify and implement sustainable supply chain processes that support an optimal work environment, enabling clinicians to focus on patient volume, flow, and most importantly, care.
As health systems balance cost pressures with the need to improve care, non-acute sites represent both a challenge and an opportunity. With the right supply chain partner, clinics can reduce administrative burdens, increase staff satisfaction, and unlock capacity to see more patients.
“We’re not your typical distribution partner,” Young said. “We want to help our customers run more efficiently, better utilize their workforce, improve revenue, and create happier employees.”
By rethinking supply chain processes—and partnering with experts who understand the non-acute environment— health systems can ensure clinicians spend less time managing boxes and more time delivering the care that matters most.
The challenges facing rural healthcare and potential policy solutions.
BY JENNA HUGHES
Nearly 46 million people in the U.S. live in rural areas, and roughly 77% of rural counties in the U.S. are considered healthcare deserts, or geographic regions where residents face significant barriers to healthcare access, according to the National Rural Health Association (NRHA).
There are numerous ways to define rural health. The federal government designates more than 70 different ways of defining rural health across various agencies.
NRHA, a national membership organization that represents more than 90% of the nation’s rural hospitals, rural health clinics, and rural community health centers, strongly recommends that definitions of rural be specific to the purposes of the programs in which they are used, and that they are referred to as programmatic designations and not as definitions.
“At NRHA, we define rural America as a place where those most in need of healthcare services often have the fewest options available to access that care,” said Alan Morgan, Chief Executive Officer of NRHA. As CEO, Morgan oversees the organization’s educational, program and policy activities.
NRHA aims to address rural health challenges by identifying best practices, sharing those best practices for replication and working through legislation and regulation to remove barriers to expanding them.
“NRHA has stayed true to the same mission for more than 40 years –promoting leadership and developing healthy rural communities both for the health system and for healthcare delivery,” said Morgan.

There are underlying similarities in healthcare access challenges among those living in rural America, regardless of location. These include workforce shortages, greater distances for patients to be able to seek care between access points, and significant health disparities.
“It is not unusual to have a life expectancy among rural populations that are 20 years less than their urban
counterparts,” said Morgan. “It is unacceptable that an individual’s length and quality of life is determined simply on where they live.”
Another issue is distance. Rural residents tend to travel farther to access care than urban residents.
“Where we find the greatest disparities among urban and rural populations is within behavioral health, maternity care, pharmacy access, long-term care, and more,” said
Morgan. “This is due to fewer providers available, a culture that doesn’t always embrace behavioral health, distance from care, and higher rates of economic and community pressures than in urban areas.”
“Maternity deserts found in rural America are also substantial, and if a community lacks access to proper maternity care, young families will not be able to move there,” said Morgan.
Women in rural areas experience markedly higher rates of maternal morbidity and mortality due to lack of access to consistent maternity care, reproductive services, and postpartum support, according to the Rural Health Information Hub.
Rural community pharmacies also face many challenges to staying open, including low volume purchasing, slim profit margins, unfavorable insurance practices, and a limited pharmacy workforce.
“Over the last 15 years, more than 1,000 rural pharmacies have closed across the U.S., and more than 500 rural nursing homes have closed over the past decade,” said Morgan.
The loss of vital health services in these locations results in reduced access to care, increased healthcare costs, and significant economic strain withing rural communities.
Another challenge facing rural America is the widespread closure of hospitals and
emergency rooms, a trend that threatens not only access to essential medical services but also the overall stability of rural communities – impacting emergency care response times to local economies and population health outcomes.
Since 2010, nearly 190 rural hospitals have shut their doors or discontinued inpatient services, according to NRHA. Nationally, nearly 50% of rural hospitals are operating with negative margins and are therefore vulnerable to closure.
“Rural hospitals are closing not because of low patient volumes or because people are moving out of rural America,” said Morgan. “Small rural hospitals are closing today because they have a disproportionate share of patients with high health needs and the inability to pay for that care, and bad debt is the reason these hospitals are closing across the U.S.”
When a rural hospital closes, not only does the community lose access to accessible health care, but a major employer and community cornerstone ends, affecting the community at large.
“The problem when you lose a rural hospital is that you lose an anchor institution, a point of care, and in many cases the largest employer in the county,” said Morgan. “When a rural hospital closes, often the community follows. You lose the direct jobs in the hospital; you lose the indirect jobs that support healthcare. It is
About 77% of rural U.S. counties are healthcare deserts, facing severe challenges like workforce shortages, long travel distances for care, and lack of access to services such as maternity care, behavioral health, and pharmacy support. These disparities often result in significantly lower life expectancy for rural residents compared to urban populations.
tough to quantify the loss of individuals that leave or do not move to the community because they don’t have access to 24/7 emergency room service care.”
Addressing the rural healthcare crisis requires a variety of tactics, including telehealth, incentivizing healthcare providers to work in rural areas, the use of artificial intelligence, and strengthening state and federal funding for rural healthcare facilities.
One of the major reasons for rural hospital staffing issues is a lack of incentives for recent graduates to move to rural areas for work.
“Fewer than 4% of the nation’s incoming medical students come from rural America. Upper income urban students are going to school in urban areas, being trained in urban areas, and do their residency in urban areas,” said Morgan.
Training physicians in rural areas through rural residency programs not only provides greater access to care for rural communities, but also increases the likelihood of physicians practicing in rural parts of the country, according to the Health Resources & Services Administration
“Rural residency training programs serve to attract rural kids with academic instructors that are passionate about healthcare in rural America, and these students are more likely to end up staying and practicing in rural areas,” said Morgan.
Addressing workforce shortages also requires the introduction of technological solutions to ease patient load and administrative burdens on existing staff.
“Telehealth and telemedicine are also a great solution that’s successfully working within rural areas to address
workforce shortages,” said Morgan. “Additionally, Artificial Intelligence (AI) technology is increasingly being used for documentation, coding, and other administrative functions, freeing up staff time from nurses to clinicians to admin staff, and has had a real beneficial impact very quickly in rural communities”
Yet another obstacle facing rural Americans is patients needing to travel to receive healthcare. Often, residents in remote areas may have to travel significantly farther distances than those in urban communities to show up to in-person care.
Providers have increasingly relied on solutions like telehealth and AI to allow for more patient-facing time for rurally located, eliminating the burden of frequent travel for many residents with travel barriers.
“Telehealth is a great tool to expand primary care, but never a replacement for primary care,” said Morgan. “We must find the happy medium as to how we utilize technology to address workforce shortages without utilizing technology to eliminate any points of access to care that are currently there.”
Collaboration among healthcare providers, community organizations, government agencies and educational institutions is crucial to developing and implementing policy changes that benefit communities facing location-based health disparities.
“Federal, state, and local policy leaders must be good partners with local healthcare because in many cases, they are the payors for this healthcare,” said Morgan.
“At NRHA, our partnerships with Group Purchasing Organizations
Closures threaten rural communities
Since 2010, nearly 190 rural hospitals have closed, primarily due to financial instability, not lack of demand. These closures remove vital access points for healthcare, eliminate key employers, and contribute to the economic decline and depopulation of rural communities.
(GPOs), technology companies, and medical device companies are incredibly valuable because they bring the realworld data from their customers and we’re able to make a strong policy case on the implications of adverse policies,” said Morgan.
NRHA’s advocacy policies include investing in a strong rural healthcare infrastructure, reducing rural healthcare workforce shortages, and building rural health opportunities.
“Promoting a policy approach that keeps Americans healthy and out of hospitals in the first place, and promoting a public health wellness approach across communities helps both patients and providers, and is the first step to a healthier nation overall,” said Morgan.
The challenges associated with rural healthcare delivery often require physicians and health systems to find creative approaches to continue delivering patient care. Hundreds of towns across the
U.S. are currently serving as ‘innovation hubs,’ or healthcare settings stretched thin that are consequently fostering collaboration and innovation; and these places are having a significant impact on the redesign of the nation’s healthcare system as a whole.
“All of the innovative, creative things that are happening within healthcare delivery and policy today are beginning in small towns across America,” said Morgan. “If you want to see what the healthcare system is going to look like 20 years from now, visit any small town today and you will see coordinated care, an emphasis on primary care, the use of community healthcare workers as a bridge between the community and providers, telehealth use, and AI technology solutions. The rural health system is stretched to the max with high health needs and low reimbursement, but through creative approaches these physicians are making it work.”
The National Rural Health Association (NRHA) promotes solutions such as rural medical training programs, telehealth, AI tools, and public policy reforms. Innovation is emerging from rural “healthcare hubs” that are finding creative ways to deliver care despite limited resources, helping shape the future of U.S. healthcare.
In 2019, The Queen’s Health Systems (QHS) in Hawaii, one of the state’s largest employers with four hospitals and more than 70 care sites, faced a daunting challenge. Its longtime medical librarian was preparing for retirement, and leadership quickly realized that replacing such a critical role would not be easy. The Hawaii Medical Library, serving the entire system, provided clinicians and staff with the evidence-based resources they needed to deliver exceptional care. Losing that support would have left a gap at the heart of QHS’s mission.
After exploring options, QHS turned to HPC International, Inc., whose HPCLibrarian™ solution offered a turnkey approach to medical library management. What began as a project-based collaboration soon transitioned into a fully outsourced service model, ensuring a seamless handoff as the in-house librarian retired. Within weeks, HPC assumed management of the Hawaii Medical Library, providing QHS with a team of expert librarians rather than relying on a single point of expertise.
The results were transformative. Instead of higher costs that typically come with organizational growth, HPC achieved a 19% reduction to the library’s budget, even as the system expanded bed count, admissions, and employee headcount from 2020 through 2024. HPC accomplished this by renegotiating vendor contracts, consolidating subscriptions, and replacing underutilized resources with higher-value alternatives. Additionally, as a Vizient GPO contract supplier, HPC helped QHS capture member rebates not available through direct hires.
Beyond savings, HPC’s model expanded access and coverage. QHS staff now benefit from seven-day-a-week support, including evenings and weekends, ensuring critical information is always within reach. The cloud-based transition of the library website provided clinicians with remote access to resources, while ongoing training sessions and workshops helped nurses, physicians, and researchers strengthen their skills in evidence-based practice.
Former QHS Vice President of Native Hawaiian Affairs & Clinical Support, Dr. Gerard Akaka, reflected on the impact:
“This was the best decision as we benefited from their expertise, experience and, importantly, management of our budget through strategic curation of subscriptions. In the past, we had one librarian who wasn’t available when on PTO. Now we have coverage 7 days per week throughout the year. My experience with HPC has been excellent and I highly recommend them.”
Now in its sixth year of service, the HPC partnership continues to provide QHS with scalable, cost-efficient library management that evolves with the system’s needs. For hospital leaders facing librarian retirements, staffing gaps, or the challenge of modernizing resource management, QHS’s experience demonstrates how outsourcing can preserve access to knowledge, strengthen clinical support, and ensure financial sustainability.
A new approach to managing your medical library that’s cost-effective and drives savings while providing the vital research support your hospital staff depend on.
HPCLibrarianTM is a one-of-a-kind service for hospitals and health systems nationwide in need of medical librarians.
HPC librarians have a proven track record of successfully:
` Managing institutional libraries
` Overseeing library subscription renewals
` Negotiating the costs of library resources
` Building virtual library websites
` Providing research support to staff 7 days a week to fuel evidence-based practice and ensure compliance with healthcare accreditation guidelines and professional development requirements.
HPCLibrarianTM brings the expertise and know-how necessary to support your library with no training needed.
HPC can provide specialized support to expand your existing librarian team, or you can fully transition all responsibilities and operational oversight to HPC’s librarians who work remotely to support your staff in a virtual model.

33.3% Amazing and underappreciated resource. Makes lit review and access to scholarly articles very easy. Thank You!
A recent survey of library patrons using HPCLibrarian TM were asked how they benefited from the information provided by their HPC librarian:
62.5% Changed a clinical decision
Validated a clinical decision


All from a single source.
Running an orthopaedic trauma service never slows down. Every choice—from patient care to inventory and cost control—shapes outcomes. That’s why we created Alliance, a value-added program designed with trauma care at its core.
Alliance simplifies trauma procurement by connecting patient care and supply chain management. You can pick the right blend of strategic contracting, inventory management, education, and implementation support to fit your service line, giving you flexibility and control from the start.


Alliance helps you take control of trauma care in ways you’ll wonder how you ever managed without.
Maximize contract value with options that drive compliance, enhance savings, and ensure you’re getting the most from your agreements -- all while simplifying purchasing.
Gain a clear view of your trauma service line with easy-to-understand data helping you to optimize spend and uncover opportunities to improve efficiency and outcomes.
Flexible financing solutions that help you acquire essential trauma equipment today while preserving cash flow for the future, so financial constraints don’t slow down patient care.
From planning to execution, our project management team helps streamline transitions, align key stakeholders, track compliance, and provide real-time guidance.
Take charge of your inventory with tailored solutions that maximize value, reduce waste, and right-size your inventory to ease space and sterile processing constraints.
Our trauma experts work alongside you to develop individualized strategies, tackling your biggest challenges with solutions designed to fit your team’s unique needs and goals.


Why can’t supply chain’s relationship with clinicians be like playing Tetris?
BY R. DANA BARLOW
Unfortunately, conversations can become contentious, regardless of industry, profession or social/societal clique. In healthcare administration, finance and operations, which extends to supply chain, contentious conversations occur with payers, service companies, suppliers and even within the walls of the organizations themselves as polarization can infect departments and specialties.
External politics aside, this issue taps into internal corporate and economic influence as one group within an organization may seek and strive to gain some advantage over another. While that may seem overly simplistic, it’s not wholly unrealistic. Participants tend to approach these conversations motivated by a sporting mentality (some may call it adversarial) that generates one obvious outcome – a winner and a loser. This continues to occur between and within healthcare organizations throughout the nation, regardless of the parade of educational conference and trade show keynotes and learning labs, media essays, opinion columns and news reports about the need for collaboration, cooperation and that old game theory concept of “coopetition,” a cleverly created term that fuses cooperation with competition much like those Hollywood conceits that merge the first names of celebrity couples for publicity and ratings.
Coopetition generally refers to interorganizational participants collectively working together for the benefit of a larger process or system while competing individually for customer interest and market share. Think Coca-Cola and Pepsi “teaming up” to ensure the survival and success of the multibillion-dollar soft drink segment of the beverage industry as “healthier” options allure consumer interest and purchasing power while also beating each other up over brand preference and consumer favor.
In healthcare, supply chain’s contract negotiations with suppliers are supposed to be tough so that each side can collect a win or two as they navigate through the emotional rapids, bobbing and weaving to generate a long-term professional relationship.
Supply chain’s conversations with clinicians – surgeons, physicians and nurses – shouldn’t be so tough. After all, both groups play on the same team, right? And they’re playing to achieve a common goal – not a win for either side, but a win for the patient, their mutual customer.
Alas, too often the conduct and conversations between the clinical community and supply chain resembles what we see in professional sports, football and basketball, in particular. Disgruntled “star” athletes grapple with performing on teams that just can’t seem to get into the playoffs year after year so they grumble for a trade to a team with a better record – or in this analogical case to a healthcare organization that will provide them what they want.
Perhaps Mark F. Dozier, associate vice president, supply chain services, strategic sourcing and engagement, HonorHealth, encapsulates the healthcare mindset best in this edition’s clinician-supply chain conversation story.
economically trained and degreed clinicians who care about the health of the organizations. In short, one needs the other and vice versa to care for patients. Clinicians need hospitals and other healthcare facilities in which to practice medicine. Without them, where would they practice? Clinicians need supply chain to bring in products and services. Without supply chain, how would clinicians obtain products and services (cost effectively)? Without products and services, how would clinicians work on patients? If healthcare providers cannot control budgets and expenses to the point that they have to cease operations, where would clinicians practice?
Call it a daisy chain linked at the intersection of common sense, historical experience and wisdom.
Over the decades, clinical and supply chain players have hemmed and hawed on how to work together with options spanning a variety of demands and offerings from the simple to the
“Supply chain is focused on the health of the hospital system. Clinicians are focused on the health of the patient. These two perspectives do not always meet.”
“Supply chain is focused on the health of the hospital system. Clinicians are focused on the health of the patient. These two perspectives do not always meet,” Dozier noted.
What a profound overarching observation that highlights the underpinnings of a selfish and superficial attitude. For the record, there are plenty of supply chain professionals who care about the health of the patient just as there are
complex. Clinicians may want access to what they used in medical school or later in residency. Or maybe they contributed to the design and production of a product or invested in the manufacturer. Or maybe they favor a particular manufacturer rep. Some want to be brought into the product assessment/evaluation process much earlier –say, initial discussions and sourcing pool forward through value analysis.
Not surprisingly, a typical reaction involves clinicians accusing supply chain of contracting for the cheapest products that don’t provide the desired benefits for their patients.
Those in supply chain who eschew adversarial relationships employ a few strategies and tactics to facilitate conversation and elicit cooperation. Chief among them: Collecting and sharing accurate procedural data. Another is gainsharing where supply chain can apply any contractual cost savings achieved to funding for cliniciandesired products and technology.
If someone wants something else because of some distinctiveness, we ask whether the product we have on hand is something they can live with. You have to meet halfway because it’s our economic reality. If their comfort level is how they were trained in what they were using, then we have to work a little bit harder with the physician because you can’t keep inviting variation. It’s just too costly. It’s something that collectively both supply chain and the clinical leaders have to work on together.”
Another popular strategy is recruiting a physician/surgeon champion to “ride
If someone wants something else because of some distinctiveness, we ask whether the product we have on hand is something they can live with. You have to meet halfway because it’s our economic reality.
One idea shared by a supply chain executive a few years back seemed at the time enterprising and innovative on the front end, but dangerous on the back end. If a clinician favored a product or technology not on contract that was more expensive than the contracted item, then supply chain would agree to contribute the price of the current product under contract, leaving the clinician to foot the bill for the difference.
Tom Lubotsky, vice president and chief supply chain officer, Allina Health, doesn’t find that viable at all.
“You wouldn’t make exceptions for one doctor who is trained differently or who prefers a set of instruments,” he countered. “All those other doctors doing the same procedure may be comfortable using a certain product we make available.
herd” or appointing/employing a “medical director of supply chain.” This can be a practicing doctor on staff or someone with a medical degree and training who can talk the talk and walk the walk with clinical peers. [See “Physician/ Surgeon-Supply Chain Relations Fueled by Circle of Trust,” September 2024
The Journal of Healthcare Contracting.] Lubotsky agrees that medical directors can be the bridge needed to connect the dots and link the two mindsets.
“When we can’t reason with a clinician about a specific product or device or preference, the medical director has the clinical knowledge or knows who to go to manage the process of acceptability,” he said. “They can work with them. They can talk in their language. They
can challenge them where they feel that they’re not being reasonable in terms of their request. The peer-to-peer relationship is huge.
“I couldn’t carry out some of our discussions about the variation of management and use and the variation of different suppliers we have for the same products without a medical director’s engagement and help,” Lubotsky continued. “But it’s not just the medical director of supply chain. It could be a physician champion of that specific service. In some instances, it could be the administrator of that service line that comes in and helps out.” He adds that these team members represent “where true clinical integration comes together because then you can manage these relationships and these processes much more effectively.”
Lubotsky acknowledges that not everyone has the resources to employ a dedicated medical director of supply chain, whether full-time or part-time, but some kind of physician or service line leader can make all the difference.
Ultimately, clinicians and supply chain need to be using the same playbook as teammates. Think of it as playing the video game Tetris. Each participant is a different shape that can fit together in tight links. When these shapes fill a complete line, then the line disappears, which earns points toward increasing your score. Think of the lines as challenges to be overcome. Working together eliminates the challenges so that you both succeed for the good of the organization and the patient – not necessarily in that order.
R. Dana Barlow serves as a senior writer and columnist for The Journal of Healthcare Contracting. Barlow has nearly four decades of journalistic experience and has covered healthcare supply chain issues for more than 30 years. He can be reached at rickdanabarlow@wingfootmedia.biz





Medegen is the U.S. manufacturer of Bedside Products and core EVS Products delivering:
RELIABLE SUPPLY CHAIN: Stronger, shorter supply lines for critical essentials.
REGULATORY CONFIDENCE: Compliance with FDA and U.S. safety standards.
FAST DELIVERY: Quick domestic turnaround gets orders to you sooner.
PROVEN QUALITY: Made to rigorous U.S. manufacturing standards.
BUILT FOR AGILITY: Rapid response to urgent needs and custom requests.
ECO-SMARTER: Shorter transport means lower environmental impact.
MADE IN AMERICA: Supporting U.S. jobs and communities.

Mayo Clinic awarded up to $40 million by ARPA-H for pioneering air safety research
Mayo Clinic has been selected to lead a groundbreaking research project focused on improving indoor air quality and safety in healthcare settings by the Advanced Research Project Agency for Health (ARPA-H). The project, part of the ARPA-H BREATHE program, aims to develop new ways to monitor and improve air in real time, helping protect public health in buildings nationwide.
Through the HAIQU project, Mayo Clinic will introduce cutting-edge biosensors, artificial intelligence and smart air filtration systems in emergency departments across Mayo Clinic’s campuses in Florida, Arizona and Minnesota. These innovative technologies work together to enhance air quality by proactively monitoring the environment, assessing potential risks and automatically improving air safety when needed – creating healthier spaces for patients and care teams alike.
The work is directly aligned with the design priorities of Bold. Forward. Unbound., which emphasizes clean, flexible and intelligent environments to support optimal healing.
As part of the AHA’s long-standing commitment to helping hospitals and health systems defend against and deflect cyberattacks, the AHA and Microsoft announced several new and updated offerings as part of the Rural Health Resiliency program. The program offers free and discounted services to eligible rural hospitals, including Critical Access Hospitals and Rural Emergency Hospitals. Among the offerings are free cybersecurity assessments, cloud capability evaluation, curated cyber and artificial intelligence training and foundational cyber certifications for rural hospital information technology staff.
The Northwell Cancer Institute unveiled its Center for Women’s Cancer at the R.J. Zuckerberg Cancer Center . The $14 million, 21,000-square-foot facility is Long Island’s first dedicated cancer center for women, representing a major transformation in delivering specialized care at every stage. The outpatient center integrates breast surgery, gynecologic oncology, medical oncology and comprehensive support services in a single location, addressing the interconnected nature of women’s cancer risks and providing services focused on women and their unique care needs.
The Center for Women’s Cancer addresses a critical gap in cancer care delivery by recognizing the genetic and clinical connections between breast and gynecologic cancers, particularly for patients with BRCA gene variants and other hereditary cancers. This integrated approach positions Northwell at the forefront of precision oncology for women.
In the August 2025 edition of The Journal of Healthcare Contracting, the story, “CSC Turns: The Highs, Lows, Sighs and Woes,” listed Ryan Rotar as Executive Director, Supply Chain, at UNC Health, before he left for Tecsys. While Rotar did serve in that role at UNC Health for several years, his title before leaving for Tecsys was Director of Information Technology – ERP Systems at UNC Health.

Empower your team to work more efficiently and collaborate seamlessly at the point of care with the Midmark Digital ECG.
With optional DICOM compatibility, you can securely share ECG data with cardiology specialists via their preferred CVIS—right from your EMR. This supports fewer manual steps, faster turnaround and more accurate test results without disrupting your workflow.
It’s an opportunity to strengthen the connection between your team and your patients— transforming every data point into a clearer picture of health and every interaction into better care.
View product info at: midmark.com/ecg-jhc
Scan to see the Midmark Digital ECG.

The Share Moving Media team appreciates all of our loyal readers and advertisers.
We are truly thankful for the wonderful industry we have the privilege to serve.
